0% found this document useful (0 votes)
4K views4 pagesFamily Planning Service Record Form
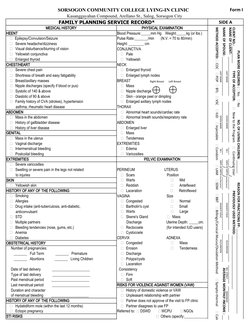
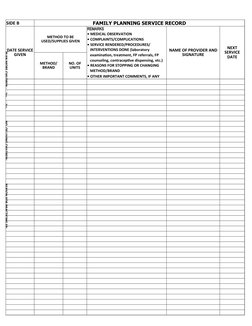
The document is a medical form for family planning services at Sorsogon Community College Lying-In Clinic. It collects information such as medical history, physical examination findings, method of family planning accepted, and details of the client such as name, age, number of living children, and reason for practicing family planning. The form has sections to document findings from examinations of various body systems and organs including HEENT, chest, heart, abdomen, genitals, extremities, pelvis, and skin. Physical measurements such as blood pressure, pulse, height, and weight are also recorded.
Uploaded by
Barangay Lam-anCopyright
© © All Rights Reserved
We take content rights seriously. If you suspect this is your content, claim it here.
Available Formats
Download as XLSX, PDF, TXT or read online on Scribd
0% found this document useful (0 votes)
4K views4 pagesFamily Planning Service Record Form
The document is a medical form for family planning services at Sorsogon Community College Lying-In Clinic. It collects information such as medical history, physical examination findings, method of family planning accepted, and details of the client such as name, age, number of living children, and reason for practicing family planning. The form has sections to document findings from examinations of various body systems and organs including HEENT, chest, heart, abdomen, genitals, extremities, pelvis, and skin. Physical measurements such as blood pressure, pulse, height, and weight are also recorded.
Uploaded by
Barangay Lam-anCopyright
© © All Rights Reserved
We take content rights seriously. If you suspect this is your content, claim it here.
Available Formats
Download as XLSX, PDF, TXT or read online on Scribd