You might also like
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Dıffıcultıes in Teachıng Essay Wrıtıng in Englısh: Jabbarov Ulugbek, Jabbarova AnoraDocument9 pagesDıffıcultıes in Teachıng Essay Wrıtıng in Englısh: Jabbarov Ulugbek, Jabbarova Anoraroger inocencioNo ratings yet
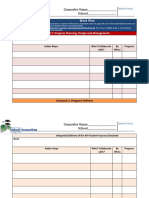
- Work Plan Template 10Document9 pagesWork Plan Template 10Mariem BejiNo ratings yet
- Meiosis Ppt.2014Document47 pagesMeiosis Ppt.2014Alyssa BowmanNo ratings yet
- DRRM Accomplishment ReportDocument4 pagesDRRM Accomplishment Reportroger inocencio100% (2)
- Mendelian GeneticsDocument20 pagesMendelian Geneticsroger inocencioNo ratings yet
- Improving Attitudes Toward Mathematics Learning With Problem Posing in Class VIIIDocument9 pagesImproving Attitudes Toward Mathematics Learning With Problem Posing in Class VIIIroger inocencioNo ratings yet
- RUBRIC - Essay EvaluationDocument2 pagesRUBRIC - Essay Evaluationroger inocencioNo ratings yet
- For School DRRM Coordinators (TREE PLANTING ACTIVITY) - To Be Submitted ToDocument6 pagesFor School DRRM Coordinators (TREE PLANTING ACTIVITY) - To Be Submitted ToReynaldo Wayacan Garro Jr.No ratings yet
- Teacher Induction Program Module 1 V1Document133 pagesTeacher Induction Program Module 1 V1Katniss Remar DeeNo ratings yet
- Home Visitation FormDocument1 pageHome Visitation Formroger inocencioNo ratings yet
- Home Visitation FormDocument1 pageHome Visitation Formroger inocencioNo ratings yet
- Home Visitation FormDocument1 pageHome Visitation Formroger inocencioNo ratings yet
- Automated SF2Document115 pagesAutomated SF2roger inocencioNo ratings yet
- DepEd 2020 Standard Screen PDFDocument1 pageDepEd 2020 Standard Screen PDFroger inocencioNo ratings yet
- Indigenized Instructional MaterialsDocument4 pagesIndigenized Instructional MaterialsJoymar Hapson0% (1)
- 3 Module 9 WalkthroughDocument15 pages3 Module 9 WalkthroughIan Khay CastroNo ratings yet
- DLL Template g8 2nd QuarterdoneDocument55 pagesDLL Template g8 2nd QuarterdoneChai Barcelon97% (116)
- DLL Template g8 2nd QuarterdoneDocument55 pagesDLL Template g8 2nd QuarterdoneChai Barcelon97% (116)
- DM SGOD No. 82 Division Search For The Best Gulayan Sa Paaralan Program GPP School Garden Implementers For School Year 2018 2019Document7 pagesDM SGOD No. 82 Division Search For The Best Gulayan Sa Paaralan Program GPP School Garden Implementers For School Year 2018 2019roger inocencioNo ratings yet
- Periodical Test in Science 8Document3 pagesPeriodical Test in Science 8Eileen Joy Noceda88% (194)
- Module11.PPST5 .2.2 PDFDocument36 pagesModule11.PPST5 .2.2 PDFGinny Paul Gabuan100% (1)
- Table of SpecuficationsDocument3 pagesTable of SpecuficationsBernardo MacaranasNo ratings yet
- UM-NO 620s 2016Document2 pagesUM-NO 620s 2016roger inocencioNo ratings yet
- Word Problem Solving in Middle Grades MathematicsDocument16 pagesWord Problem Solving in Middle Grades Mathematicsroger inocencioNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Berklee Ear Training ConductingDocument17 pagesBerklee Ear Training Conductingpavan sagarNo ratings yet
- Setting Up and Using Field Service Advanced SchedulerDocument43 pagesSetting Up and Using Field Service Advanced Schedulermohammed achatNo ratings yet
- SQL SH Solutions Exercices 2Document1 pageSQL SH Solutions Exercices 2Charafeddine ELBAHJANo ratings yet
- Microwave Link Design, Survey and Installation in Pyay Technological UniversityDocument5 pagesMicrowave Link Design, Survey and Installation in Pyay Technological UniversitySaid AdamNo ratings yet
- How To Beat Facial Recognition TechnologyDocument8 pagesHow To Beat Facial Recognition Technologyjack007xrayNo ratings yet
- Modul Pemrograman Database IDocument62 pagesModul Pemrograman Database IMuhammad Arya Rahmat BarokhahNo ratings yet
- Ongc DataDocument407 pagesOngc DataFunding MillilonsNo ratings yet
- HowTo Calibration ES-1000 v1Document8 pagesHowTo Calibration ES-1000 v1trunghieu02ck1No ratings yet
- Text2App - A Framework For Creating Android Apps From Text DescriptionsDocument9 pagesText2App - A Framework For Creating Android Apps From Text Descriptionssarte00No ratings yet
- Timecreator 1000Document298 pagesTimecreator 1000Jacob WilkersonNo ratings yet
- Application of Hybrid Ensemble Machine Learning Approach For Prediction of Residential Natural Gas Demand and ConsumptionDocument8 pagesApplication of Hybrid Ensemble Machine Learning Approach For Prediction of Residential Natural Gas Demand and ConsumptionInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- GenMath Week 1 - 051343Document61 pagesGenMath Week 1 - 051343Reymark VelascoNo ratings yet
- Entry Level Software Developer Resume ExamplesDocument5 pagesEntry Level Software Developer Resume Examplesafjwdbaekycbaa100% (2)
- Pageview As Id 33348Document109 pagesPageview As Id 33348long chenNo ratings yet
- Operating System Services: Col. Genetu Yohannes (Lecturer) Department of CIT, College of Engineering Defence UniversityDocument31 pagesOperating System Services: Col. Genetu Yohannes (Lecturer) Department of CIT, College of Engineering Defence UniversityAmanuelNo ratings yet
- Features of PythonDocument77 pagesFeatures of PythonA.Dinesh arumugamNo ratings yet
- Probability and Statistics For Engineering and The Sciences International Metric Edition 9th Edition Devore Solutions ManualDocument38 pagesProbability and Statistics For Engineering and The Sciences International Metric Edition 9th Edition Devore Solutions Manualegglertitularxidp100% (13)
- FDD, HDD, USB, Card: Emulator FDD 1,44MB - USB - BlackDocument5 pagesFDD, HDD, USB, Card: Emulator FDD 1,44MB - USB - BlackEhsan PoravarNo ratings yet
- Data Science: What Is Data Science and Who Is Data ScientistDocument26 pagesData Science: What Is Data Science and Who Is Data ScientistZaib KhanNo ratings yet
- How To Check Possible Causes If MRP Does Not Create Any ProposalsDocument7 pagesHow To Check Possible Causes If MRP Does Not Create Any Proposalssangeeta_pradhan_3No ratings yet
- Fortigate 200F Series: Data SheetDocument6 pagesFortigate 200F Series: Data SheetEliranNo ratings yet
- Installation Checklist For SPV Module: Sterling and Wilson Document No.: SW-SEPC-ICL-PV-002, Rev: 01Document2 pagesInstallation Checklist For SPV Module: Sterling and Wilson Document No.: SW-SEPC-ICL-PV-002, Rev: 01Adithi RNo ratings yet
- What Is Functional Dependency?: Re Exivity: If Y Is A Subset of X, Then X Y Holds by Re Exivity RuleDocument17 pagesWhat Is Functional Dependency?: Re Exivity: If Y Is A Subset of X, Then X Y Holds by Re Exivity RuleDivya SinghNo ratings yet
- Information Technology Practice TestDocument2 pagesInformation Technology Practice TestKenneth Bailey100% (1)
- Mikrotik in Real Life, Full Scale and Low Budget ISP PDFDocument44 pagesMikrotik in Real Life, Full Scale and Low Budget ISP PDFNay Lin KyawNo ratings yet
- Lecture 1 - Introduction: Data Warehouses, Business Intelligence, Data MiningDocument41 pagesLecture 1 - Introduction: Data Warehouses, Business Intelligence, Data MiningxainshahNo ratings yet
- TDA Cyber Snapshot 2022Document20 pagesTDA Cyber Snapshot 2022CerealCruncherNo ratings yet
- HSC Biology 1st Part (Abul Hossain)Document359 pagesHSC Biology 1st Part (Abul Hossain)Arafat Turjoy50% (2)
- Controller Option (M416) PC 120912Document8 pagesController Option (M416) PC 120912Dawood AhmedNo ratings yet
- MPI DynamicprocessesDocument47 pagesMPI DynamicprocessesBassel GhaybourNo ratings yet