You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- DOMINGO - OB RequirmentsDocument10 pagesDOMINGO - OB RequirmentsJick Esteva de VicenteNo ratings yet
- Isometric Plumbing LayoutDocument1 pageIsometric Plumbing LayoutFrancis Philippe Cruzana CariñoNo ratings yet
- LABOR Room - ANDRADEDocument5 pagesLABOR Room - ANDRADEArje Lans AndradeNo ratings yet
- HOPE 2 Module 8Document8 pagesHOPE 2 Module 8Ojoy PersiaNo ratings yet
- Understanding Mycobacterium tuberculosis: Causative Agent, Risk Factors, Symptoms, Diagnosis and TreatmentDocument20 pagesUnderstanding Mycobacterium tuberculosis: Causative Agent, Risk Factors, Symptoms, Diagnosis and TreatmentDivya TiwariNo ratings yet
- Enhance settling tank performance with proper designDocument4 pagesEnhance settling tank performance with proper designJanaisha Bai TitoNo ratings yet
- Coronavirus Disease 2020 (COVID-19) : China National Pharmaceutical Group Co - LTD (SINOPHARM)Document20 pagesCoronavirus Disease 2020 (COVID-19) : China National Pharmaceutical Group Co - LTD (SINOPHARM)Anusheh Asad100% (1)
- The Purpose of International OrganizationsDocument3 pagesThe Purpose of International OrganizationsMuhammad HabibiNo ratings yet
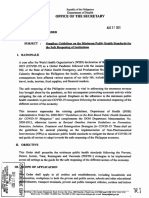
- DOH Administrative Order No 2024 0043Document44 pagesDOH Administrative Order No 2024 0043Jasper John HerreraNo ratings yet
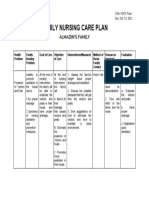
- FAMILY NURSING CARE PLAN - Almadin's FamilyDocument1 pageFAMILY NURSING CARE PLAN - Almadin's FamilyAngeline TaghapNo ratings yet
- Baccalaureat Session De: Juin 2018 EPREUVE DE: Anglais Series: D/CDocument3 pagesBaccalaureat Session De: Juin 2018 EPREUVE DE: Anglais Series: D/ClouyachrisnaNo ratings yet
- Chapter 8-1Document39 pagesChapter 8-1chindypermataNo ratings yet
- Sources of Epidemiological DataDocument3 pagesSources of Epidemiological Datageorgeloto1283% (6)
- Accenture Climate Change and HealthDocument40 pagesAccenture Climate Change and HealthShivraj JadhavNo ratings yet
- Assessment of Non Revenue Water in District Meter Area DmaDocument4 pagesAssessment of Non Revenue Water in District Meter Area DmaSekretariat SPSPNo ratings yet
- THE PHYSICAL AND SEXUAL SELFDocument20 pagesTHE PHYSICAL AND SEXUAL SELFsigma rusNo ratings yet
- UAS Genap Semester II Kebidanan STIKES HafshawatyDocument3 pagesUAS Genap Semester II Kebidanan STIKES HafshawatyHanna HannaNo ratings yet
- Understanding Disease Transmission DynamicsDocument14 pagesUnderstanding Disease Transmission Dynamicswulanda septianiNo ratings yet
- Project ReportDocument16 pagesProject Reportshaqib71% (7)
- DR Lal Pathlabs: InterpretationDocument2 pagesDR Lal Pathlabs: InterpretationSantanu MondalNo ratings yet
- Family PlanningDocument59 pagesFamily PlanningDhruva PatelNo ratings yet
- Family Nursing Care PlanDocument3 pagesFamily Nursing Care PlanColleen De la Rosa100% (1)
- Stunting 1 Pendampingan PT 2019 PDFDocument79 pagesStunting 1 Pendampingan PT 2019 PDFDany DiasNo ratings yet
- Community Medicine 2022Document8 pagesCommunity Medicine 2022Ashirwad DadeiaNo ratings yet
- Public Health, Health and LifestyleDocument149 pagesPublic Health, Health and LifestyleBrian MaloneyNo ratings yet
- San Isidro High School Summative Health TestDocument2 pagesSan Isidro High School Summative Health TestDennis Mark Dela CruzNo ratings yet
- FINAL-Edited - SLeM1 - PE10 - Quarter1 (1) Edited by RUFO JOHN PAULDocument11 pagesFINAL-Edited - SLeM1 - PE10 - Quarter1 (1) Edited by RUFO JOHN PAULMaze PhonfoNo ratings yet
- Trabajo de InglesDocument9 pagesTrabajo de InglesCoronado Ramirez, Jesús DavidNo ratings yet
- Cleveland City Council Legislation: Free Feminine Hygiene ProductsDocument4 pagesCleveland City Council Legislation: Free Feminine Hygiene ProductsWKYC.comNo ratings yet
- Fibroid With PregnancyDocument5 pagesFibroid With PregnancyvaishaliNo ratings yet