You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- 2020 Noelle, Brittany - Weight Training For Women - Exercises and Workout Programs For Building Strength With Free Weights-Rockridge Press (2020)Document200 pages2020 Noelle, Brittany - Weight Training For Women - Exercises and Workout Programs For Building Strength With Free Weights-Rockridge Press (2020)Luis Vargas100% (3)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (842)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5807)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Total Gym Work OutDocument16 pagesTotal Gym Work OutBilla Uppalapati100% (1)
- Anabolic Vs Androgenic Ratio of SteroidsDocument2 pagesAnabolic Vs Androgenic Ratio of Steroidsvetmode100% (2)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Dumbbell HIIT Workout Plan PDFDocument5 pagesDumbbell HIIT Workout Plan PDFAlexandra BascoNo ratings yet
- The Ultimate Boxing Workout PlanDocument9 pagesThe Ultimate Boxing Workout PlanJason CarterNo ratings yet
- Training The Lats For Maximum Isolation Stimulation Innervation and Pump by Greg Zulak PDFDocument155 pagesTraining The Lats For Maximum Isolation Stimulation Innervation and Pump by Greg Zulak PDFsech284854100% (7)
- The Tools You Need To Build The Body You Want: Tut Workout: 4 Day Muscle Building Workout SplitDocument1 pageThe Tools You Need To Build The Body You Want: Tut Workout: 4 Day Muscle Building Workout SplitJorge NogalesNo ratings yet
- 30 Days Without Weights For Ultimate StrengthDocument9 pages30 Days Without Weights For Ultimate Strengthmarin0410No ratings yet
- Strengthtraining 1Document26 pagesStrengthtraining 1craig1014100% (5)
- Kettlebell OriginsDocument19 pagesKettlebell Originsthzone1986No ratings yet
- Basketball Advanced Off-Season Strength Training - 1458857274827 PDFDocument18 pagesBasketball Advanced Off-Season Strength Training - 1458857274827 PDFwarrenbuirchNo ratings yet
- NZ Rugby WorkoutDocument6 pagesNZ Rugby Workoutjmhiggin9894No ratings yet
- Ross Dickerson - WEIGHTED AND CARDIO ABS 2018 PDFDocument13 pagesRoss Dickerson - WEIGHTED AND CARDIO ABS 2018 PDFKartik Singh50% (2)
- QBANKDocument38 pagesQBANKsbarolia2673% (11)
- Beast Ebook PDFDocument38 pagesBeast Ebook PDFSteeN100% (1)
- Klokov Training ProgramDocument3 pagesKlokov Training ProgramHari SetiawanNo ratings yet
- Northwestern University, Inc: After Finishing The Course, The Student Must Be Able To: and of The CTEDocument7 pagesNorthwestern University, Inc: After Finishing The Course, The Student Must Be Able To: and of The CTENicole ReidNo ratings yet
- Module Dual SPorts PrelimsDocument62 pagesModule Dual SPorts PrelimsNicole ReidNo ratings yet
- Additional Patient PopulationsDocument4 pagesAdditional Patient PopulationsNicole ReidNo ratings yet
- Endurance, Resistance and Flexibility ExerciseDocument6 pagesEndurance, Resistance and Flexibility ExerciseNicole ReidNo ratings yet
- Physiologic Aspects and Medical EvaluationDocument2 pagesPhysiologic Aspects and Medical EvaluationNicole ReidNo ratings yet
- Active Assisted and Passive ROM ExercisesDocument6 pagesActive Assisted and Passive ROM ExercisesNicole ReidNo ratings yet
- Libro1 (Versión 1) (Autoguardado)Document12 pagesLibro1 (Versión 1) (Autoguardado)Maria SantiagoNo ratings yet
- Funda ExamDocument21 pagesFunda ExamFebykates Egos-RafisuraNo ratings yet
- Weight Training Technique Part204Document1 pageWeight Training Technique Part204larvitar2No ratings yet
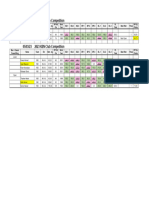
- Results - KZN Club Comp March 2023Document1 pageResults - KZN Club Comp March 2023Kiran KooverjeeNo ratings yet
- Spectrum Exercises PDFDocument54 pagesSpectrum Exercises PDFbog495100% (1)
- Week 8 AssignmentDocument9 pagesWeek 8 Assignmentapi-521054554No ratings yet
- Weight Training For The Martial Artist Martial Arts Self DefenseDocument116 pagesWeight Training For The Martial Artist Martial Arts Self DefenseKalyan PingaliNo ratings yet
- GZCLP 3 Day TemplateDocument15 pagesGZCLP 3 Day TemplatepkojivqlNo ratings yet
- Name:Mustafa Reg No.12397 Subject:Therapeutic ExerciseDocument10 pagesName:Mustafa Reg No.12397 Subject:Therapeutic Exercisemustafa wazirNo ratings yet
- Nrol Blank Training Log For LifeDocument6 pagesNrol Blank Training Log For LifeejnNo ratings yet
- Crec Colts HandbookDocument19 pagesCrec Colts Handbookapi-280048754No ratings yet
- ACEBarcelona2017 Results 1day 1Document13 pagesACEBarcelona2017 Results 1day 1xosmar185No ratings yet
- 3 - Day - Male - Final - 1 - OGDocument5 pages3 - Day - Male - Final - 1 - OGuser240No ratings yet
- Pyramid Weight Lifting ChartDocument3 pagesPyramid Weight Lifting ChartJoshua WhiteNo ratings yet