You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5819)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (845)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
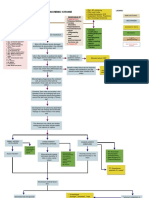
- Acute Ischemic Stroke Concept MapDocument6 pagesAcute Ischemic Stroke Concept MapMoonyeen Jann Casera Balic100% (2)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Renal NursingDocument11 pagesRenal NursingFreeNursingNotes100% (10)
- Ehrlichiosisand Anaplasmosis:: An UpdateDocument42 pagesEhrlichiosisand Anaplasmosis:: An UpdateMargarita CCNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Case Presentation On Pre-EclampsiaDocument18 pagesCase Presentation On Pre-EclampsiaPabhat Kumar89% (9)
- MUST To KNOW in Clinical MicrosDocument26 pagesMUST To KNOW in Clinical MicrosTristan Jay Calabia100% (2)
- Thoracic and Abdominal TraumaDocument76 pagesThoracic and Abdominal Traumajhk0428100% (1)
- Video Laringo Descartable CR-31D PDFDocument2 pagesVideo Laringo Descartable CR-31D PDFgiovanny calderonNo ratings yet
- ReferenceGuide EDocument370 pagesReferenceGuide Egiovanny calderonNo ratings yet
- ReferenceGuide EDocument366 pagesReferenceGuide Egiovanny calderonNo ratings yet
- Eigen Pamphlet 2016Document12 pagesEigen Pamphlet 2016giovanny calderonNo ratings yet
- CSH Perspectives Rev - Apolipoprotein E and Apolipoprotein E Receptors - Normal Biology and Roles in ADDocument23 pagesCSH Perspectives Rev - Apolipoprotein E and Apolipoprotein E Receptors - Normal Biology and Roles in ADGeneziz DiazNo ratings yet
- YNM Part 2 - ExplainDocument61 pagesYNM Part 2 - ExplainCHAKRADHARA RAO100% (1)
- Criteri 205 JohnesDocument7 pagesCriteri 205 JohnesTeodor ŞişianuNo ratings yet
- Clinical Neurology Made EasyDocument189 pagesClinical Neurology Made Easyranin ditaNo ratings yet
- Hemoptysis 1Document27 pagesHemoptysis 1Ruby FirdausNo ratings yet
- Analgesic Nephropathy: Is It Caused by Multi-Analgesic Abuse or Single Substance Use?Document10 pagesAnalgesic Nephropathy: Is It Caused by Multi-Analgesic Abuse or Single Substance Use?Michelle VerhoevenNo ratings yet
- Jurnal Pakai 5 (Patofisiologi, Gejala)Document7 pagesJurnal Pakai 5 (Patofisiologi, Gejala)Satrya DitaNo ratings yet
- Prepared By: Melody Gay M. Igcasenza, PTRP, RNDocument122 pagesPrepared By: Melody Gay M. Igcasenza, PTRP, RNtishpatNo ratings yet
- SLE Notes PDFDocument4 pagesSLE Notes PDFSrinivas PingaliNo ratings yet
- Choledocholithiasis - Clinical Manifestations, Diagnosis, and Management - UpToDateDocument19 pagesCholedocholithiasis - Clinical Manifestations, Diagnosis, and Management - UpToDateFeer VillarrealNo ratings yet
- Final Coaching NP3 Set3Document14 pagesFinal Coaching NP3 Set3STEFFI GABRIELLE GOLEZNo ratings yet
- Katie Is A Teenage Girl Who Suffers From A Rare Disease Called Xeroderma Pigmentosum. HerDocument4 pagesKatie Is A Teenage Girl Who Suffers From A Rare Disease Called Xeroderma Pigmentosum. HerLyrah ManioNo ratings yet
- Acute Appendicitis 2Document7 pagesAcute Appendicitis 2Aiman ArifinNo ratings yet
- Drug Study - IbuprofenDocument7 pagesDrug Study - IbuprofenajNo ratings yet
- Case Study - ESRD (DS, NCP)Document8 pagesCase Study - ESRD (DS, NCP)Zhy CaluzaNo ratings yet
- Anorexia Myanmar 2019Document33 pagesAnorexia Myanmar 2019Naing LlynNo ratings yet
- Siadh Diabetes Insipidus Acute Renal Failure Chronic Renal FailureDocument6 pagesSiadh Diabetes Insipidus Acute Renal Failure Chronic Renal FailureRanusha AnushaNo ratings yet
- Tarporley October 19Document100 pagesTarporley October 19Talkabout PublishingNo ratings yet
- NCMB 312 MS RLE WEEK 15 Concept Mapping GI BleedingDocument2 pagesNCMB 312 MS RLE WEEK 15 Concept Mapping GI BleedinggabbyNo ratings yet
- Neurosurgery Past PapersDocument74 pagesNeurosurgery Past PapersRand Ahmad100% (1)
- BlepharitisDocument20 pagesBlepharitisNorshahidah IedaNo ratings yet
- Blood Products and Their Indications: Mr. Donald BrownDocument33 pagesBlood Products and Their Indications: Mr. Donald BrownJasleen KaurNo ratings yet
- ANAPHY - Nervous SystemDocument5 pagesANAPHY - Nervous SystemMA. ANDREA NICOLE DURANNo ratings yet