You might also like
- SE Chapter 5Document4 pagesSE Chapter 5Mohamed Abdirahman AddowNo ratings yet
- Service Science, Management, and Engineering:: Theory and ApplicationsFrom EverandService Science, Management, and Engineering:: Theory and ApplicationsNo ratings yet
- System Integration and Architecture 1Document8 pagesSystem Integration and Architecture 1charimaine hernandezNo ratings yet
- The Modelingof Clinic Systems Using Unified Modeling Language UML3Document15 pagesThe Modelingof Clinic Systems Using Unified Modeling Language UML3Muhammad Qasim RazaNo ratings yet
- 1 OnlineDocument6 pages1 Onlinefedonay746No ratings yet
- Chapter 5 System Modeling 1 30/10/2014Document58 pagesChapter 5 System Modeling 1 30/10/2014daniel whitelyNo ratings yet
- Diagrams, and Object Diagrams, Which Are Used To Create The Structural ModelDocument14 pagesDiagrams, and Object Diagrams, Which Are Used To Create The Structural ModelLonAtanacioNo ratings yet
- A UML Approach To Process Modelling of Clinical Practice Guidelines For EnactmentDocument6 pagesA UML Approach To Process Modelling of Clinical Practice Guidelines For Enactmentpecs1021No ratings yet
- Chapter 5 System Modeling 1Document60 pagesChapter 5 System Modeling 1Ryle Gabriel MagistradoNo ratings yet
- Ch5 System ModelingDocument112 pagesCh5 System ModelingmisbahNo ratings yet
- System Modeling: Existing and Planned System ModelsDocument5 pagesSystem Modeling: Existing and Planned System ModelsMaricar SucalditoNo ratings yet
- Assignment - 01: Department of Computer Science & EngineeringDocument8 pagesAssignment - 01: Department of Computer Science & Engineeringfourth year projectNo ratings yet
- L07-System ModelingDocument48 pagesL07-System Modelingnagui.mostafaNo ratings yet
- Firstly... What Is UML?: Software DevelopmentDocument12 pagesFirstly... What Is UML?: Software Developmentekichi_onizukaNo ratings yet
- CS 410/510 - Software Engineering System Modeling: The Big PictureDocument6 pagesCS 410/510 - Software Engineering System Modeling: The Big PictureNaveed HarshaNo ratings yet
- Software Ngineering ModelingDocument54 pagesSoftware Ngineering ModelingblinNo ratings yet
- Se Model 4Document8 pagesSe Model 4Praveen KumarNo ratings yet
- Lec 8 SEDocument23 pagesLec 8 SENaima Naeem 631-FBAS/BSIT/F21No ratings yet
- 1 Chapter 5 System ModelingDocument53 pages1 Chapter 5 System Modelingtrà giang võ thịNo ratings yet
- Abstract Hospital Future V1.6Document2 pagesAbstract Hospital Future V1.6Dima AmmoraNo ratings yet
- System Modelling 5Document46 pagesSystem Modelling 5Etefa BelachewNo ratings yet
- Classification of Model and Simulation: TopicDocument15 pagesClassification of Model and Simulation: TopicOrion SowNo ratings yet
- System ModellingDocument18 pagesSystem ModellingKHALiFA OpNo ratings yet
- UML Pros Cons IWSSD 10Document12 pagesUML Pros Cons IWSSD 10utpal_rohitNo ratings yet
- Analysis and Design of Clinical Information Management System Based On UML of AIDS of Traditional Chinese MedicineDocument5 pagesAnalysis and Design of Clinical Information Management System Based On UML of AIDS of Traditional Chinese MedicineMohamad Nizwan MarjugiNo ratings yet
- SE Module 3Document23 pagesSE Module 3The BigBradNo ratings yet
- What Is UMLDocument5 pagesWhat Is UMLPankaj AgarwalNo ratings yet
- Unified Modeling Language and Design of Case-Based Retrieval Medical ImagingDocument5 pagesUnified Modeling Language and Design of Case-Based Retrieval Medical ImagingAshwini PatilNo ratings yet
- P PP PDocument9 pagesP PP PNikita SoniNo ratings yet
- Advance System Analysis: Agile Model-Driven Development (AMDD), Usage ModelingDocument23 pagesAdvance System Analysis: Agile Model-Driven Development (AMDD), Usage Modelingapi-19822376No ratings yet
- Chapter 5 System Modeling 1Document20 pagesChapter 5 System Modeling 1Etengal SebelasNo ratings yet
- Lecture 5 - System ModellingDocument53 pagesLecture 5 - System Modellingabdiburgal5No ratings yet
- System ModelingDocument7 pagesSystem ModelingHassan .YNo ratings yet
- Use Case Modelling by Kurt Bittner and Ian SpenceDocument82 pagesUse Case Modelling by Kurt Bittner and Ian SpenceShuryEndosNo ratings yet
- 2790-Article Text-11162-1-10-20110209 PDFDocument6 pages2790-Article Text-11162-1-10-20110209 PDFTushar BallabhNo ratings yet
- Use Cases: A. Modeling The Behavior of A System by Using Use Case DiagramsDocument3 pagesUse Cases: A. Modeling The Behavior of A System by Using Use Case Diagramsnikole ariana chavezNo ratings yet
- SE&CT Chapter 03Document53 pagesSE&CT Chapter 03Ḿūĵṫấßấ ĀßȋdȋNo ratings yet
- Managing Inconsistencies in UML ModelsDocument18 pagesManaging Inconsistencies in UML ModelssoftNo ratings yet
- Use Case Diagram TutorialDocument10 pagesUse Case Diagram TutorialHailu BadyeNo ratings yet
- System Models PDFDocument17 pagesSystem Models PDFJuarniey WangNo ratings yet
- Faysal Bank LimitedDocument3 pagesFaysal Bank LimitedAsif JavaidNo ratings yet
- Lecture-07 - Software EngineeringDocument50 pagesLecture-07 - Software Engineeringjamesboss207No ratings yet
- Modelling The Hospital Into The Future With UMLDocument12 pagesModelling The Hospital Into The Future With UMLRony ChuquínNo ratings yet
- Hospital Information System: Full ReportDocument9 pagesHospital Information System: Full ReportFarheen AhmedNo ratings yet
- A Methods of Ensuring Consistency Between UML Diagrams: April 2018Document12 pagesA Methods of Ensuring Consistency Between UML Diagrams: April 2018Maxwell MabhikwaNo ratings yet
- System Modelling Ch5Document53 pagesSystem Modelling Ch5Deniecia FrancisNo ratings yet
- Unit 3 - Design and CodingDocument26 pagesUnit 3 - Design and Coding160 NikeshNo ratings yet
- Analysis and Design For Object-Oriented Multi-Tier Architecture of Public Opinion Survey System Based On UMLDocument5 pagesAnalysis and Design For Object-Oriented Multi-Tier Architecture of Public Opinion Survey System Based On UMLJemy ArieswantoNo ratings yet
- Chapter 5: System ModelingDocument55 pagesChapter 5: System Modelingnabaraj negiNo ratings yet
- Chapter 5Document28 pagesChapter 5Feras JbourNo ratings yet
- Discrete-Event Simulation of HealthDocument42 pagesDiscrete-Event Simulation of Health6551209251No ratings yet
- Emdedded AssignDocument19 pagesEmdedded AssignPayal SainiNo ratings yet
- Transforming Use Case Models To Class Models and OCL-SpecificationsDocument25 pagesTransforming Use Case Models To Class Models and OCL-Specificationsجعفر عباسNo ratings yet
- System Modelling IDocument47 pagesSystem Modelling IBebo AkramNo ratings yet
- On Use Cases and Their Relationships in The Unified Modelling LanguageDocument16 pagesOn Use Cases and Their Relationships in The Unified Modelling LanguageHannah Esey Aquino PaquinNo ratings yet
- System MOdelingDocument73 pagesSystem MOdelingSadaf ManoNo ratings yet
- Chapter 4 - System Requirements and Modeling - Part 1: Principles of Software EngineeringDocument24 pagesChapter 4 - System Requirements and Modeling - Part 1: Principles of Software Engineeringthe endNo ratings yet
- Simula Approve 20Document17 pagesSimula Approve 20TAN NGUYEN NHATNo ratings yet
- Alter 2012Document19 pagesAlter 2012Anish MonachanNo ratings yet
- Lecture-2: Introduction To Data ScienceDocument32 pagesLecture-2: Introduction To Data ScienceSaif Ali KhanNo ratings yet
- Lecture-6: Introduction To Data ScienceDocument25 pagesLecture-6: Introduction To Data ScienceSaif Ali KhanNo ratings yet
- Lecture-5: Introduction To Data ScienceDocument28 pagesLecture-5: Introduction To Data ScienceSaif Ali KhanNo ratings yet
- Lecture-4: Introduction To Data ScienceDocument41 pagesLecture-4: Introduction To Data ScienceSaif Ali KhanNo ratings yet
- Difference Between System Call and Procedure CallDocument4 pagesDifference Between System Call and Procedure CallSaif Ali KhanNo ratings yet
- Machine LearningDocument36 pagesMachine LearningSaif Ali KhanNo ratings yet
- Machine LearningDocument19 pagesMachine LearningSaif Ali KhanNo ratings yet
- Concepts and Techniques: - Chapter 3Document63 pagesConcepts and Techniques: - Chapter 3Sudhakar TripathiNo ratings yet
- K-Nearest NeighborDocument12 pagesK-Nearest NeighborSaif Ali KhanNo ratings yet
- Machine LearningDocument31 pagesMachine LearningSaif Ali KhanNo ratings yet
- Chapter 12: Binary Search TreesDocument26 pagesChapter 12: Binary Search TreesAqil SiddiquiNo ratings yet
- Concepts and Techniques: - Chapter 4Document58 pagesConcepts and Techniques: - Chapter 4shyamNo ratings yet
- Concepts and Techniques: - Chapter 1Document41 pagesConcepts and Techniques: - Chapter 1Tolga YılmazNo ratings yet
- Concepts and Techniques: - Chapter 2Document65 pagesConcepts and Techniques: - Chapter 2napsterNo ratings yet
- CS4043D Course PlanDocument2 pagesCS4043D Course PlanSaif Ali KhanNo ratings yet
- Machine LearningDocument36 pagesMachine LearningSaif Ali KhanNo ratings yet
- End Semester Exam CS 3007 D Object Oriented SystemsDocument1 pageEnd Semester Exam CS 3007 D Object Oriented SystemsSaif Ali KhanNo ratings yet
- CS 4061D AssignmentDocument2 pagesCS 4061D AssignmentSaif Ali KhanNo ratings yet
- TutorialDocument2 pagesTutorialSaif Ali KhanNo ratings yet
- Cs4044D Machine LearningDocument3 pagesCs4044D Machine LearningSaif Ali KhanNo ratings yet
- K-Nearest NeighborDocument12 pagesK-Nearest NeighborSaif Ali KhanNo ratings yet
- CS 4061D AssignmentDocument2 pagesCS 4061D AssignmentSaif Ali KhanNo ratings yet
- Graph Theory and Social Networks: Alexandru CostanDocument28 pagesGraph Theory and Social Networks: Alexandru CostanSaif Ali KhanNo ratings yet
- Machine LearningDocument19 pagesMachine LearningSaif Ali KhanNo ratings yet
- K-Nearest NeighborDocument12 pagesK-Nearest NeighborSaif Ali KhanNo ratings yet
- Machine LearningDocument31 pagesMachine LearningSaif Ali KhanNo ratings yet
- Chapter 8Document75 pagesChapter 8Saif Ali KhanNo ratings yet
- Chapter 6: The Relational Algebra and Relational CalculusDocument11 pagesChapter 6: The Relational Algebra and Relational CalculusMuhammad Rico SalahuddinNo ratings yet
- Image Processing Assignment-1Document5 pagesImage Processing Assignment-1Saif Ali KhanNo ratings yet
- Design and Implementation of Electronic Billing SystemDocument64 pagesDesign and Implementation of Electronic Billing SystemDamilola AdegbemileNo ratings yet
- Audience Behavior Mining: Integrating TV Ratings With Multimedia ContentDocument274 pagesAudience Behavior Mining: Integrating TV Ratings With Multimedia ContentkkNo ratings yet
- Project - Proposal - For - A - Library System.Document12 pagesProject - Proposal - For - A - Library System.Chala Geta100% (5)
- DoDAF TutorialDocument126 pagesDoDAF Tutorialksenthil77No ratings yet
- Dormitory Management System Proposal For DBUDocument88 pagesDormitory Management System Proposal For DBUBishri Mohammed100% (2)
- Systems Analysis and Design With UML, 4th Edition Chapter 1 Question SolutionDocument14 pagesSystems Analysis and Design With UML, 4th Edition Chapter 1 Question SolutionStanleyYeung100% (2)
- OOAD Sample PaperDocument23 pagesOOAD Sample PaperHassan Bin RaeesNo ratings yet
- Isa 95.00.02-2010Document186 pagesIsa 95.00.02-2010Hector Tostado100% (1)
- Åα¿½«ªÑ¡¿Ñ 1Document127 pagesÅα¿½«ªÑ¡¿Ñ 1Tung Vo An ThanhNo ratings yet
- Using RoseDocument120 pagesUsing RoseSantosh KumarNo ratings yet
- Practical No.4 Introducion To Class Diagrams: MembersDocument23 pagesPractical No.4 Introducion To Class Diagrams: MembersManmit KaurNo ratings yet
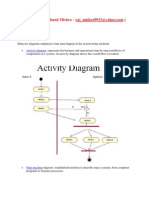
- Activity AnalysisDocument11 pagesActivity AnalysisEd Doloriel Morales100% (2)
- Functional Modelling (Unit 2)Document7 pagesFunctional Modelling (Unit 2)Shivam RajputNo ratings yet
- The Unified Modeling LanguageDocument6 pagesThe Unified Modeling LanguageRoya Jaferi0% (1)
- As ISO 15745.1-2004 Industrial Automation Systems and Integration - Open Systems Application Integration FramDocument10 pagesAs ISO 15745.1-2004 Industrial Automation Systems and Integration - Open Systems Application Integration FramSAI Global - APACNo ratings yet
- Iso 19100 Series of Geographic Information Standards: (Submitted by The Secretariat)Document17 pagesIso 19100 Series of Geographic Information Standards: (Submitted by The Secretariat)Sella SerafinaNo ratings yet
- UT Dallas Syllabus For cs6359.002.09s Taught by (rxb080100)Document6 pagesUT Dallas Syllabus For cs6359.002.09s Taught by (rxb080100)UT Dallas Provost's Technology GroupNo ratings yet
- Rental House Management SystemDocument39 pagesRental House Management SystemYoha Teferi100% (2)
- The Software Development BookDocument27 pagesThe Software Development BookConcern ShokoNo ratings yet
- Unit-5 STM To FollowDocument48 pagesUnit-5 STM To FollowTułäsiŕäm RamuNo ratings yet
- Chatterbox in JavaDocument60 pagesChatterbox in JavaPawan SinghNo ratings yet
- Introduction To Rational RoseDocument7 pagesIntroduction To Rational RoseMukesh KumarNo ratings yet
- Online SystemDocument35 pagesOnline SystemPravashSahoo100% (1)
- Pos System (Shoe Retail System) Documentation: November 2015Document28 pagesPos System (Shoe Retail System) Documentation: November 2015Adnan RaiNo ratings yet
- Final Dorcot RepotDocument60 pagesFinal Dorcot RepotSabbir KhanNo ratings yet
- Software Project Management: SyllabusDocument6 pagesSoftware Project Management: SyllabusAnonymous rFt9CaE1No ratings yet
- Regulations - 2008Document82 pagesRegulations - 2008BubbyOshinNo ratings yet
- Course Plan of Object Oriented Software Engineering I Me CseDocument4 pagesCourse Plan of Object Oriented Software Engineering I Me CsesurendiranNo ratings yet
- CS8592-OOAD Question Bank With AnsDocument14 pagesCS8592-OOAD Question Bank With Anssaran SanjayNo ratings yet
- STA 101 Module 3 System Integration and ArchitectureDocument20 pagesSTA 101 Module 3 System Integration and ArchitectureRogin Llorico UbamosNo ratings yet
- $100M Offers: How to Make Offers So Good People Feel Stupid Saying NoFrom Everand$100M Offers: How to Make Offers So Good People Feel Stupid Saying NoRating: 5 out of 5 stars5/5 (21)
- The Millionaire Fastlane, 10th Anniversary Edition: Crack the Code to Wealth and Live Rich for a LifetimeFrom EverandThe Millionaire Fastlane, 10th Anniversary Edition: Crack the Code to Wealth and Live Rich for a LifetimeRating: 4.5 out of 5 stars4.5/5 (88)
- $100M Leads: How to Get Strangers to Want to Buy Your StuffFrom Everand$100M Leads: How to Get Strangers to Want to Buy Your StuffRating: 5 out of 5 stars5/5 (17)
- The Coaching Habit: Say Less, Ask More & Change the Way You Lead ForeverFrom EverandThe Coaching Habit: Say Less, Ask More & Change the Way You Lead ForeverRating: 4.5 out of 5 stars4.5/5 (186)
- Speaking Effective English!: Your Guide to Acquiring New Confidence In Personal and Professional CommunicationFrom EverandSpeaking Effective English!: Your Guide to Acquiring New Confidence In Personal and Professional CommunicationRating: 4.5 out of 5 stars4.5/5 (74)
- 12 Months to $1 Million: How to Pick a Winning Product, Build a Real Business, and Become a Seven-Figure EntrepreneurFrom Everand12 Months to $1 Million: How to Pick a Winning Product, Build a Real Business, and Become a Seven-Figure EntrepreneurRating: 4 out of 5 stars4/5 (2)
- The First Minute: How to start conversations that get resultsFrom EverandThe First Minute: How to start conversations that get resultsRating: 4.5 out of 5 stars4.5/5 (57)
- How to Talk to Anyone at Work: 72 Little Tricks for Big Success Communicating on the JobFrom EverandHow to Talk to Anyone at Work: 72 Little Tricks for Big Success Communicating on the JobRating: 4.5 out of 5 stars4.5/5 (36)
- Broken Money: Why Our Financial System Is Failing Us and How We Can Make It BetterFrom EverandBroken Money: Why Our Financial System Is Failing Us and How We Can Make It BetterRating: 5 out of 5 stars5/5 (1)
- Summary of Zero to One: Notes on Startups, or How to Build the FutureFrom EverandSummary of Zero to One: Notes on Startups, or How to Build the FutureRating: 4.5 out of 5 stars4.5/5 (100)
- Fascinate: How to Make Your Brand Impossible to ResistFrom EverandFascinate: How to Make Your Brand Impossible to ResistRating: 5 out of 5 stars5/5 (1)