You might also like
- Nursing Care Plan Assessment Diagnosis Inference Planning Interventio N Rationale EvaluationDocument3 pagesNursing Care Plan Assessment Diagnosis Inference Planning Interventio N Rationale EvaluationDianne100% (2)
- Nursing Care Plan: S.No Assessment Nursing Diagnosis Goal Interventions Implementations Rationale EvaluationDocument4 pagesNursing Care Plan: S.No Assessment Nursing Diagnosis Goal Interventions Implementations Rationale EvaluationPriyanka John100% (3)
- Generic Name Brand Name Dosage Indications Mechanisms of Action Adverse Effects Nursing ResponsibilitiesDocument10 pagesGeneric Name Brand Name Dosage Indications Mechanisms of Action Adverse Effects Nursing ResponsibilitiesJennalyn CasapaoNo ratings yet
- Nursing Care Plan for Breast Engorgement Pain ReliefDocument1 pageNursing Care Plan for Breast Engorgement Pain ReliefMarceline VueenNo ratings yet
- Nursing Care Plan For Pregnancy Induced HypertensionDocument9 pagesNursing Care Plan For Pregnancy Induced HypertensionMurugham DineshNo ratings yet
- Nursing Care Plan Placenta PreviaDocument2 pagesNursing Care Plan Placenta PreviaLei Ortega100% (3)
- Hyperemesis GravidarumDocument16 pagesHyperemesis GravidarumKristine Alejandro80% (5)
- Nursing Care Plan PrenatalDocument5 pagesNursing Care Plan PrenatalKim Galamgam100% (2)
- NCP - Placenta PreviaDocument3 pagesNCP - Placenta PreviaJulianna Alex ConopioNo ratings yet
- Nursing Process For A Client With Molar Pregnancy (H-Mole)Document24 pagesNursing Process For A Client With Molar Pregnancy (H-Mole)api-370148995% (19)
- Nursing Care Plan for Postoperative ComfortDocument1 pageNursing Care Plan for Postoperative ComfortAngela DancelNo ratings yet
- Hyperemesis Gravidarum 1Document26 pagesHyperemesis Gravidarum 1Jas Castro Jovero100% (3)
- NCP Case Study 1Document3 pagesNCP Case Study 1Kristinelou Reyna100% (5)
- Nursing Care Plan Abruptio PlacentaeDocument2 pagesNursing Care Plan Abruptio PlacentaeWann WannNo ratings yet
- Lesson Plan On Gestational DiabetesDocument7 pagesLesson Plan On Gestational DiabetesKinley Dorji100% (2)
- NCP 2013 ObDocument1 pageNCP 2013 ObSonny Dizon Pareñas100% (2)
- NCP: Puerperal InfectionDocument8 pagesNCP: Puerperal InfectionJavie83% (12)
- CARE PLAN ON Cord Prolapsed.Document14 pagesCARE PLAN ON Cord Prolapsed.priyanka100% (8)
- Post Partum Hemorrhage Nursing Care PlanDocument9 pagesPost Partum Hemorrhage Nursing Care PlanElli SuñgaNo ratings yet
- Nursing Care Plan: Submitted To: Submitted By: Ms Kamini Manisha Joshi Asst. Prof. Acn Msc. Nursing 1 SemesterDocument14 pagesNursing Care Plan: Submitted To: Submitted By: Ms Kamini Manisha Joshi Asst. Prof. Acn Msc. Nursing 1 SemesterDIMPYNo ratings yet
- Prenatal Nursing Care PlansDocument25 pagesPrenatal Nursing Care PlansRijane Tabonoc OmlangNo ratings yet
- Priorities List of Nursing DiagnosisDocument4 pagesPriorities List of Nursing DiagnosisValarmathiNo ratings yet
- A Case Study of Cesarean Delivery (Breech Presentation) : Submitted By: Corpus. NichelleDocument24 pagesA Case Study of Cesarean Delivery (Breech Presentation) : Submitted By: Corpus. NichelleFitriNo ratings yet
- Cs On RH IncompatibilityDocument17 pagesCs On RH IncompatibilityRupali Arora100% (2)
- Breastfeeding BibliographyDocument6 pagesBreastfeeding BibliographyPiyush DuttaNo ratings yet
- NCP PPHDocument2 pagesNCP PPHmikee-berredo-9975No ratings yet
- Pregnancy Induced Hypertension Nursing Care PlanDocument5 pagesPregnancy Induced Hypertension Nursing Care Planjohncarlo ramosNo ratings yet
- NCP For Ectopic PregnancyDocument4 pagesNCP For Ectopic PregnancyClarissa_Dante_735850% (4)
- Case Study 1Document29 pagesCase Study 1Patricia Ann Salazar Rn100% (3)
- Preeclampsia Nursing Care PlanDocument8 pagesPreeclampsia Nursing Care PlanElli SuñgaNo ratings yet
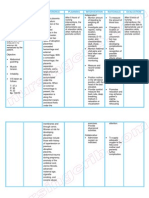
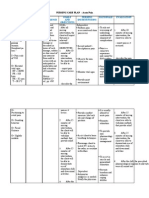
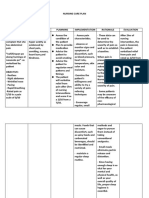
- NCP Preeclampsia and EclampsiaDocument16 pagesNCP Preeclampsia and EclampsiaBiway Regala100% (1)
- Abruptio Placenta Nursing Care PlanDocument2 pagesAbruptio Placenta Nursing Care PlanJharene Basbaño100% (5)
- Nursing Care Plan AbortionDocument4 pagesNursing Care Plan AbortionJane Casiquin100% (1)
- Abruptio Placenta NCP 2 FinalDocument19 pagesAbruptio Placenta NCP 2 FinalTin100% (1)
- Maternal Risk AssessmentDocument3 pagesMaternal Risk AssessmentMark FernandezNo ratings yet
- Nursing Care Plan Abrubtio PlacentaDocument2 pagesNursing Care Plan Abrubtio PlacentaLei Ortega0% (1)
- NCP Pain (H Mole)Document3 pagesNCP Pain (H Mole)Khat Quimen Mayo86% (7)
- Ectopic Pregnancy Nursing Care PlanDocument2 pagesEctopic Pregnancy Nursing Care PlanKim GalamgamNo ratings yet
- Postnatal ExaminationDocument19 pagesPostnatal ExaminationAlpha100% (1)
- Hyperemesis Gravidarum Case StudyDocument32 pagesHyperemesis Gravidarum Case StudyMonette Abalos Mendova89% (9)
- Eclampsia: Case Presentation Group ADocument56 pagesEclampsia: Case Presentation Group AArah Momo67% (3)
- Abruptio Placenta NCPDocument2 pagesAbruptio Placenta NCPNichole Audrey Saavedra100% (1)
- Nursing Goals for Pregnant Client with Nutritional and Sleep IssuesDocument6 pagesNursing Goals for Pregnant Client with Nutritional and Sleep IssuesRaja100% (5)
- Nursing Care Plan for Labor Pain ManagementDocument8 pagesNursing Care Plan for Labor Pain ManagementDickson,Emilia Jade100% (1)
- Nursing Care Plan Dysfunctional Uterine BleedingDocument2 pagesNursing Care Plan Dysfunctional Uterine BleedingLei Ortega68% (25)
- Nursing Diagnosis: May Be Related To: Fluid Volume Deficit (Isotonic)Document26 pagesNursing Diagnosis: May Be Related To: Fluid Volume Deficit (Isotonic)Ric Nacional75% (4)
- Case StudyDocument21 pagesCase StudyKavi rajput100% (3)
- 2 - EndometriosisDocument3 pages2 - EndometriosisJayson Olile100% (1)
- Antenatal Case PresentationDocument10 pagesAntenatal Case PresentationRijane Tabonoc OmlangNo ratings yet
- NCP 28Document9 pagesNCP 28Leanne Joie Lozano100% (1)
- NCP On Imbalanced Nutrition: Less Than A Body Requirements R/T Inability To Ingest FoodDocument1 pageNCP On Imbalanced Nutrition: Less Than A Body Requirements R/T Inability To Ingest FoodErle Gray CadangenNo ratings yet
- Nursing Diagnosis, Goals, and Interventions for Acute Pain, Nutrition Imbalance, and Fluid Volume DeficitDocument5 pagesNursing Diagnosis, Goals, and Interventions for Acute Pain, Nutrition Imbalance, and Fluid Volume DeficitAngelica ValeraNo ratings yet
- Nursing DignosisDocument5 pagesNursing DignosisvishnukulakkadaNo ratings yet
- Name: Babu Kaji Maharjan: Patient's IdentificationDocument6 pagesName: Babu Kaji Maharjan: Patient's IdentificationAlisha MaharjanNo ratings yet
- Name: Garanchon, Ceyan Peaches BSN2DDocument3 pagesName: Garanchon, Ceyan Peaches BSN2DXeyanNo ratings yet
- Nursing Care Plan: Rochelle Maglangit RagoDocument2 pagesNursing Care Plan: Rochelle Maglangit RagoRochelle RagoNo ratings yet
- Nursing Care Plan Assessment Nursing Diagnosis Rationale Plan of Care Nursing Intervention Rationale Evaluation Subjective DataDocument4 pagesNursing Care Plan Assessment Nursing Diagnosis Rationale Plan of Care Nursing Intervention Rationale Evaluation Subjective DataSophia PandesNo ratings yet
- Assess The Plan To Provide Advice The Advice TheDocument3 pagesAssess The Plan To Provide Advice The Advice TheDarwin QuirimitNo ratings yet
- Case Study No.10 (NCP)Document5 pagesCase Study No.10 (NCP)Rosemarie R. Reyes100% (1)
- Knowledge DeficitDocument2 pagesKnowledge DeficitSahara Sahjz Macabangun67% (3)
- NUR260-Capstone Test 3Document16 pagesNUR260-Capstone Test 3Carole EmenikeNo ratings yet
- Ajmg A 61300Document9 pagesAjmg A 61300Nigel GarayNo ratings yet
- ACOG Practice Bulletin No. 212 Summary - Pregnancy and Heart DiseaseDocument6 pagesACOG Practice Bulletin No. 212 Summary - Pregnancy and Heart DiseaseYuly Andrea Marquez CastañedaNo ratings yet
- BSN 2-4 - 2V - MCN CASE STUDY (Final)Document100 pagesBSN 2-4 - 2V - MCN CASE STUDY (Final)Angeline ShackletonNo ratings yet
- Teenege PregnancyDocument3 pagesTeenege PregnancyJairah LuzNo ratings yet
- Guinea Pig DissertationDocument78 pagesGuinea Pig Dissertationcreatingcreator100% (1)
- MCN Reviewer DefinitionOfTermsDocument10 pagesMCN Reviewer DefinitionOfTermsJenessel Ann P DaugNo ratings yet
- Health exam questions on family, relationships and drugsDocument16 pagesHealth exam questions on family, relationships and drugsPENTIL HIGH SCHOOLNo ratings yet
- Chn211 Transes - PrelimsDocument42 pagesChn211 Transes - Prelimsrelynmasula02No ratings yet
- High Risk Prenatal CareDocument4 pagesHigh Risk Prenatal CareKatherine Gayle GuiaNo ratings yet
- I Year BBA LL. B. (Hons.) - Semester-II (2020-21) Constitutional Law: Internal Assignment-IIDocument13 pagesI Year BBA LL. B. (Hons.) - Semester-II (2020-21) Constitutional Law: Internal Assignment-IIshrisanjanaNo ratings yet
- Screening of High-Risk Pregnancy, Newer Modalities of DiagnosisDocument12 pagesScreening of High-Risk Pregnancy, Newer Modalities of DiagnosisSanthosh.S.U100% (9)
- NeoPREP 2011Document342 pagesNeoPREP 2011johnbarrow641No ratings yet
- Yoga For Pregnant Ladies EnglishDocument44 pagesYoga For Pregnant Ladies EnglishDrAjey BhatNo ratings yet
- (OBS) 1.09 Pre-Conceptional Counselling & Prenatal Care - Bongala (Sep 8)Document16 pages(OBS) 1.09 Pre-Conceptional Counselling & Prenatal Care - Bongala (Sep 8)Noreen Hannah GabrielNo ratings yet
- Impacts of Antenatal Nursing Interventions On Mothers ' Breastfeeding Self-Efficacy: An Experimental StudyDocument12 pagesImpacts of Antenatal Nursing Interventions On Mothers ' Breastfeeding Self-Efficacy: An Experimental StudyevaNo ratings yet
- A. B. A. B.: Obstetric NursingDocument9 pagesA. B. A. B.: Obstetric NursingAtivon AlracNo ratings yet
- Random FactsDocument298 pagesRandom FactsglemeseNo ratings yet
- Infertility Project PDFDocument11 pagesInfertility Project PDFSunil KumarNo ratings yet
- 3rd Lesson Assessing Child Bearing WomenDocument6 pages3rd Lesson Assessing Child Bearing WomendaningdubouzetNo ratings yet
- ICD10WHO2007 TnI4Document1,656 pagesICD10WHO2007 TnI4Kanok SongprapaiNo ratings yet
- 5249 13639 2 PBDocument3 pages5249 13639 2 PBBeti KristinawatiNo ratings yet
- Allianz Global Assistance International Travel Insurance SummaryDocument40 pagesAllianz Global Assistance International Travel Insurance SummaryIvory PlatypusNo ratings yet
- Case StudyDocument26 pagesCase StudyGrace Orencia100% (1)
- Novorapid Product Monograph PDFDocument50 pagesNovorapid Product Monograph PDFAtid AmandaNo ratings yet
- Fetal Development Week-By-Week Stages of PregnancyDocument11 pagesFetal Development Week-By-Week Stages of Pregnancysam8833No ratings yet
- Prevalence of Anemia Among Pregnant Women Attending Antenatal Care at Tikur Anbessa Specialized Hospital Addis Ababa Ethiopia 2329 8790.1000125Document6 pagesPrevalence of Anemia Among Pregnant Women Attending Antenatal Care at Tikur Anbessa Specialized Hospital Addis Ababa Ethiopia 2329 8790.1000125thaynara robertoNo ratings yet
- Ginecologia Womens Imaging Obstetrics and Gynecology PDFDocument198 pagesGinecologia Womens Imaging Obstetrics and Gynecology PDFAndrei MurariuNo ratings yet
- Clear My Choice: Not Yet Answered Marked Out of 1.00Document7 pagesClear My Choice: Not Yet Answered Marked Out of 1.00medodiabNo ratings yet
- SaluEric New An Alluring Imp WPS Office 1Document7 pagesSaluEric New An Alluring Imp WPS Office 1Eric SaludaresNo ratings yet