You might also like
- Car Bop Latin PIDocument19 pagesCar Bop Latin PIdsouzareshminaNo ratings yet
- Standardization of Chemotherapy and Individual Dosing of Platinum CompoundsDocument6 pagesStandardization of Chemotherapy and Individual Dosing of Platinum CompoundsJesse Helmut Hansen-BartelNo ratings yet
- Tyrosine Kinase Inhibittors - Recent Advances: DR Shuvra Neel BaulDocument53 pagesTyrosine Kinase Inhibittors - Recent Advances: DR Shuvra Neel BaulumasinhaNo ratings yet
- Advances in The Management of Non Small Cell Lung CancerDocument53 pagesAdvances in The Management of Non Small Cell Lung CancerRashid AyubiNo ratings yet
- In Vitro: Wu-Chou Su, Shu-Ling Chang, Tsai-Yun Chen, Jiann-Shiuh Chen and Chao-Jung TsaoDocument6 pagesIn Vitro: Wu-Chou Su, Shu-Ling Chang, Tsai-Yun Chen, Jiann-Shiuh Chen and Chao-Jung TsaoJohn GuerreroNo ratings yet
- Cytocrom FuntionDocument24 pagesCytocrom FuntionJorge Ramirez RaherNo ratings yet
- CiplaMed - PACLITAX NAB Injection - 2018-03-20Document21 pagesCiplaMed - PACLITAX NAB Injection - 2018-03-20ravikanthNo ratings yet
- Tyrosine Kinase Inhibitor TKI Flow Chart For Treatment of CMLDocument7 pagesTyrosine Kinase Inhibitor TKI Flow Chart For Treatment of CMLmuthia rana zahra100% (1)
- Right Vs Left CRC Final 1Document47 pagesRight Vs Left CRC Final 1Hemanth KumarNo ratings yet
- 0002-9645-Ajvr 65 11 1502Document6 pages0002-9645-Ajvr 65 11 1502Ioana SanduNo ratings yet
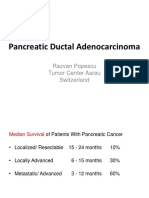
- Europe Balkan Course 2018 Systemic Management of Pancreatic Cancer PopescuDocument64 pagesEurope Balkan Course 2018 Systemic Management of Pancreatic Cancer PopescuCripto MonedeNo ratings yet
- 1121-26 1.10 Kua Voon Fong PDFDocument6 pages1121-26 1.10 Kua Voon Fong PDFfaidgustisyarifNo ratings yet
- Guidelines For Dosing of Some Commonly Used PenicDocument1 pageGuidelines For Dosing of Some Commonly Used PenicRamadan ElkalmiNo ratings yet
- Artículo Leucemia Linfoblástica CrónicaDocument20 pagesArtículo Leucemia Linfoblástica CrónicaMariali PalaciosNo ratings yet
- 12 ON 2020 Lung WBDocument96 pages12 ON 2020 Lung WBabdullahNo ratings yet
- 2028-Article Text-9832-3-10-20131105Document3 pages2028-Article Text-9832-3-10-20131105HMC ProcurementNo ratings yet
- Efikasi Dan Toksisitas Rejimen Sisplatin + Etoposid Untuk Kemoterapi Kanker Paru Jenis Karsinoma Bukan Sel Kecil (KPKBSK) Stage LanjutDocument11 pagesEfikasi Dan Toksisitas Rejimen Sisplatin + Etoposid Untuk Kemoterapi Kanker Paru Jenis Karsinoma Bukan Sel Kecil (KPKBSK) Stage LanjutDila Putri KristiyantiNo ratings yet
- Sangviroon 2010Document8 pagesSangviroon 2010uciNo ratings yet
- Manuscript FiksDocument7 pagesManuscript Fiksninik_suprayitnoNo ratings yet
- Carboplatin Dosing 2nd Draft DrLinkDocument4 pagesCarboplatin Dosing 2nd Draft DrLinkJesse Helmut Hansen-BartelNo ratings yet
- GPT2 - Gls1 - Sensitivity - 2020Document12 pagesGPT2 - Gls1 - Sensitivity - 2020shravanvvNo ratings yet
- Long-Term Mortality After The Blood Pressure and Lipid-Lowering Treatment in Hypertensive Patients: 16-Year Follow-Up of The ASCOT Legacy StudyDocument22 pagesLong-Term Mortality After The Blood Pressure and Lipid-Lowering Treatment in Hypertensive Patients: 16-Year Follow-Up of The ASCOT Legacy StudyFlore HountondjiNo ratings yet
- CML EsmoDocument3 pagesCML EsmowidweedNo ratings yet
- Cancer Lung Chemotherapy Regimen 3.4 March 2015Document69 pagesCancer Lung Chemotherapy Regimen 3.4 March 2015Jenny MárquezNo ratings yet
- Phase I Studies With Carboplatin at The Royal Marsden HospitalDocument7 pagesPhase I Studies With Carboplatin at The Royal Marsden HospitalArun GargNo ratings yet
- Navsari Agricultural University: Reprint Author E-Mail Author(s) Keyword(s) Author Address SourceDocument4 pagesNavsari Agricultural University: Reprint Author E-Mail Author(s) Keyword(s) Author Address Sourcerickpatel373No ratings yet
- Ukrainian Anti-Cancer Institute2Document44 pagesUkrainian Anti-Cancer Institute2Anonymous KUimpSvdNo ratings yet
- Thrombolytics: Interventional FellowDocument51 pagesThrombolytics: Interventional Fellowusfcards100% (1)
- Dasatinib vs. Imatinib in Patients With Chronic Myeloid Leukemia in Chronic Phase (CML-CP)Document10 pagesDasatinib vs. Imatinib in Patients With Chronic Myeloid Leukemia in Chronic Phase (CML-CP)risna sariNo ratings yet
- Hodgkin LymphomaDocument32 pagesHodgkin LymphomaAndi SusiloNo ratings yet
- Producing Kpc-Type Carbapenemases Mediated by Insertional Inactivation of The Phoq/Phop MGRB RegulatorDocument6 pagesProducing Kpc-Type Carbapenemases Mediated by Insertional Inactivation of The Phoq/Phop MGRB RegulatorABachiraya MongkhunNo ratings yet
- M. Sibuea, M. Lutfi, M. HakimiDocument9 pagesM. Sibuea, M. Lutfi, M. HakimiVeronica SharinoNo ratings yet
- Agonist-Inverse Agonist Characterization at CB1 and CB2Document8 pagesAgonist-Inverse Agonist Characterization at CB1 and CB2Maria DanilaNo ratings yet
- j.1528-1167.2006.00715 30.xDocument272 pagesj.1528-1167.2006.00715 30.xJeremy PorteousNo ratings yet
- Cancer de Plaman Cu Celule MiciDocument84 pagesCancer de Plaman Cu Celule MiciANDREEA GRIGORASNo ratings yet
- ASH CaplacizumabDocument4 pagesASH CaplacizumabMagdalena Górska-KosickaNo ratings yet
- Alvarado Lahip2Document11 pagesAlvarado Lahip2api-559892740No ratings yet
- S 025 LBLDocument16 pagesS 025 LBLarmanNo ratings yet
- Formulation and Evaluation of Dsatinib TabletsDocument9 pagesFormulation and Evaluation of Dsatinib TabletsSyed Abdul Haleem AkmalNo ratings yet
- CNR2 4 E1310Document7 pagesCNR2 4 E1310فرجني موغNo ratings yet
- 2018 CML Updates and Case Presentations: Washington University in ST Louis Medical SchoolDocument113 pages2018 CML Updates and Case Presentations: Washington University in ST Louis Medical SchoolIris GzlzNo ratings yet
- Pharmacology of OxaliplatinDocument16 pagesPharmacology of OxaliplatinAliza JafriNo ratings yet
- Methven TPCR RDocument6 pagesMethven TPCR RMARIA VICTORIA VELARDE ALIAGANo ratings yet
- 81572-Article Text-197102-1-10-20170330Document10 pages81572-Article Text-197102-1-10-20170330Lydie Praxede EkoboNo ratings yet
- BJC 2013230Document6 pagesBJC 2013230Abraham OsunaNo ratings yet
- FPTP - Amoxicillin - Clavulanic Acid in Cats With & Without Chronic Kidney DiseaseDocument2 pagesFPTP - Amoxicillin - Clavulanic Acid in Cats With & Without Chronic Kidney DiseaseMabe AguirreNo ratings yet
- A Systematic Review and Economic Model of The Clinical and Cost-Effectiveness of Immunosuppressive Therapy For Renal Transplantation in ChildrenDocument6 pagesA Systematic Review and Economic Model of The Clinical and Cost-Effectiveness of Immunosuppressive Therapy For Renal Transplantation in Childrenjose.ottoNo ratings yet
- Crej2: Alkaline PHDocument7 pagesCrej2: Alkaline PHMadalina Cioroiu-AndronescuNo ratings yet
- Savremena Inzulinska TerapijaDocument35 pagesSavremena Inzulinska TerapijaAmilaHadžićNo ratings yet
- Experience of Starting ABO Incompatible Renal Transplant in NepalDocument4 pagesExperience of Starting ABO Incompatible Renal Transplant in NepalRabin NepaliNo ratings yet
- Elecsys Calcitinin Fact SheetDocument2 pagesElecsys Calcitinin Fact SheetNika AndrianiNo ratings yet
- A Theoretical Physiologically-Based Pharmacokinetic Approach To Ascertain Covariates Explaining The Large Interpatient Variability in Tacrolimus DispositionDocument12 pagesA Theoretical Physiologically-Based Pharmacokinetic Approach To Ascertain Covariates Explaining The Large Interpatient Variability in Tacrolimus Disposition陈梓强No ratings yet
- Clozapina 3Document16 pagesClozapina 3Robert MovileanuNo ratings yet
- Daivonex Cream PI - LPS-11-045Document5 pagesDaivonex Cream PI - LPS-11-045Hesam AhmadianNo ratings yet
- Appendix 5 Calculation of Estimated Creatinine Clearance (CRCL)Document4 pagesAppendix 5 Calculation of Estimated Creatinine Clearance (CRCL)Erin FlowersNo ratings yet
- 311 Topotecan Monotherapy 5 DayDocument4 pages311 Topotecan Monotherapy 5 DayRuxandra BănicăNo ratings yet
- Sonnykalangi,+65 +ok+rev+SUMARDIANI+08529863978Document7 pagesSonnykalangi,+65 +ok+rev+SUMARDIANI+08529863978djibriel92No ratings yet
- Fast Facts: Treatment-Free Remission in Chronic Myeloid Leukemia: From concept to practice and beyondFrom EverandFast Facts: Treatment-Free Remission in Chronic Myeloid Leukemia: From concept to practice and beyondNo ratings yet
- ChoreaDocument4 pagesChoreaapi-19973386No ratings yet
- Icra Longterms CareDocument19 pagesIcra Longterms CareFajarRachmadiNo ratings yet
- Untitled PresentationDocument228 pagesUntitled PresentationSafira WasimNo ratings yet
- Astigmidwife Vlogs Online Tutorial: All Rights Are Reserved. No Part of This Publication May Be ReproducedDocument12 pagesAstigmidwife Vlogs Online Tutorial: All Rights Are Reserved. No Part of This Publication May Be ReproducedLynden BulanNo ratings yet
- Brooder PneumoniaDocument27 pagesBrooder PneumoniaMohammad Rizwan SaeedNo ratings yet
- Hypoglycemia in Adults Clinical Manifestations, Definition, and CausesDocument1 pageHypoglycemia in Adults Clinical Manifestations, Definition, and CausesnovaNo ratings yet
- Progeria Case StudyDocument12 pagesProgeria Case StudyChristein Roger Dondoyano GamaleNo ratings yet
- Tuberculosis 2022Document17 pagesTuberculosis 2022Mohamed HamzaNo ratings yet
- Immunization ScheduleDocument2 pagesImmunization ScheduleTracy100% (1)
- Fatigue After StrokeDocument6 pagesFatigue After StrokeAnugerah NasutionNo ratings yet
- Gambaran Klinis Dan Patologis Pada Ayam Yang Terserang Flu Burung Sangat Patogenik (HPAI) Di Beberapa Peternakan Di Jawa Timur Dan Jawa BaratDocument9 pagesGambaran Klinis Dan Patologis Pada Ayam Yang Terserang Flu Burung Sangat Patogenik (HPAI) Di Beberapa Peternakan Di Jawa Timur Dan Jawa BaratILHAM BAGUS DARMA .NNo ratings yet
- Chapter 4: Comprehensive Geriatric Assessment: Multiple ChoiceDocument3 pagesChapter 4: Comprehensive Geriatric Assessment: Multiple ChoiceJamie100% (2)
- Cervical DystociaDocument22 pagesCervical DystociaBaldau TiwariNo ratings yet
- Thyroid Function Blood TestsDocument5 pagesThyroid Function Blood TestsCassandra ColigadoNo ratings yet
- Revathi Papsmear ProcedureDocument50 pagesRevathi Papsmear ProcedureRevathi DadamNo ratings yet
- Health Certificate PDFDocument2 pagesHealth Certificate PDFPedro KunstNo ratings yet
- 53 Coronary Artery AnomaliesDocument5 pages53 Coronary Artery AnomaliesVictor PazNo ratings yet
- Time in Time Out: Temperature Monitoring Log Sheet For The Month of February 2019Document6 pagesTime in Time Out: Temperature Monitoring Log Sheet For The Month of February 2019Waqas VickyNo ratings yet
- 327-Differential Diagnosis of SEIZURE - SattawutDocument44 pages327-Differential Diagnosis of SEIZURE - Sattawutyusma wati99No ratings yet
- Drugs Affecting Coagulation ObjectivesDocument14 pagesDrugs Affecting Coagulation ObjectiveslouradelNo ratings yet
- Obstetrics & Gynecologyc MnemonicsDocument12 pagesObstetrics & Gynecologyc MnemonicsMuhammad Luqman Nul HakimNo ratings yet
- Rubifen 10 MG Immediate Release TabletsDocument8 pagesRubifen 10 MG Immediate Release TabletsMuse LoverNo ratings yet
- A A To Raco AbdominalDocument64 pagesA A To Raco AbdominalYgor AlbuquerqueNo ratings yet
- Leech TherapyDocument30 pagesLeech TherapyMohamed ShiffaNo ratings yet
- Healing-Chakras (GLB)Document21 pagesHealing-Chakras (GLB)GetaLuciaNo ratings yet
- Fistula Ani Japanese GuidelineDocument7 pagesFistula Ani Japanese GuidelinevivianmtNo ratings yet
- New Inborn Error of MetabolismDocument45 pagesNew Inborn Error of Metabolismmannan mangal100% (1)
- CH 084 Oral ThrushDocument7 pagesCH 084 Oral ThrushSavir GuptaNo ratings yet
- Encefalitis LimbicaDocument11 pagesEncefalitis LimbicaRandy UlloaNo ratings yet
- AceDocument14 pagesAceJustice Ace DaprozaNo ratings yet