You might also like
- Issue Trauma Kepala2019Document9 pagesIssue Trauma Kepala2019Siska Prima OlimvianiNo ratings yet
- Issue Trauma Kepala2019Document9 pagesIssue Trauma Kepala2019Siska Prima OlimvianiNo ratings yet
- Issue Trauma Kepala2019Document6 pagesIssue Trauma Kepala2019Siska Prima OlimvianiNo ratings yet
- Young Adults' Perspectives On Health-Related QualityDocument9 pagesYoung Adults' Perspectives On Health-Related QualitySiska Prima OlimvianiNo ratings yet
- Jurnal Trauma Head2020Document30 pagesJurnal Trauma Head2020Siska Prima OlimvianiNo ratings yet
- Jurnal Trauma Head2020Document30 pagesJurnal Trauma Head2020Siska Prima OlimvianiNo ratings yet
- Issue Trauma Kepala2019Document9 pagesIssue Trauma Kepala2019Siska Prima OlimvianiNo ratings yet
- Hamilton Anxiety Rating Scale (HAM-A)Document2 pagesHamilton Anxiety Rating Scale (HAM-A)Elsa Ameliana ManurungNo ratings yet
- Handheld Finger Anxiety CoroDocument9 pagesHandheld Finger Anxiety CoroSiska Prima OlimvianiNo ratings yet
- Avender On Anxiety and Pain in AngiographyDocument25 pagesAvender On Anxiety and Pain in AngiographySiska Prima OlimvianiNo ratings yet
- OsisjsjDocument11 pagesOsisjsjZulian ZarotNo ratings yet
- Hubungan Beban Kerja Mental Terhadap Stres Kerja Pada Tenaga Kependidikan Di Kota BatamDocument8 pagesHubungan Beban Kerja Mental Terhadap Stres Kerja Pada Tenaga Kependidikan Di Kota BatamSiska Prima OlimvianiNo ratings yet
- Avender On Anxiety and Pain in AngiographyDocument25 pagesAvender On Anxiety and Pain in AngiographySiska Prima OlimvianiNo ratings yet
- Journal of Perianesthesia Nursing: ResearchDocument6 pagesJournal of Perianesthesia Nursing: ResearchSiska Prima OlimvianiNo ratings yet
- Analisis Hubungan Beban Kerja Mental Dengan Stres Kerja: Dikky FahamsyahDocument9 pagesAnalisis Hubungan Beban Kerja Mental Dengan Stres Kerja: Dikky FahamsyahbuNo ratings yet
- Perbedaan Intensitas Nyeri Antara Pemberian Terapi Back LaparatomiDocument12 pagesPerbedaan Intensitas Nyeri Antara Pemberian Terapi Back LaparatomiMulyro BiadinNo ratings yet
- View Topic Percutaneous Coronary Intervention Overview: December 2014Document49 pagesView Topic Percutaneous Coronary Intervention Overview: December 2014Siska Prima OlimvianiNo ratings yet
- Avender On Anxiety and Pain in AngiographyDocument25 pagesAvender On Anxiety and Pain in AngiographySiska Prima OlimvianiNo ratings yet
- Gadar 220190401Document7 pagesGadar 220190401muhammad pratamaNo ratings yet
- JJS Ex - Finger-Hold PDFDocument2 pagesJJS Ex - Finger-Hold PDFNaresh MuttavarapuNo ratings yet
- View Topic Percutaneous Coronary Intervention Overview: December 2014Document49 pagesView Topic Percutaneous Coronary Intervention Overview: December 2014Siska Prima OlimvianiNo ratings yet
- Handheld RelaxationDocument8 pagesHandheld RelaxationSiska Prima OlimvianiNo ratings yet
- OsisjsjDocument11 pagesOsisjsjZulian ZarotNo ratings yet
- Journal of Perianesthesia Nursing: ResearchDocument6 pagesJournal of Perianesthesia Nursing: ResearchSiska Prima OlimvianiNo ratings yet
- Gadar 220190401Document7 pagesGadar 220190401muhammad pratamaNo ratings yet
- OsisjsjDocument11 pagesOsisjsjZulian ZarotNo ratings yet
- State-Trait Anxiety Inventory: HistoryDocument9 pagesState-Trait Anxiety Inventory: HistorySiska Prima OlimvianiNo ratings yet
- 572 1403 1 SMDocument7 pages572 1403 1 SMNuruz Setsu Sullivaien MBNo ratings yet
- Perbedaan Intensitas Nyeri Antara Pemberian Terapi Back LaparatomiDocument12 pagesPerbedaan Intensitas Nyeri Antara Pemberian Terapi Back LaparatomiMulyro BiadinNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- OR AppendixDocument9 pagesOR AppendixDan HizonNo ratings yet
- Community Health Nursing ExamsDocument13 pagesCommunity Health Nursing ExamsAhrisJeannine EscuadroNo ratings yet
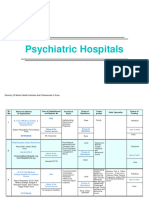
- Mental Health DirectoryDocument24 pagesMental Health DirectoryCMO Bestla GroupNo ratings yet
- HM 205 Hospital and Health System 2 2010Document4 pagesHM 205 Hospital and Health System 2 2010Madhurima ChakrabortyNo ratings yet
- Dialogue of Heart Failure Patients Accompanied by A Child With A NurseDocument2 pagesDialogue of Heart Failure Patients Accompanied by A Child With A NurseWilda NingsihNo ratings yet
- Cy 4Document110 pagesCy 4Ivy Marie TolentinoNo ratings yet
- V3 Medical Providers List Sep 2020 Jeddah&RiyadhDocument16 pagesV3 Medical Providers List Sep 2020 Jeddah&RiyadhcardossoNo ratings yet
- FDA To Authorize New Covid Boosters Without Trials in PeopleDocument3 pagesFDA To Authorize New Covid Boosters Without Trials in PeopleZsi GaNo ratings yet
- FDA Bans Times Natural Capsules, X Plus Men, OthersDocument2 pagesFDA Bans Times Natural Capsules, X Plus Men, OthersGhanaWeb EditorialNo ratings yet
- Adult Breathing Systems For Transport VentilatorsDocument4 pagesAdult Breathing Systems For Transport Ventilatorstaniamr11No ratings yet
- Minnie Germano New Resume 2023Document1 pageMinnie Germano New Resume 2023api-655682809No ratings yet
- Triage in The HospitalDocument15 pagesTriage in The HospitalCarie Manarondong100% (1)
- 22-Family MedicineDocument6 pages22-Family MedicineIbrahimFikryNo ratings yet
- Original PDF Psychiatric Mental Health Nursing Concepts of Care in Evidence Based Practice 9th PDFDocument41 pagesOriginal PDF Psychiatric Mental Health Nursing Concepts of Care in Evidence Based Practice 9th PDFjoseph.owens578100% (39)
- NIV MakassarDocument40 pagesNIV MakassarEmil LasulikaNo ratings yet
- Drugs For Life by Joseph DumitDocument42 pagesDrugs For Life by Joseph DumitDuke University Press44% (9)
- Thesis Topics in Dental Public HealthDocument4 pagesThesis Topics in Dental Public Healthaprilwatsonlittlerock100% (2)
- Indonesia Hospital NumberDocument1 pageIndonesia Hospital NumberShellyNo ratings yet
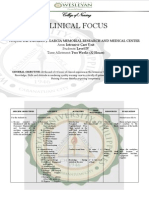
- Clinical Focus ICUDocument6 pagesClinical Focus ICUJan Rainier Carlos BalariaNo ratings yet
- PB1 - NP2Document12 pagesPB1 - NP2Denzelle ZchalletNo ratings yet
- HKGC Booklet FinalDocument95 pagesHKGC Booklet FinalAtik Badshah SHAIKHNo ratings yet
- Research Paper On Knowledge Management Practices in Pharma CompanyDocument7 pagesResearch Paper On Knowledge Management Practices in Pharma Companyafnhekkghifrbm100% (1)
- Deepu Pps Front PgesDocument6 pagesDeepu Pps Front PgesM. Shoeb SultanNo ratings yet
- Opioid Topic DiscussionDocument22 pagesOpioid Topic Discussionapi-587439953No ratings yet
- The Endocrine Society The Endocrine Society: PresentingDocument20 pagesThe Endocrine Society The Endocrine Society: PresentingRODMSANo ratings yet
- Syphilis Nursing ManagementDocument2 pagesSyphilis Nursing ManagementLizaEllaga67% (3)
- Provisional: Borderline Personality Disorder Differential DXDocument6 pagesProvisional: Borderline Personality Disorder Differential DXhernandez2812No ratings yet
- Text 918-553-8061Document4 pagesText 918-553-8061MD6No ratings yet
- Adam PharmaDocument18 pagesAdam PharmawaelajlanyNo ratings yet
- University of San Carlos Sample ThesisDocument5 pagesUniversity of San Carlos Sample Thesisafkneafpz100% (2)