You might also like
- Sample SoapDocument9 pagesSample SoapDouglas Greg Cook90% (20)
- PEDIA Case 4.1. Dengue FeverDocument10 pagesPEDIA Case 4.1. Dengue Feverotartil_nimanNo ratings yet
- Case Presentation - Acute GlomerulonephritisDocument10 pagesCase Presentation - Acute GlomerulonephritisRold Brio SosNo ratings yet
- Pedia 1Document8 pagesPedia 1Jani MisterioNo ratings yet
- D20 Modern - Evil Dead PDFDocument39 pagesD20 Modern - Evil Dead PDFLester Cooper100% (1)
- Entrepreneurship Assignment 1 Business Concept ReportDocument2 pagesEntrepreneurship Assignment 1 Business Concept ReportNoor Nabi ShaikhNo ratings yet
- Protein Expression HandbookDocument118 pagesProtein Expression HandbookLuis Arístides Torres SánchezNo ratings yet
- Monetizing Judgments DatasheetDocument9 pagesMonetizing Judgments DatasheetJohnWilliams100% (4)
- The Next Form of DemocracyDocument313 pagesThe Next Form of DemocracyVanderbilt University Press100% (2)
- IM Gastro FinalDocument10 pagesIM Gastro FinalIzzyMaxinoNo ratings yet
- Discharge Summary JAGONOYDocument6 pagesDischarge Summary JAGONOYKirstie de LunaNo ratings yet
- Diabetes Mellitus Complte LONG 2Document56 pagesDiabetes Mellitus Complte LONG 2John Vincent Dy OcampoNo ratings yet
- Clinical Case Presentation on Peptic Ulcer DiseaseDocument44 pagesClinical Case Presentation on Peptic Ulcer DiseaseRUSSELL CILOTNo ratings yet
- Woman with UTI and DiabetesDocument11 pagesWoman with UTI and DiabetesShakshi RainaNo ratings yet
- Week 3 Case - DOBDocument3 pagesWeek 3 Case - DOBKirk Matthew ZhuNo ratings yet
- BGL 1 ClerksDocument3 pagesBGL 1 ClerksJohnJoelArzagaNo ratings yet
- Acute Appendicitis Case StudyDocument16 pagesAcute Appendicitis Case StudyAslah NabilahNo ratings yet
- IM - Patient Esguera (Final)Document4 pagesIM - Patient Esguera (Final)k.n.e.d.No ratings yet
- medical report - PneumoniaeDocument8 pagesmedical report - Pneumoniaenguyenhoavanchi2002No ratings yet
- Empyema ThoracisDocument14 pagesEmpyema ThoracisMara AbantoNo ratings yet
- Decreased Fetal Movement CaseDocument3 pagesDecreased Fetal Movement CaseNehemiah FranciscoNo ratings yet
- Case Protocol - GBS - TanguilanDocument7 pagesCase Protocol - GBS - TanguilanRosealie TanguilanNo ratings yet
- Ob Gyn Sample HisotryDocument4 pagesOb Gyn Sample HisotrySophia RubiaNo ratings yet
- Group 2: Vaibhav Jain Kaliyannan Kayalvizhi Krishnamoorthy Srinath Kumar EswariDocument35 pagesGroup 2: Vaibhav Jain Kaliyannan Kayalvizhi Krishnamoorthy Srinath Kumar EswariZedd ZorïNo ratings yet
- HISTORY # 1 - PCGH, EchavezDocument11 pagesHISTORY # 1 - PCGH, EchavezHynne Jhea EchavezNo ratings yet
- Caseeeee Egaaa IrbasssDocument27 pagesCaseeeee Egaaa IrbasssIrbasMantiniSyaifulNo ratings yet
- Liver Cirrhosis Patient with HematemesisDocument12 pagesLiver Cirrhosis Patient with HematemesisMarianne R. LorenzoNo ratings yet
- Essential Hypertension Case PresentationDocument9 pagesEssential Hypertension Case PresentationCalingalan Hussin CaluangNo ratings yet
- Clinicopathologic Case Conference: Department of Family MedicineDocument39 pagesClinicopathologic Case Conference: Department of Family MedicineRaq KhoNo ratings yet
- Case Write Up MedicineDocument16 pagesCase Write Up MedicineKamogelo MabotjaNo ratings yet
- Internal Medicine (II) 2011 LogbookDocument73 pagesInternal Medicine (II) 2011 LogbookQasim HaleimiNo ratings yet
- CPC CaseDocument8 pagesCPC CasePingky khingthongNo ratings yet
- History and PE Med3ADocument3 pagesHistory and PE Med3Aawesome avedNo ratings yet
- Soap 2Document5 pagesSoap 2api-456313554No ratings yet
- 6904 Module 1 HistoryDocument3 pages6904 Module 1 Historyapi-618492022No ratings yet
- Surg Week 4Document75 pagesSurg Week 4Casey YanoNo ratings yet
- Case PresentationDocument36 pagesCase PresentationPrincewill SmithNo ratings yet
- Rectal CancerDocument71 pagesRectal CancerGio Balisi100% (2)
- Enterobiasis CaseDocument4 pagesEnterobiasis CaseKimm Delos ReyesNo ratings yet
- Cerebral Venous Thrombosis (CVT)Document9 pagesCerebral Venous Thrombosis (CVT)babuNo ratings yet
- HydrocephalusDocument19 pagesHydrocephalusJessielyn SiaNo ratings yet
- Nursing Care Plans for Neurological and Cardiovascular CasesDocument15 pagesNursing Care Plans for Neurological and Cardiovascular CasesJane FlorendoNo ratings yet
- History: O Identifying DataDocument10 pagesHistory: O Identifying DataJofen Ann Hisoler TangpuzNo ratings yet
- Case Presentation Acute GlomerulonephritisDocument10 pagesCase Presentation Acute Glomerulonephritisminangsung minangnengNo ratings yet
- Acute Nephrotic SyndromeDocument10 pagesAcute Nephrotic SyndromeEvi SilviaNo ratings yet
- OPD Case Protocol UTIDocument75 pagesOPD Case Protocol UTIJulienne Sanchez-SalazarNo ratings yet
- 'Batangas Medical Center Case Report by PGI Carlos H. AcuñaDocument7 pages'Batangas Medical Center Case Report by PGI Carlos H. AcuñaCarlos H. AcuñaNo ratings yet
- Case Clerking ApendicDocument15 pagesCase Clerking ApendicMelvin Khung100% (1)
- Acute Appendicitis 3Document8 pagesAcute Appendicitis 3Aiman ArifinNo ratings yet
- Admission Conference: Ernesto V. Ignacio JRDocument17 pagesAdmission Conference: Ernesto V. Ignacio JRernignacioNo ratings yet
- Case Presentation: Course: EndocrinologyDocument13 pagesCase Presentation: Course: EndocrinologyCalingalan Hussin CaluangNo ratings yet
- Block 7 Active Phase 1st Stage of LaborDocument29 pagesBlock 7 Active Phase 1st Stage of LaborRoselle Joy D. RosalejosNo ratings yet
- B19 Pleno Sken2Document15 pagesB19 Pleno Sken2Adelia YuantikaNo ratings yet
- Easter College: Department of NursingDocument13 pagesEaster College: Department of NursingShaii shanNo ratings yet
- B6 - Surgery GS II Case IIDocument10 pagesB6 - Surgery GS II Case IIGregNo ratings yet
- Nephrotic Syndrome in an 8-Year-Old BoyDocument54 pagesNephrotic Syndrome in an 8-Year-Old BoySulaiman TahsinNo ratings yet
- Chest Pain Case PresentationDocument70 pagesChest Pain Case PresentationAj Christian Lacuesta IsipNo ratings yet
- Team C Final Written OutputDocument22 pagesTeam C Final Written OutputCarina SuarezNo ratings yet
- Dysuria and ComorbiditiesDocument39 pagesDysuria and ComorbiditiesChathiya Banu KrishenanNo ratings yet
- CPC-Patho Version 6Document20 pagesCPC-Patho Version 6Bea SamonteNo ratings yet
- ASD Internship ReportingDocument14 pagesASD Internship ReportingPernel Jose Alam MicuboNo ratings yet
- Islamic University in Uganda: Habib Medical SchoolDocument8 pagesIslamic University in Uganda: Habib Medical SchoolUsaid SulaimanNo ratings yet
- Chronic Diseases - Lymes, Hpv, Hsv Mis-Diagnosis and Mistreatment: A New Approach to the EpidemicFrom EverandChronic Diseases - Lymes, Hpv, Hsv Mis-Diagnosis and Mistreatment: A New Approach to the EpidemicRating: 5 out of 5 stars5/5 (1)
- MRI Safety Update for Patients with CIEDsDocument26 pagesMRI Safety Update for Patients with CIEDsNehemiah FranciscoNo ratings yet
- PID Notes 2Document3 pagesPID Notes 2Nehemiah FranciscoNo ratings yet
- EBCPGonthyroidDocument35 pagesEBCPGonthyroidAwee WeeNo ratings yet
- COVID-19 Diagnosis and Management: A Brief GuideDocument60 pagesCOVID-19 Diagnosis and Management: A Brief GuideNehemiah FranciscoNo ratings yet
- Nasal Congestion Relief with ProbioticDocument4 pagesNasal Congestion Relief with ProbioticNehemiah FranciscoNo ratings yet
- IVF Dosage Guide for Common Pediatric MedicationsDocument5 pagesIVF Dosage Guide for Common Pediatric MedicationsEloiseBalasbasNo ratings yet
- Approach To The Child With AnemiaDocument20 pagesApproach To The Child With AnemiaNehemiah FranciscoNo ratings yet
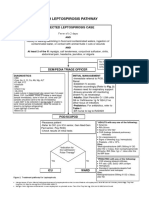
- Leptospirosis Pathway JULY 2018FINALDocument5 pagesLeptospirosis Pathway JULY 2018FINALNehemiah FranciscoNo ratings yet
- Pediatric Clinical History TemplateDocument6 pagesPediatric Clinical History TemplateNehemiah Francisco100% (2)
- 17-Ebcpg Thyroid2013Document20 pages17-Ebcpg Thyroid2013Mi MingkaiNo ratings yet
- DM2020-0319 Interim Guidelines On COVID-19 Management of Pregnant Women, Women About To Give Birth, and NewbornsDocument12 pagesDM2020-0319 Interim Guidelines On COVID-19 Management of Pregnant Women, Women About To Give Birth, and NewbornsNehemiah FranciscoNo ratings yet
- OPD Adolescent History FormDocument5 pagesOPD Adolescent History FormNehemiah FranciscoNo ratings yet
- Leptospirosis CPG 2010 PDFDocument66 pagesLeptospirosis CPG 2010 PDFRogelio Junior RiveraNo ratings yet
- Masas Cervicales AAOHNSDocument30 pagesMasas Cervicales AAOHNSchwbaccaNo ratings yet
- Physical ExaminationDocument2 pagesPhysical ExaminationNehemiah FranciscoNo ratings yet
- Clincal Practice Guidelines For Diabetes in The PhilippinesDocument40 pagesClincal Practice Guidelines For Diabetes in The PhilippinesRans NosceNo ratings yet
- Essential Newborn Care StepsDocument40 pagesEssential Newborn Care StepsNehemiah FranciscoNo ratings yet
- Decreased Fetal Movement CaseDocument3 pagesDecreased Fetal Movement CaseNehemiah FranciscoNo ratings yet
- Physical ExaminationDocument2 pagesPhysical ExaminationNehemiah FranciscoNo ratings yet
- PD - E7 - TOPIC2 - History Taking and PE of Pediatric PatientDocument11 pagesPD - E7 - TOPIC2 - History Taking and PE of Pediatric PatientNehemiah FranciscoNo ratings yet
- De La Salle University Medical Center Department of Obstetrics and Gynecology Cases Admissions February 2021Document3 pagesDe La Salle University Medical Center Department of Obstetrics and Gynecology Cases Admissions February 2021Nehemiah FranciscoNo ratings yet
- Gastric CaseDocument19 pagesGastric CaseNehemiah FranciscoNo ratings yet
- OPD Adolescent History FormDocument5 pagesOPD Adolescent History FormNehemiah FranciscoNo ratings yet
- De La Salle Medical College Suturing GuideDocument6 pagesDe La Salle Medical College Suturing GuideNehemiah FranciscoNo ratings yet
- Pediatric Clinical History TemplateDocument6 pagesPediatric Clinical History TemplateNehemiah Francisco100% (2)
- Basic Wound Dressing On A Surgical WoundDocument2 pagesBasic Wound Dressing On A Surgical WoundNehemiah FranciscoNo ratings yet
- Medical Circumcision: Biblical HistoryDocument2 pagesMedical Circumcision: Biblical HistoryNehemiah FranciscoNo ratings yet
- Basic Wound Dressing LectureDocument9 pagesBasic Wound Dressing LectureNehemiah FranciscoNo ratings yet
- RBC Production and DestructionDocument44 pagesRBC Production and DestructionNehemiah FranciscoNo ratings yet
- Importance of Research in ArchitectureDocument9 pagesImportance of Research in ArchitectureKathleen Mae SoriaNo ratings yet
- Quiz ManaSciDocument15 pagesQuiz ManaSciRocio Isabel LuzuriagaNo ratings yet
- ĐỀ THI GIỮA KÌ 2 - E9 (TẤN)Document4 pagesĐỀ THI GIỮA KÌ 2 - E9 (TẤN)xyencoconutNo ratings yet
- P17P01 Ca019 17 An 101 1260 in DWG 191 - Tus Ins 233 FS 0194 - 0 PDFDocument7 pagesP17P01 Ca019 17 An 101 1260 in DWG 191 - Tus Ins 233 FS 0194 - 0 PDFrenzomcuevaNo ratings yet
- OBE-Syllabus Photography 2015Document8 pagesOBE-Syllabus Photography 2015Frederick Eboña100% (1)
- OS Fundamentals: Memory, Processes, KernelsDocument36 pagesOS Fundamentals: Memory, Processes, KernelsSparkerz S Vijay100% (1)
- HCPN Certification Agreement, Partner Agreement-HUAWEI CLOUDDocument9 pagesHCPN Certification Agreement, Partner Agreement-HUAWEI CLOUDSolNo ratings yet
- State of Employee Engagement: Global Survey 2010Document16 pagesState of Employee Engagement: Global Survey 2010aptmbaNo ratings yet
- 10 INSIGHT - 2023 - D SouzaDocument7 pages10 INSIGHT - 2023 - D SouzazhaobingNo ratings yet
- The Role of Standards in Smart CitiesDocument19 pagesThe Role of Standards in Smart CitiesmeyyaNo ratings yet
- Data Compilation TemplateDocument257 pagesData Compilation TemplateemelyseuwaseNo ratings yet
- Anuraj JainDocument3 pagesAnuraj Jainanuraj1983No ratings yet
- Hematology: AnemiaDocument46 pagesHematology: AnemiaCyrus100% (1)
- OCCUPATIONAL SAFETY REGULATIONSDocument126 pagesOCCUPATIONAL SAFETY REGULATIONSKarthikeyan Sankarrajan100% (3)
- ISE215 Lecture4 Usingtheproduct Andre SjsuDocument25 pagesISE215 Lecture4 Usingtheproduct Andre SjsuHALASA TextilHogarNo ratings yet
- SAnet CD 9811017409 PDFDocument357 pagesSAnet CD 9811017409 PDFoeamaoesahaNo ratings yet
- IAII FINAL EXAM Maual SET BDocument9 pagesIAII FINAL EXAM Maual SET BClara MacallingNo ratings yet
- Election Summary Report November 3, 2020 - General Election Wayne County, Michigan Unofficial ResultsDocument77 pagesElection Summary Report November 3, 2020 - General Election Wayne County, Michigan Unofficial ResultsStephen BoyleNo ratings yet
- 07 Trumpet 2, 3Document3 pages07 Trumpet 2, 3Eneas Augusto100% (1)
- Maintenance and Service GuideDocument185 pagesMaintenance and Service GuidenstomarNo ratings yet
- Liming Heavy Industry Introduction NewDocument7 pagesLiming Heavy Industry Introduction NewJohnny DoeNo ratings yet
- Activityideabank FinalDocument72 pagesActivityideabank FinalJoy Tu TranNo ratings yet
- Communicating EffectivelyDocument7 pagesCommunicating EffectivelyPaulo LewisNo ratings yet
- Elon Musk AchievementsDocument13 pagesElon Musk AchievementsCarlos SuárezNo ratings yet
- Hill Et Al 2013 Evol Hum BehavDocument8 pagesHill Et Al 2013 Evol Hum BehavMike WillieNo ratings yet