You might also like
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Flowsimulator Framework For Massively Parallel CFD ApplicationsDocument5 pagesThe Flowsimulator Framework For Massively Parallel CFD Applications43No ratings yet
- En 1822-1 (2019) (E)Document8 pagesEn 1822-1 (2019) (E)430% (1)
- HDUWJHDocument1 pageHDUWJH43No ratings yet
- Table of Contents: Infoprint 1822Document168 pagesTable of Contents: Infoprint 182243No ratings yet
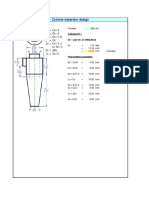
- CYCLONE Drawing v0 PDFDocument1 pageCYCLONE Drawing v0 PDF43No ratings yet
- Effectof Geometric Parametersonthe Performanceof CycloneDocument6 pagesEffectof Geometric Parametersonthe Performanceof Cyclone43No ratings yet
- Test Certification: Cartridge P/N: TCAL-30 Media Type: 20 X 30 Mesh, 5% TEDA Impregnated Carbon Media Lot #: I-22032Document12 pagesTest Certification: Cartridge P/N: TCAL-30 Media Type: 20 X 30 Mesh, 5% TEDA Impregnated Carbon Media Lot #: I-2203243No ratings yet
- Cylone DesignDocument1 pageCylone Design43No ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- 10 1108 - TQM 03 2020 0066 PDFDocument23 pages10 1108 - TQM 03 2020 0066 PDFLejandra MNo ratings yet
- Toolbox TalkDocument14 pagesToolbox Talkcall_mustafas2361No ratings yet
- CATaclysm Preview ReleaseDocument52 pagesCATaclysm Preview ReleaseGhaderalNo ratings yet
- Python in Hidrology BookDocument153 pagesPython in Hidrology BookJuan david Gonzalez vasquez100% (1)
- Jacob Stewart ResumeDocument2 pagesJacob Stewart Resumeapi-250063152No ratings yet
- Instant Download Business in Action 7Th Edition Bovee Solutions Manual PDF ScribdDocument17 pagesInstant Download Business in Action 7Th Edition Bovee Solutions Manual PDF ScribdLance CorreaNo ratings yet
- Grade 3 - Unit 1 Increase and Decrease PatternDocument7 pagesGrade 3 - Unit 1 Increase and Decrease PatternKyo ToeyNo ratings yet
- Evidence Prove DiscriminationDocument5 pagesEvidence Prove DiscriminationRenzo JimenezNo ratings yet
- G2 Rust Grades USA PDFDocument2 pagesG2 Rust Grades USA PDFSt3fandragos4306No ratings yet
- Sample CVFormat 1Document2 pagesSample CVFormat 1subham.sharmaNo ratings yet
- Test Physics Chapter# 12,13,14 (2 Year) NameDocument1 pageTest Physics Chapter# 12,13,14 (2 Year) NameStay FocusedNo ratings yet
- 2 Design of DOSAGE DESIGNDocument16 pages2 Design of DOSAGE DESIGNMarjo100% (1)
- Common Core Content and Training Objectives For Basic AIS Training - Phase 2 - SpecialistDocument82 pagesCommon Core Content and Training Objectives For Basic AIS Training - Phase 2 - SpecialistjlferreiraNo ratings yet
- Pathogenic Escherichia Coli Associated With DiarrheaDocument7 pagesPathogenic Escherichia Coli Associated With DiarrheaSiti Fatimah RadNo ratings yet
- MH5-C Prospekt PDFDocument16 pagesMH5-C Prospekt PDFvatasaNo ratings yet
- Been There, Done That, Wrote The Blog: The Choices and Challenges of Supporting Adolescents and Young Adults With CancerDocument8 pagesBeen There, Done That, Wrote The Blog: The Choices and Challenges of Supporting Adolescents and Young Adults With CancerNanis DimmitrisNo ratings yet
- Work Breakdown StructureDocument8 pagesWork Breakdown StructurerenshagullNo ratings yet
- Healthy Apps Us New VarDocument9 pagesHealthy Apps Us New VarJESUS DELGADONo ratings yet
- Galgotias University Uttar Pradesh School of Computing Science & Engineering B.Tech. (CSE) 2018-19 Semester Wise Breakup of CoursesDocument2 pagesGalgotias University Uttar Pradesh School of Computing Science & Engineering B.Tech. (CSE) 2018-19 Semester Wise Breakup of CoursesRohit Singh BhatiNo ratings yet
- Pathophysiology of Myocardial Infarction and Acute Management StrategiesDocument11 pagesPathophysiology of Myocardial Infarction and Acute Management StrategiesnwabukingzNo ratings yet
- Conducting Focus GroupsDocument4 pagesConducting Focus GroupsOxfam100% (1)
- KDE11SSDocument2 pagesKDE11SSluisgomezpasion1No ratings yet
- Highlights ASME Guides Preheat PWHT IDocument4 pagesHighlights ASME Guides Preheat PWHT IArul Edwin Vijay VincentNo ratings yet
- Praise and Worship Songs Volume 2 PDFDocument92 pagesPraise and Worship Songs Volume 2 PDFDaniel AnayaNo ratings yet
- Registration ListDocument5 pagesRegistration ListGnanesh Shetty BharathipuraNo ratings yet
- Federalist Papers 10 51 ExcerptsDocument2 pagesFederalist Papers 10 51 Excerptsapi-292351355No ratings yet
- 19 Dark PPT TemplateDocument15 pages19 Dark PPT TemplateKurt W. DelleraNo ratings yet
- RCA LCD26V6SY Service Manual 1.0 PDFDocument33 pagesRCA LCD26V6SY Service Manual 1.0 PDFPocho Pochito100% (1)
- Breastfeeding W Success ManualDocument40 pagesBreastfeeding W Success ManualNova GaveNo ratings yet
- J.K. Brimacombe - Design of Continuous Casting MachinesDocument13 pagesJ.K. Brimacombe - Design of Continuous Casting MachinesJavier GómezNo ratings yet