You might also like
- Assessment, Controversy, and Confounding Factors: Brain DeathDocument23 pagesAssessment, Controversy, and Confounding Factors: Brain DeathdewiNo ratings yet
- Cerebral Herniation Syndromes and Intracranial HypertensionFrom EverandCerebral Herniation Syndromes and Intracranial HypertensionMatthew KoenigNo ratings yet
- DAO 2000-98 Safety RulesDocument118 pagesDAO 2000-98 Safety RulesKaring Paalan Paredes67% (3)
- Dapus 32Document4 pagesDapus 32Titi SulistiowatiNo ratings yet
- Neutrophil To Lymphocyte Ratio at Admission Prognostic Factor in Patients With Acute Ischemic StrokeDocument7 pagesNeutrophil To Lymphocyte Ratio at Admission Prognostic Factor in Patients With Acute Ischemic StrokeUtari UbNo ratings yet
- Manejo PostparoDocument17 pagesManejo PostparoAngela Moreira ArteagaNo ratings yet
- Management of Intracranial Pressure: Part I: ClinicalDocument10 pagesManagement of Intracranial Pressure: Part I: ClinicaljuanNo ratings yet
- Fisiopatoliga Evc Imagen PDFDocument13 pagesFisiopatoliga Evc Imagen PDFOswaldo AmayaNo ratings yet
- Acute Ischemic StrokeDocument9 pagesAcute Ischemic Strokepuskesmas tarikNo ratings yet
- Posterior Reversible Encephalopathy Syndrome: A Review: Jai Shankar, DM, MSC, Jillian Banfield, PHDDocument7 pagesPosterior Reversible Encephalopathy Syndrome: A Review: Jai Shankar, DM, MSC, Jillian Banfield, PHDkidNo ratings yet
- A Study On Fasting Lipid Profile in Nonadiabetic Stroke PatientsDocument8 pagesA Study On Fasting Lipid Profile in Nonadiabetic Stroke PatientsIJAR JOURNALNo ratings yet
- Research On Post Reversible Encephalopathy Due To Blood TransfusionsDocument7 pagesResearch On Post Reversible Encephalopathy Due To Blood TransfusionsAnkit AgarwalNo ratings yet
- Bruce C V Campbell Ischaemic Stroke 2019Document22 pagesBruce C V Campbell Ischaemic Stroke 2019yiyecNo ratings yet
- 1092 0684 Article Pe7Document8 pages1092 0684 Article Pe7ersalivianiNo ratings yet
- Lo SatuDocument5 pagesLo SatuRatihNo ratings yet
- A Study On Fasting Lipid Profile in Non-Diabetic Stroke PatientsDocument7 pagesA Study On Fasting Lipid Profile in Non-Diabetic Stroke PatientsIJAR JOURNALNo ratings yet
- Cerebral Hyperperfusion Syndrome After Carotid Revascularization: A Brief ReviewDocument7 pagesCerebral Hyperperfusion Syndrome After Carotid Revascularization: A Brief ReviewanankastikNo ratings yet
- Tadevosyan 2021Document26 pagesTadevosyan 2021W Antonio Rivera MartínezNo ratings yet
- 3 Principles of Intracranial PressureDocument21 pages3 Principles of Intracranial Pressureba.ramirez11No ratings yet
- 1 s2.0 S1878875018317406 PDFDocument10 pages1 s2.0 S1878875018317406 PDFeribu191No ratings yet
- Neonates With Symptomatic Hyperinsulinemic Hypoglycemia Generate Inappropriately Low Serum Cortisol Countrregulatory Hormonal Responses 2003Document6 pagesNeonates With Symptomatic Hyperinsulinemic Hypoglycemia Generate Inappropriately Low Serum Cortisol Countrregulatory Hormonal Responses 2003Arturo RNo ratings yet
- Blood Pressure and The Brain The Neurology of Hypertension PDFDocument12 pagesBlood Pressure and The Brain The Neurology of Hypertension PDFGustavo PestanaNo ratings yet
- Strokeaha 119 025061Document7 pagesStrokeaha 119 025061Jess RitumaltaNo ratings yet
- Recurrent Primary Cerebral Hemorrhage: Frequency, Mechanisms, and PrognosisDocument4 pagesRecurrent Primary Cerebral Hemorrhage: Frequency, Mechanisms, and PrognosismelvinNo ratings yet
- Haemorrhagic Stroke On Elderly Man With Uncontrolled HypertensionDocument7 pagesHaemorrhagic Stroke On Elderly Man With Uncontrolled HypertensionRifka IrhamnaNo ratings yet
- Posterior Reversible Encephalopathy SyndromeDocument9 pagesPosterior Reversible Encephalopathy SyndromejuanmontoyaseNo ratings yet
- HIE and CVSDocument11 pagesHIE and CVSakshayajainaNo ratings yet
- Cortical Hyperintensity On Proton Density-Weighted Images: An MR Sign of Cyclosporine-Related EncephalopathyDocument9 pagesCortical Hyperintensity On Proton Density-Weighted Images: An MR Sign of Cyclosporine-Related Encephalopathyshannon prijadiNo ratings yet
- Abnormal Regional Cerebral Blood Flow in Cognitively Normal Elderly Subjects With HypertensionDocument7 pagesAbnormal Regional Cerebral Blood Flow in Cognitively Normal Elderly Subjects With HypertensionAminarsihNo ratings yet
- 2017 Motor CortexDocument5 pages2017 Motor Cortexramy RamyNo ratings yet
- Stroke Volume Predicts Nocturnal Hypoxemia in The Acute Ischemic Stroke After Intravenous ThrombolysisDocument8 pagesStroke Volume Predicts Nocturnal Hypoxemia in The Acute Ischemic Stroke After Intravenous ThrombolysisPutri Rahmadhani Ngakpaniklage AsdsNo ratings yet
- Hypertension AsessmentDocument20 pagesHypertension AsessmentLale Aulia M WidarmiNo ratings yet
- Neuro4Nurses Cerebellar StrokeDocument2 pagesNeuro4Nurses Cerebellar StrokeAisyahNurjannahNo ratings yet
- Levitt2019 PDFDocument14 pagesLevitt2019 PDFalejandro echeverriNo ratings yet
- Perioperative Glucocorticoid ManagementDocument8 pagesPerioperative Glucocorticoid ManagementjuanpbagurNo ratings yet
- Intracranialhemorrhage Andintracranial Hypertension: Evie Marcolini,, Christoph Stretz,, Kyle M. DewittDocument16 pagesIntracranialhemorrhage Andintracranial Hypertension: Evie Marcolini,, Christoph Stretz,, Kyle M. DewittAxel DuncanNo ratings yet
- Basic Principles of Cerebral Protection in Humans: William L. LanierDocument4 pagesBasic Principles of Cerebral Protection in Humans: William L. Lanierrachel0301No ratings yet
- Aldosterone Does Not Predict Cardiovascular Events Following Acute Coronary Syndrome in Patients Initially Without Heart FailureDocument8 pagesAldosterone Does Not Predict Cardiovascular Events Following Acute Coronary Syndrome in Patients Initially Without Heart FailureAbdulkafi tashaniNo ratings yet
- Article 4 NL RatioDocument4 pagesArticle 4 NL RatioPrateek Kumar PandaNo ratings yet
- 2020 Can Ocular OCT Findings Be As A Predictor For End-Organ Damage in Systemic Hypertension?Document5 pages2020 Can Ocular OCT Findings Be As A Predictor For End-Organ Damage in Systemic Hypertension?StefanieNo ratings yet
- Cyclic Cushing 'S Syndrome - A Diagnostic ChallengeDocument7 pagesCyclic Cushing 'S Syndrome - A Diagnostic ChallengeAndri AffandiNo ratings yet
- Intracraneanal PressureDocument8 pagesIntracraneanal PressurearturoNo ratings yet
- A Case Report of Posterior Reversible Encephalopathy Syndrome in A Patient Diagnosed With Emphysematous Necrotizing Biliary PancreatitisDocument5 pagesA Case Report of Posterior Reversible Encephalopathy Syndrome in A Patient Diagnosed With Emphysematous Necrotizing Biliary Pancreatitisbijnn journalNo ratings yet
- The Human Sympathetic Nervous System: Its Relevance in Hypertension and Heart FailureDocument10 pagesThe Human Sympathetic Nervous System: Its Relevance in Hypertension and Heart FailureadeNo ratings yet
- Common Etiologies of Upper Extremity SpasticityDocument7 pagesCommon Etiologies of Upper Extremity SpasticityNoviNo ratings yet
- 9 CNS Sequela of CHDDocument9 pages9 CNS Sequela of CHDVictor PazNo ratings yet
- Cerebral Salt Wasting Is The Most Common Cause of Hyponatremia in StrokeDocument7 pagesCerebral Salt Wasting Is The Most Common Cause of Hyponatremia in StrokeAlkausarNo ratings yet
- Cushing Syndrome 2Document16 pagesCushing Syndrome 2ClarestaNo ratings yet
- Acute Ischemic Stroke: Clinical PracticeDocument8 pagesAcute Ischemic Stroke: Clinical PracticeDorina FrunzeNo ratings yet
- Textbook of NeuroimagingDocument403 pagesTextbook of NeuroimagingcelooshNo ratings yet
- Jurnal 12Document10 pagesJurnal 12Zella ZakyaNo ratings yet
- Electrolytes Disturbances and Seizures: Critical ReviewDocument9 pagesElectrolytes Disturbances and Seizures: Critical ReviewkomalkomelNo ratings yet
- Evaluation and Management of Elevated Intracranial Pressure in AdultsDocument28 pagesEvaluation and Management of Elevated Intracranial Pressure in AdultssandykumalaNo ratings yet
- Acute CardiacDocument23 pagesAcute CardiacbagusputrabaliNo ratings yet
- T T A S: Hrombolytic Herapy in Cute TrokeDocument3 pagesT T A S: Hrombolytic Herapy in Cute TrokevivinNo ratings yet
- Block 2 Assignment Edited Catherine Ruguru SamsonDocument12 pagesBlock 2 Assignment Edited Catherine Ruguru Samsonmoses karituNo ratings yet
- Fisiopatología EstatusDocument14 pagesFisiopatología EstatusDaniel LeivaNo ratings yet
- Garosi 2011Document9 pagesGarosi 2011Alba Rocio Zavala MoyaNo ratings yet
- 10.1038@s41572 019 0118 8Document22 pages10.1038@s41572 019 0118 8Anabel AguilarNo ratings yet
- Orthostatic Hypotension in Older AdultsFrom EverandOrthostatic Hypotension in Older AdultsAhmet Turan IsikNo ratings yet
- The Dislocated Brain: Innovation in Traumatic Brain Injury and IrrigationFrom EverandThe Dislocated Brain: Innovation in Traumatic Brain Injury and IrrigationRating: 5 out of 5 stars5/5 (2)
- Marinedrugs 15 00295Document16 pagesMarinedrugs 15 00295Jean Pierre Chastre LuzaNo ratings yet
- IGTANJINSDocument8 pagesIGTANJINSJean Pierre Chastre LuzaNo ratings yet
- A New A-Conotoxin Which Targets A3b2 Nicotinic AceDocument8 pagesA New A-Conotoxin Which Targets A3b2 Nicotinic AceJean Pierre Chastre LuzaNo ratings yet
- Glutamate: The Most Abundant Neurotransmitter: Bernat González I LlinaresDocument35 pagesGlutamate: The Most Abundant Neurotransmitter: Bernat González I LlinaresJean Pierre Chastre LuzaNo ratings yet
- Brainstem: Francisco E. Olucha BordonauDocument22 pagesBrainstem: Francisco E. Olucha BordonauJean Pierre Chastre LuzaNo ratings yet
- Somatosensory PathwaysDocument28 pagesSomatosensory PathwaysJean Pierre Chastre LuzaNo ratings yet
- Development of The NSDocument7 pagesDevelopment of The NSJean Pierre Chastre LuzaNo ratings yet
- Baba & Ji (MCN, 2003)Document13 pagesBaba & Ji (MCN, 2003)Jean Pierre Chastre LuzaNo ratings yet
- Cerebellum TextDocument7 pagesCerebellum TextJean Pierre Chastre LuzaNo ratings yet
- Dendritic Reorganization in Pyramidal Neurons in Medial Prefrontal Cortex After Chronic Corticosterone AdministrationDocument9 pagesDendritic Reorganization in Pyramidal Neurons in Medial Prefrontal Cortex After Chronic Corticosterone AdministrationJean Pierre Chastre LuzaNo ratings yet
- BDNFand ECSDocument6 pagesBDNFand ECSJean Pierre Chastre LuzaNo ratings yet
- 83 1yhhhDocument6 pages83 1yhhhJean Pierre Chastre LuzaNo ratings yet
- Antidepressant Effect of Extracts From Ginkgo Biloba Leaves in Behavioral ModelsDocument4 pagesAntidepressant Effect of Extracts From Ginkgo Biloba Leaves in Behavioral ModelsJean Pierre Chastre LuzaNo ratings yet
- Uva-Dare (Digital Academic Repository)Document37 pagesUva-Dare (Digital Academic Repository)Jean Pierre Chastre LuzaNo ratings yet
- Reseach and Report Yokukansan Increases Serum Brain-Derived Neurotrophic Factor (BDNF) Levels in Gunn RatDocument8 pagesReseach and Report Yokukansan Increases Serum Brain-Derived Neurotrophic Factor (BDNF) Levels in Gunn RatJean Pierre Chastre LuzaNo ratings yet
- Perifusion Steroidogenesis Leydig: LH-dependentDocument9 pagesPerifusion Steroidogenesis Leydig: LH-dependentJean Pierre Chastre LuzaNo ratings yet
- 10 1 1 375 5716Document7 pages10 1 1 375 5716Jean Pierre Chastre LuzaNo ratings yet
- Auer1984 Article TheDistributionOfHypoglycemicBDocument15 pagesAuer1984 Article TheDistributionOfHypoglycemicBJean Pierre Chastre LuzaNo ratings yet
- Mæhlen-Torvik1990 Article NecrosisOfGranuleCellsOfHippocDocument3 pagesMæhlen-Torvik1990 Article NecrosisOfGranuleCellsOfHippocJean Pierre Chastre LuzaNo ratings yet
- Regulation by Prostaglandins Steroidogenesis Large: Differential of ofDocument9 pagesRegulation by Prostaglandins Steroidogenesis Large: Differential of ofJean Pierre Chastre LuzaNo ratings yet
- Steroidogenesis by Development: StagesDocument8 pagesSteroidogenesis by Development: StagesJean Pierre Chastre LuzaNo ratings yet
- Alpha7 Nicotinic Acetylcholine Receptor Is A Target in Pharmacology and ToxicologyDocument20 pagesAlpha7 Nicotinic Acetylcholine Receptor Is A Target in Pharmacology and ToxicologyJean Pierre Chastre LuzaNo ratings yet
- De Jong Hey 1973Document8 pagesDe Jong Hey 1973Jean Pierre Chastre LuzaNo ratings yet
- Human A4b2 Neuronal Nicotinic Acetylcholine ReceptDocument13 pagesHuman A4b2 Neuronal Nicotinic Acetylcholine ReceptJean Pierre Chastre LuzaNo ratings yet
- Marine Drugs: The Nemertine Toxin Anabaseine and Its Derivative DMXBA (GTS-21) : Chemical and Pharmacological PropertiesDocument19 pagesMarine Drugs: The Nemertine Toxin Anabaseine and Its Derivative DMXBA (GTS-21) : Chemical and Pharmacological PropertiesJean Pierre Chastre LuzaNo ratings yet
- SHE Meeting PresentationDocument14 pagesSHE Meeting PresentationDanielson CulanibanNo ratings yet
- Chapter 9 - Drug Therapy During PregnancyDocument3 pagesChapter 9 - Drug Therapy During Pregnancydlneisha61No ratings yet
- Case StudyDocument13 pagesCase StudySanthiya MogenNo ratings yet
- DSM 5 Pros and ConsDocument6 pagesDSM 5 Pros and Consapi-484975841No ratings yet
- Louisiana SDM Screening and Response Assessment 10-17-2011Document22 pagesLouisiana SDM Screening and Response Assessment 10-17-2011Rick ThomaNo ratings yet
- Foundations, Promises and Uncertainties of Personalized MedicineDocument7 pagesFoundations, Promises and Uncertainties of Personalized MedicineVeronica BalanNo ratings yet
- Differential Diagnosis of Neck MassesDocument10 pagesDifferential Diagnosis of Neck Massesapi-19916399No ratings yet
- Assestment 5 SUPERVISOR REPORT TemplateDocument3 pagesAssestment 5 SUPERVISOR REPORT TemplateOhms Branguelo100% (1)
- Report Using The American Conference of Industrial HygienDocument46 pagesReport Using The American Conference of Industrial Hygienjuscel1n0No ratings yet
- Covid 19 ReportDocument4 pagesCovid 19 ReportJeancy SenosinNo ratings yet
- Introduction From Nancy Lonsdorf M.D.: Maharishi Vedic MedicineDocument81 pagesIntroduction From Nancy Lonsdorf M.D.: Maharishi Vedic Medicines muraNo ratings yet
- Clinical Practice Guidelines For Pain Management.11Document25 pagesClinical Practice Guidelines For Pain Management.11Neta Aza MaineztNo ratings yet
- Building Renovation How To Retrofit and Reuse Existing Buildings To Save Energy and Respond To New Needs (Manuela Grecchi)Document127 pagesBuilding Renovation How To Retrofit and Reuse Existing Buildings To Save Energy and Respond To New Needs (Manuela Grecchi)zainab abbas100% (1)
- Electronic Child Health Network (Echn) : Hospitals in OntarioDocument7 pagesElectronic Child Health Network (Echn) : Hospitals in OntariobevNo ratings yet
- What Is Dengue FeverDocument28 pagesWhat Is Dengue FeverNatalieNo ratings yet
- Hyperlipidemia 1Document32 pagesHyperlipidemia 1Binita ShakyaNo ratings yet
- Thermal Baths GermanyDocument92 pagesThermal Baths Germanyvikaspi100% (1)
- Adolescent Health Care PDFDocument729 pagesAdolescent Health Care PDFAlain BriseñoNo ratings yet
- The Political Economy Of Robots Prospects For Prosperity And Peace In The Automated 21St Century Ryan Kiggins Ed full chapter pdf docxDocument70 pagesThe Political Economy Of Robots Prospects For Prosperity And Peace In The Automated 21St Century Ryan Kiggins Ed full chapter pdf docxsialiorewa100% (2)
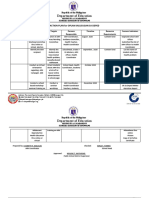
- Sta. Anastacia-San Rafael National High School ARH Action Plan For 2019Document4 pagesSta. Anastacia-San Rafael National High School ARH Action Plan For 2019LylebethMalolesNo ratings yet
- Procedural Sedation in The ED: - Myths and MethodsDocument37 pagesProcedural Sedation in The ED: - Myths and MethodsSteven RossNo ratings yet
- SAT 5th EditionDocument234 pagesSAT 5th EditionChandrasreeNo ratings yet
- Tujuan Teori KeperawatanDocument15 pagesTujuan Teori KeperawatankintaniaNo ratings yet
- Bulgarian Diet - Lose Weight Diets 2013Document3 pagesBulgarian Diet - Lose Weight Diets 2013Curin Ioan AurelianNo ratings yet
- PhenobarbitalDocument2 pagesPhenobarbitalArnzz Agbulos100% (1)
- Tom's Fourth Year Guide (2011-12)Document709 pagesTom's Fourth Year Guide (2011-12)jangyNo ratings yet
- THERA DWI K. (202010230311349/G) : Read The Text Carefully and Answer The QuestionsDocument2 pagesTHERA DWI K. (202010230311349/G) : Read The Text Carefully and Answer The Questionsthera dwiNo ratings yet
- Learning Module in PE Grade 11: Quarter 1 (Week 4)Document9 pagesLearning Module in PE Grade 11: Quarter 1 (Week 4)emerito basillaNo ratings yet
- DIASS Module 4 3rd Q OkDocument12 pagesDIASS Module 4 3rd Q OkLady PilaNo ratings yet