You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5796)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Jose Rizal University: ODC Form 2ADocument3 pagesJose Rizal University: ODC Form 2AJonieP84No ratings yet
- Jose Rizal University: ODC Form 2BDocument3 pagesJose Rizal University: ODC Form 2BJonieP84No ratings yet
- Jose Rizal University: ODC Form 1CDocument3 pagesJose Rizal University: ODC Form 1CJonieP84No ratings yet
- Jose Rizal University: ODC Form 1ADocument2 pagesJose Rizal University: ODC Form 1AJonieP84No ratings yet
- Jose Rizal University: ODC Form 1BDocument3 pagesJose Rizal University: ODC Form 1BJonieP84No ratings yet
- List of Foods That Burn Fat: Fat FightersDocument4 pagesList of Foods That Burn Fat: Fat FightersJonieP84100% (1)
- Losartan Potassium Drug StudyDocument2 pagesLosartan Potassium Drug StudyJonieP84100% (4)
- Appearance of A Newborn: Presented by The Group 4Document40 pagesAppearance of A Newborn: Presented by The Group 4JonieP84No ratings yet
- Amlodipine Besylate Drug StudyDocument2 pagesAmlodipine Besylate Drug StudyJonieP84No ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Written Examination Handbook For General Dentistry May 2021-MinDocument20 pagesWritten Examination Handbook For General Dentistry May 2021-MinMuhammad Hassan memonNo ratings yet
- Underlying Contributors To Childhood Stunting: What Evidence Exists On Nutrition-Sensitive Risk Factors?Document12 pagesUnderlying Contributors To Childhood Stunting: What Evidence Exists On Nutrition-Sensitive Risk Factors?Andi Fahira NurNo ratings yet
- Q.P. CODE 1764 Question Bank For Ii Year B.SC Nursing Community Health Nursing-I Unit-I Short Answers (2 Marks)Document22 pagesQ.P. CODE 1764 Question Bank For Ii Year B.SC Nursing Community Health Nursing-I Unit-I Short Answers (2 Marks)Nilakshi Barik Mandal100% (1)
- Private Duty NursingDocument6 pagesPrivate Duty NursingKate Ocampo0% (1)
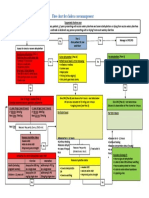
- Appendix 11. Flow Chart For Cholera Case ManagementDocument1 pageAppendix 11. Flow Chart For Cholera Case ManagementGerard Pio Wee100% (1)
- Woorksheet G10Document2 pagesWoorksheet G10Josielyn Camara DistorNo ratings yet
- Normal Birth As A Cultural PhenomenonDocument8 pagesNormal Birth As A Cultural PhenomenonMaria Johanna SchoutenNo ratings yet
- Aged Care QuestionsDocument9 pagesAged Care QuestionsElie RizkNo ratings yet
- Sterile Processing Technician or Medical Supply Technician or MeDocument3 pagesSterile Processing Technician or Medical Supply Technician or Meapi-77583771No ratings yet
- Dental Pre-Certification FormDocument4 pagesDental Pre-Certification FormSteve HyipNo ratings yet
- Competency-Based Training in Basic Emergency Obstetric and Newborn Care (BEmONC) Improves Porvers' Performance in Tanzania (Poster Version)Document1 pageCompetency-Based Training in Basic Emergency Obstetric and Newborn Care (BEmONC) Improves Porvers' Performance in Tanzania (Poster Version)JhpiegoNo ratings yet
- Selena-Sledai : A Tool To Assess Disease Activity in Patients With SLEDocument2 pagesSelena-Sledai : A Tool To Assess Disease Activity in Patients With SLELe DungNo ratings yet
- Health Belief ModelDocument12 pagesHealth Belief ModelNarjina Begam100% (1)
- Emergency and Disaster NursingDocument9 pagesEmergency and Disaster NursingDempsey AlmirañezNo ratings yet
- Male InfertilityDocument17 pagesMale InfertilityIda Bagus Putu SwabawaNo ratings yet
- Autism Spectrum Disorders (ASD) Presented By: Amanda WilkinsDocument16 pagesAutism Spectrum Disorders (ASD) Presented By: Amanda WilkinsiedaNo ratings yet
- 2-3. Principles of Tooth Preparation Part I & II DR SghaireenDocument69 pages2-3. Principles of Tooth Preparation Part I & II DR SghaireenMAJEED ALANZINo ratings yet
- Needle Stick Injuries Among Healthcare Waste Handlers in A Tertiary Care Hospital of DelhiDocument4 pagesNeedle Stick Injuries Among Healthcare Waste Handlers in A Tertiary Care Hospital of DelhiAdvanced Research PublicationsNo ratings yet
- Philippines EMS SystemDocument25 pagesPhilippines EMS SystemErnan BaldomeroNo ratings yet
- Bubonic PlagueDocument15 pagesBubonic Plagueapi-283967550No ratings yet
- Ppe Training Record: Department Occupation Type of Ppe Make/Model Name InitialsDocument3 pagesPpe Training Record: Department Occupation Type of Ppe Make/Model Name Initialsvlad100% (1)
- Assessment of HearingDocument51 pagesAssessment of HearingSwetha PasupuletiNo ratings yet
- Physical Wellness ChecklistDocument2 pagesPhysical Wellness ChecklistAndrea Fleur Du Mal100% (1)
- Application Letter CCMCDocument6 pagesApplication Letter CCMCgillan jonnel satinitiganNo ratings yet
- 10 Low-Fat Cheese Types For Weight Loss - Eat This Not ThatDocument1 page10 Low-Fat Cheese Types For Weight Loss - Eat This Not Thatsabita ojhaNo ratings yet
- Here Are The Pediatric Nursing BulletsDocument4 pagesHere Are The Pediatric Nursing BulletsMary Janine Joy RimanoNo ratings yet
- Tangcay Tenorio. Teves Group 4 C1 Concept Map On Hydatidiform MoleDocument11 pagesTangcay Tenorio. Teves Group 4 C1 Concept Map On Hydatidiform MoleJoi Owen TevesNo ratings yet
- UNIT 1 - Week (1-3) : Introduction To General Toxicology Intended Learning Outcomes (ILO)Document19 pagesUNIT 1 - Week (1-3) : Introduction To General Toxicology Intended Learning Outcomes (ILO)Hannah Jean Lapenid LemorenasNo ratings yet
- Usmle Step 1 Syllabus OutlineDocument38 pagesUsmle Step 1 Syllabus OutlineAsish GeiorgeNo ratings yet
- MT MLT RefDocument3 pagesMT MLT RefMystic MilanNo ratings yet