You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5814)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (845)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Notice of Appeal NAPOLCOMDocument3 pagesNotice of Appeal NAPOLCOMJhoey Castillo Bueno75% (4)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Crane LoadingsDocument2 pagesCrane Loadingsmoseslugtu632470% (10)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Role of Beliefs in Teacher Agency: A Critical AnalysisDocument9 pagesThe Role of Beliefs in Teacher Agency: A Critical AnalysisSapna Shyam JeetahNo ratings yet
- Contoh Soal SelidikDocument3 pagesContoh Soal SelidikRohaiza RozaliNo ratings yet
- Lesson Plan in Biology Second Year High SchoolDocument3 pagesLesson Plan in Biology Second Year High SchoolJayCesarNo ratings yet
- Karen Horney Quiz Theories of PersonalityDocument2 pagesKaren Horney Quiz Theories of Personalityzainab hanifNo ratings yet
- Official History of Improved Order of RedmenDocument672 pagesOfficial History of Improved Order of RedmenGiniti Harcum El BeyNo ratings yet
- The Perception of Color in Architecture - by TMD STUDIO LTD - TMD STUDIO's Insights - MediumDocument2 pagesThe Perception of Color in Architecture - by TMD STUDIO LTD - TMD STUDIO's Insights - MediumStella ChalNo ratings yet
- Symmetricom Syncserver - S300 - S350Document214 pagesSymmetricom Syncserver - S300 - S350Fürst AdemarNo ratings yet
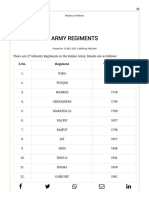
- Army Regiments: S.No. Regiment Year of RaisingDocument3 pagesArmy Regiments: S.No. Regiment Year of RaisingAsc47No ratings yet
- ComDocument294 pagesComAMAN SAXENANo ratings yet
- Transliteration-Telugu: Mokshamu Galada-SaramatiDocument8 pagesTransliteration-Telugu: Mokshamu Galada-Saramativishwa007No ratings yet
- CMucat Application FormDocument1 pageCMucat Application FormJiyan Litohon100% (1)
- Space Curves - 1: Differential Geometry III, Solutions 4 (Week 4)Document3 pagesSpace Curves - 1: Differential Geometry III, Solutions 4 (Week 4)Gag PafNo ratings yet
- Diagnostic Imagining Technique. (Osce)Document17 pagesDiagnostic Imagining Technique. (Osce)Rabah IrfanNo ratings yet
- Sonnet 54Document7 pagesSonnet 54api-272948113No ratings yet
- International Marketing ModuleDocument131 pagesInternational Marketing ModuleTekle KochitoNo ratings yet
- Culture and Multinational ManagementDocument82 pagesCulture and Multinational ManagementDr.Revathi AnandkumarNo ratings yet
- Teaching NotesDocument13 pagesTeaching NotesmaxventoNo ratings yet
- John McDowell, Wittgenstein On Following A Rule', Synthese 58, 325-63, 1984.Document40 pagesJohn McDowell, Wittgenstein On Following A Rule', Synthese 58, 325-63, 1984.happisseiNo ratings yet
- SEBI Order Satyam PDFDocument65 pagesSEBI Order Satyam PDFABHIJEETNo ratings yet
- Unruh 2Document7 pagesUnruh 2amanNo ratings yet
- Bagua Zhuan Huan ZhangDocument6 pagesBagua Zhuan Huan Zhangjilongfeng666No ratings yet
- Ihcdc 2021Document2 pagesIhcdc 2021Wisnu WiwekaNo ratings yet
- Jan Scholten Repertory of The Elements 5994eceb1723ddd169543dffDocument3 pagesJan Scholten Repertory of The Elements 5994eceb1723ddd169543dffUsman AnsariNo ratings yet
- Conditionals If Clauses Testi 1 50 Soruluk Cevap Anahtari 91684Document5 pagesConditionals If Clauses Testi 1 50 Soruluk Cevap Anahtari 91684zakariaalkassem3No ratings yet
- Mythic Odysseys of Theros (+deluxe Cover) - 2Document26 pagesMythic Odysseys of Theros (+deluxe Cover) - 2gabiNo ratings yet
- Writing - Exercise 6 (Writing A Report) - IGCSE AIDDocument3 pagesWriting - Exercise 6 (Writing A Report) - IGCSE AIDDonet M. ThomasNo ratings yet
- ROC Graphs: Notes and Practical Considerations For Data Mining ResearchersDocument28 pagesROC Graphs: Notes and Practical Considerations For Data Mining ResearchersJan ShumwayNo ratings yet
- Intro Mass SpecDocument2 pagesIntro Mass SpecHuy Đặng Anh0% (1)