You might also like
- Pure Bodybuilding Phase 2 - Hypertrophy HandbookDocument53 pagesPure Bodybuilding Phase 2 - Hypertrophy HandbookLaura Duff100% (1)
- Kryptonian Muscle Gain SystemDocument86 pagesKryptonian Muscle Gain SystemTrading Solutions100% (3)
- Koda Workout Plan Ebook (10) 2Document62 pagesKoda Workout Plan Ebook (10) 2tomNo ratings yet
- An Essential Guide To VBTDocument21 pagesAn Essential Guide To VBTLino DélcioNo ratings yet
- The Compiled Work of Charles Poliquin by Gregory TaperDocument25 pagesThe Compiled Work of Charles Poliquin by Gregory TaperZachary LeeNo ratings yet
- Full Body Training V2: The Intermediate ProgrammeDocument44 pagesFull Body Training V2: The Intermediate Programmemstephen2448100% (2)
- Book of Programmes for the Team Sport Athlete; Size & StrengthFrom EverandBook of Programmes for the Team Sport Athlete; Size & StrengthNo ratings yet
- JEP Journal of Exercise Physiology: Online OnlineDocument17 pagesJEP Journal of Exercise Physiology: Online OnlineTomas Rivera100% (2)
- 14 CPFI Tri-SetDocument6 pages14 CPFI Tri-SetjoaoevandroNo ratings yet
- Comparisons Between Twice-Daily and Once-Daily Training Sessions in Male Weight LiftersDocument11 pagesComparisons Between Twice-Daily and Once-Daily Training Sessions in Male Weight LiftersMatheus AguiarNo ratings yet
- 3sets TrainingDocument5 pages3sets TrainingNeuNo ratings yet
- Concurrent Resistance and Endurance Training Influence Basal Metabolic Rate in Nondieting IndividualsDocument6 pagesConcurrent Resistance and Endurance Training Influence Basal Metabolic Rate in Nondieting IndividualsRui CunhaNo ratings yet
- Schoenfeld 2015Document9 pagesSchoenfeld 2015GutoGonçalves100% (1)
- Defreitas 2010Document7 pagesDefreitas 2010Fabiano LacerdaNo ratings yet
- Polarized Training-Intensity Distribution Leads To Greater Physiological and Performance AdaptationsDocument11 pagesPolarized Training-Intensity Distribution Leads To Greater Physiological and Performance AdaptationsLeonardoValenzuela0% (1)
- Running Head: Neither Load Nor Hormones Determine HypertrophyDocument32 pagesRunning Head: Neither Load Nor Hormones Determine HypertrophyMarcelo NorisNo ratings yet
- 07 - JSCR - Effect of Short Term Equal Volume Resistance Training With Different Workout Frequency On Muscle Mass and Strength in Untrained Men and WomenDocument4 pages07 - JSCR - Effect of Short Term Equal Volume Resistance Training With Different Workout Frequency On Muscle Mass and Strength in Untrained Men and WomenEmerson AlissonNo ratings yet
- A Genetic-Based Algorithm For Personalized Resistance TrainingDocument10 pagesA Genetic-Based Algorithm For Personalized Resistance TrainingFabiano LacerdaNo ratings yet
- Core StiffnessMcGill 2015Document12 pagesCore StiffnessMcGill 2015Hugo TintiNo ratings yet
- Progressive Resistance Training Volume Effects On.2 PDFDocument8 pagesProgressive Resistance Training Volume Effects On.2 PDFPabloAñonNo ratings yet
- Can Creatine Supplementation Interfere With Muscle Strength and Fatigue in Brazilian National Level Paralympic Powerlifting?Document12 pagesCan Creatine Supplementation Interfere With Muscle Strength and Fatigue in Brazilian National Level Paralympic Powerlifting?Rodrigo SampaioNo ratings yet
- Effect of Training Cessation On Muscular Performance A Meta AnalysisDocument10 pagesEffect of Training Cessation On Muscular Performance A Meta AnalysisGutoGonçalvesNo ratings yet
- Os Efeitos de Adicionar Exercícios Uniarticulares A Um MultiarticularDocument5 pagesOs Efeitos de Adicionar Exercícios Uniarticulares A Um MultiarticularThiago SartiNo ratings yet
- Effect of Training Cessation On Muscular Performance: A Meta-AnalysisDocument10 pagesEffect of Training Cessation On Muscular Performance: A Meta-AnalysisLuiz Eduardo RodriguesNo ratings yet
- Moderators of Strength Gains and Hypertrophy in Resistance Training: A Systematic Review and Meta-AnalysisDocument11 pagesModerators of Strength Gains and Hypertrophy in Resistance Training: A Systematic Review and Meta-AnalysisJoão Rangel MiguelNo ratings yet
- Pattison 2020Document6 pagesPattison 2020caio personalNo ratings yet
- Maximizing Muscle Hypertrophy A SystematicDocument16 pagesMaximizing Muscle Hypertrophy A SystematicFabri DisandroNo ratings yet
- Effects of Creatine Supplementation On Body Mass and Muscle Girths in BodybuildersDocument4 pagesEffects of Creatine Supplementation On Body Mass and Muscle Girths in Bodybuildersmarcopulv19No ratings yet
- Efectos de Un Programa de e Volumen Aleman Modificado Sobre La Hipertrofia y Fuerza MuscularDocument11 pagesEfectos de Un Programa de e Volumen Aleman Modificado Sobre La Hipertrofia y Fuerza MuscularFabri DisandroNo ratings yet
- The Effect of Training Volume and Intensity On ImDocument4 pagesThe Effect of Training Volume and Intensity On ImCAMPERNo ratings yet
- Revision SistematicaDocument7 pagesRevision SistematicaCarolina SandovalNo ratings yet
- Brazilian Journal of Physical TherapyDocument10 pagesBrazilian Journal of Physical TherapyMARIA RESENDENo ratings yet
- Jenkins2017.PDF Treino de ForçaDocument15 pagesJenkins2017.PDF Treino de ForçaAnderson TeixeiraNo ratings yet
- Ogasawara Et Al. 2012Document4 pagesOgasawara Et Al. 2012clincursoNo ratings yet
- A Systematic Review, Meta-Analysis and Meta-Regression of The Effect of Protein Supplementation On Resistance Training-Induced Gains in Muscle Mass and Strength in Healthy Adults - 376.fullDocument11 pagesA Systematic Review, Meta-Analysis and Meta-Regression of The Effect of Protein Supplementation On Resistance Training-Induced Gains in Muscle Mass and Strength in Healthy Adults - 376.fullAlexandre ReisNo ratings yet
- 2014 - Villanueva Et Al - Creatine SupplementationDocument15 pages2014 - Villanueva Et Al - Creatine SupplementationKurnia Maratus SolichahNo ratings yet
- 10 1 1 811 366 PDFDocument7 pages10 1 1 811 366 PDFbookslolNo ratings yet
- Effects of A 12 Week Strength Training PDocument10 pagesEffects of A 12 Week Strength Training PSamehAlyNo ratings yet
- Clinical Nutrition: Randomized Control TrialsDocument8 pagesClinical Nutrition: Randomized Control TrialsteresaNo ratings yet
- The Effects of Traditional Superset and Tri-Set ReDocument13 pagesThe Effects of Traditional Superset and Tri-Set ReMarcel GomesNo ratings yet
- Documento Senza TitoloDocument106 pagesDocumento Senza Titolothommygym08No ratings yet
- Fphys 07 00487Document16 pagesFphys 07 00487NICOLÁS ANDRÉS AYELEF PARRAGUEZNo ratings yet
- Absctrac Congreso NSCADocument144 pagesAbsctrac Congreso NSCAMelina LabroneNo ratings yet
- Neuromuscular Training Improves Performance On The Star Excursion Balance Test in Young Female AthletesDocument8 pagesNeuromuscular Training Improves Performance On The Star Excursion Balance Test in Young Female Athletesrduran621679No ratings yet
- Effects of Different Volume-Equated Resistance Training Loading Strategies On Muscular Adaptations in Well-Trained MenDocument11 pagesEffects of Different Volume-Equated Resistance Training Loading Strategies On Muscular Adaptations in Well-Trained Menjoaoevandro100% (1)
- ResearchDocument29 pagesResearchEijunNo ratings yet
- Continous Vs CyclicDocument11 pagesContinous Vs CyclicGál Bence SzabóNo ratings yet
- Exploring The Dose-Response Relationship Between EDocument55 pagesExploring The Dose-Response Relationship Between EnazireunvNo ratings yet
- 2019 - Myofibrillar Protein Synthesis and MuscleDocument10 pages2019 - Myofibrillar Protein Synthesis and MuscleDiego Duarte CavalcanteNo ratings yet
- Strength Training Basics LEERDocument8 pagesStrength Training Basics LEERbichofoodNo ratings yet
- Tabla Periodica OrtografiaDocument10 pagesTabla Periodica OrtografiacsolismNo ratings yet
- 2009 - Bemben Et Al - Creatine SupplementationDocument5 pages2009 - Bemben Et Al - Creatine SupplementationKurnia Maratus SolichahNo ratings yet
- Hipertrofia EstrategiasDocument15 pagesHipertrofia EstrategiasvicenteNo ratings yet
- Paz Et Al. 2019 - CIrcuit, Paired Set and Trad J Sports Med Phys FitnessDocument12 pagesPaz Et Al. 2019 - CIrcuit, Paired Set and Trad J Sports Med Phys Fitnessjk trainerNo ratings yet
- A Minimal Dose Approach To Resistance Training For The Older AdultDocument7 pagesA Minimal Dose Approach To Resistance Training For The Older AdultThalesNo ratings yet
- Comparison of The Effects of Velocity Based Vs Traditional Resistance Training Methods On Adaptations in Strength Power and Sprint Speed A SystematicDocument16 pagesComparison of The Effects of Velocity Based Vs Traditional Resistance Training Methods On Adaptations in Strength Power and Sprint Speed A SystematicbvgqptkhshNo ratings yet
- Increasing Lean Mass and Strength - HFT vs. LFTDocument9 pagesIncreasing Lean Mass and Strength - HFT vs. LFTKarn Mamgain100% (1)
- Citokinas y Adulto MayorDocument7 pagesCitokinas y Adulto MayorReynaldo TrianaNo ratings yet
- Influence of Resistance Training Frequency On Muscular Adaptations in Well-Trained MenDocument27 pagesInfluence of Resistance Training Frequency On Muscular Adaptations in Well-Trained MenLEANDRO ADOLFO TORRES JARAMILLONo ratings yet
- Strength and Skeletal Muscle Adaptations in Heavy-Resistance-Trained Women After Detraining and RetrainingDocument10 pagesStrength and Skeletal Muscle Adaptations in Heavy-Resistance-Trained Women After Detraining and Retraininglucas AyalaNo ratings yet
- Acute Effect of The "Zero Point" Method On Muscle Thickness and Muscle Damage in Trained MenDocument16 pagesAcute Effect of The "Zero Point" Method On Muscle Thickness and Muscle Damage in Trained MenRodrigo AlvesNo ratings yet
- The Effects of A 7-Week Heavy Elastic Band and Weight Chain Program On Upper-Body Strength and Upper-Body Power in A Sample of Division 1-AA Football PlayersDocument9 pagesThe Effects of A 7-Week Heavy Elastic Band and Weight Chain Program On Upper-Body Strength and Upper-Body Power in A Sample of Division 1-AA Football PlayersKeijoNo ratings yet
- Effects of Single Versus Multiple Bouts of Resistance Training On Maximal Strength and Anaerobic PerformanceDocument10 pagesEffects of Single Versus Multiple Bouts of Resistance Training On Maximal Strength and Anaerobic Performancemarian osorio garciaNo ratings yet
- Strength and Conditioning For Rugby League and Rugby Union Part 1Document10 pagesStrength and Conditioning For Rugby League and Rugby Union Part 1kurupirockeroNo ratings yet
- Researcharticle Open Access: Neil A. Schwarz, Sarah K. Mckinley-Barnard and Zachary J. BlahnikDocument15 pagesResearcharticle Open Access: Neil A. Schwarz, Sarah K. Mckinley-Barnard and Zachary J. BlahnikPoring CarnavasNo ratings yet
- 80/20 Endurance: The Complete System for High-Performance CoachingFrom Everand80/20 Endurance: The Complete System for High-Performance CoachingNo ratings yet
- The Lactate Revolution: The Science Of Quantifying, Predicting, And Improving Human PerformanceFrom EverandThe Lactate Revolution: The Science Of Quantifying, Predicting, And Improving Human PerformanceNo ratings yet
- Starting at The Ground Up Range of Motion.9Document12 pagesStarting at The Ground Up Range of Motion.9Sheilani MartinsNo ratings yet
- Intervalo Combinado de Sprint, Pliométrico e Treinamento de Força em Jogadores de Futebol Adolescentes Efeitos Nas Medidas de Velocidade, Força, Potência, Mudança de Direção e Capacidade AnaeróbiaDocument12 pagesIntervalo Combinado de Sprint, Pliométrico e Treinamento de Força em Jogadores de Futebol Adolescentes Efeitos Nas Medidas de Velocidade, Força, Potência, Mudança de Direção e Capacidade AnaeróbiaSheilani MartinsNo ratings yet
- Infographic Progressing Rehabilitation After InjurDocument2 pagesInfographic Progressing Rehabilitation After InjurSheilani MartinsNo ratings yet
- The Assisted Nordic Hamstring Curl: Exercise TechniqueDocument4 pagesThe Assisted Nordic Hamstring Curl: Exercise TechniqueSheilani MartinsNo ratings yet
- Snach+e+Clean+Weightlifting Movements From Full Extension The.2015 SCJDocument4 pagesSnach+e+Clean+Weightlifting Movements From Full Extension The.2015 SCJSheilani MartinsNo ratings yet
- Studyprotocol Open Access: Alexandra Hott, Sigurd Liavaag, Niels Gunnar Juel and Jens Ivar BroxDocument8 pagesStudyprotocol Open Access: Alexandra Hott, Sigurd Liavaag, Niels Gunnar Juel and Jens Ivar BroxSheilani MartinsNo ratings yet
- Flexibility Training ConceptsDocument20 pagesFlexibility Training ConceptsSheilani MartinsNo ratings yet
- Síndrome de Compressão Torácica 2Document8 pagesSíndrome de Compressão Torácica 2Sheilani MartinsNo ratings yet
- Capacidade de Sprints Repetidos Parte I - Fatores Que Contribuem para A FadigaDocument23 pagesCapacidade de Sprints Repetidos Parte I - Fatores Que Contribuem para A FadigaSheilani MartinsNo ratings yet
- 2014 Pasiakosetal - SportsMed CDocument22 pages2014 Pasiakosetal - SportsMed CSheilani MartinsNo ratings yet
- Síndrome de Compressão TorácicaDocument4 pagesSíndrome de Compressão TorácicaSheilani MartinsNo ratings yet
- Capacidade de Sprints Repetidos - Onde EstamosDocument5 pagesCapacidade de Sprints Repetidos - Onde EstamosSheilani MartinsNo ratings yet
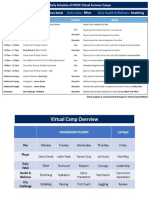
- Sample Daily Schedule Virtual CampDocument2 pagesSample Daily Schedule Virtual CampSheilani MartinsNo ratings yet
- Journal: Periodization: Period or Question Mark?Document4 pagesJournal: Periodization: Period or Question Mark?Sheilani MartinsNo ratings yet
- Variation in Barbell Position Relative To Shoulder and Foot Anatomical Landmarks Alters Movement EfficiencyDocument13 pagesVariation in Barbell Position Relative To Shoulder and Foot Anatomical Landmarks Alters Movement EfficiencySheilani MartinsNo ratings yet
- Now Stay Fit On Vegetarian Diet PDFDocument33 pagesNow Stay Fit On Vegetarian Diet PDFveeru fitness channelNo ratings yet
- Periodization in Anterior Cruciate Ligament Rehabilitation: A Novel FrameworkDocument8 pagesPeriodization in Anterior Cruciate Ligament Rehabilitation: A Novel FrameworkMario Peraza MurilloNo ratings yet
- A Compiled List If Training Myths by Dr. Mike IsraetelDocument32 pagesA Compiled List If Training Myths by Dr. Mike Israetelgasface100% (2)
- Hypertrophy-Specific Training (HST) Workout ProgramDocument11 pagesHypertrophy-Specific Training (HST) Workout ProgramIshita JainNo ratings yet
- A Comparison of Crossfit Training To Traditional Anaerobic ResistDocument85 pagesA Comparison of Crossfit Training To Traditional Anaerobic ResistCeleste Ayala100% (1)
- Stronglifts 5x5 (Blaha M.)Document21 pagesStronglifts 5x5 (Blaha M.)LazniAcc123100% (1)
- M& F ULTRA Month3 ScreenDocument11 pagesM& F ULTRA Month3 Screenjwarswolves0% (1)
- The Timing of Postexercise Protein Ingestion Is-Is Not ImportantDocument5 pagesThe Timing of Postexercise Protein Ingestion Is-Is Not ImportantEdoardo BianchiNo ratings yet
- The Time Course of Short-Term Hypertrophy Without Muscle Damage - Stock Et Al. 2017Document16 pagesThe Time Course of Short-Term Hypertrophy Without Muscle Damage - Stock Et Al. 2017Frangolho JoãoNo ratings yet
- Fiber Type Training: The Most Effective Way To Work The GlutesDocument3 pagesFiber Type Training: The Most Effective Way To Work The Glutesmehrdad_44No ratings yet
- Unit 4 Exercised-Based Fitness PrescriptionDocument38 pagesUnit 4 Exercised-Based Fitness PrescriptionJonathan GalitNo ratings yet
- LUNESDocument7 pagesLUNESjagallegos214No ratings yet
- William Lllewellyn's Anabolics, 11th Edition 2017 61 90Document30 pagesWilliam Lllewellyn's Anabolics, 11th Edition 2017 61 90Hamada MansourNo ratings yet
- Bodybuilding For Beginners - The Practical Guide To Muscle Gain, Fat Burning, and Sculpting A ChiseledDocument129 pagesBodybuilding For Beginners - The Practical Guide To Muscle Gain, Fat Burning, and Sculpting A ChiseledallianztradingNo ratings yet
- Advanced Training Techniques For Muscle Hypertrophy PDFDocument40 pagesAdvanced Training Techniques For Muscle Hypertrophy PDFtpNo ratings yet
- LAT1 Protein Content Increases Following 12 WeeksDocument15 pagesLAT1 Protein Content Increases Following 12 WeeksRosaneLacerdaNo ratings yet
- Does Training Until Failure Maximize Muscle Hypertophy?Document6 pagesDoes Training Until Failure Maximize Muscle Hypertophy?Johnny KeeverNo ratings yet
- Challenge Yourself: Beginner Mens Challenge Preparation GuideDocument23 pagesChallenge Yourself: Beginner Mens Challenge Preparation GuideUni TabberNo ratings yet
- opRvCWadQ6W48ImPKegz Build A Great Chest Mind Pump Media PDFDocument10 pagesopRvCWadQ6W48ImPKegz Build A Great Chest Mind Pump Media PDFWar LinuxNo ratings yet
- Grgic 2017Document12 pagesGrgic 2017ChrisNo ratings yet
- Muscle Intelligence - BP - Arms 7 Day Workouts PDFDocument8 pagesMuscle Intelligence - BP - Arms 7 Day Workouts PDFHarshit Singh100% (2)
- How To Get StrongDocument1 pageHow To Get StrongOle BachmanNo ratings yet
- ALIEN Lean Muscle Mass PDFDocument14 pagesALIEN Lean Muscle Mass PDFHamdan ZafarNo ratings yet