You might also like
- USMLE Step 1 NBME Question Review: Rahul Damania, MD, FAAPDocument50 pagesUSMLE Step 1 NBME Question Review: Rahul Damania, MD, FAAPRubayet Tasfin AlifNo ratings yet
- Cervicogenic HeadacheDocument8 pagesCervicogenic HeadacheEmma KopcikasNo ratings yet
- HypospadiasDocument41 pagesHypospadiasValerie SyNo ratings yet
- Case Study Endometrial PDFDocument17 pagesCase Study Endometrial PDFapi-279886264No ratings yet
- Annotated Ultra BTR Short 22-4-23 FMT, Derma, Anaesthesia, OrthoDocument27 pagesAnnotated Ultra BTR Short 22-4-23 FMT, Derma, Anaesthesia, OrthoAshok DaukiyaNo ratings yet
- The Role of Diffusion-Weighted Magnetic Resonance Imaging in The Differentiation of Head and Neck MassesDocument10 pagesThe Role of Diffusion-Weighted Magnetic Resonance Imaging in The Differentiation of Head and Neck MassestaufikolingNo ratings yet
- Comparison of Susceptibility Artifact On Rectal Dwi Mri and Rectal Volume Before and After Ultraso PDFDocument6 pagesComparison of Susceptibility Artifact On Rectal Dwi Mri and Rectal Volume Before and After Ultraso PDFНикола ЋопићNo ratings yet
- Multiple B Values of Diffusion-Weighted Magnetic Resonance Imaging in Evaluation of Solid Head and Neck MassesDocument10 pagesMultiple B Values of Diffusion-Weighted Magnetic Resonance Imaging in Evaluation of Solid Head and Neck MassesmohadeseNo ratings yet
- EO10-my M1-Sa DWI AvastinDocument3 pagesEO10-my M1-Sa DWI Avastinserv2008tutbyNo ratings yet
- PENTING ! Can MRI-derived Factors Predict The Survival in Glioblastoma Patients Treated With Postoperative Chemoradiation TherapyDocument7 pagesPENTING ! Can MRI-derived Factors Predict The Survival in Glioblastoma Patients Treated With Postoperative Chemoradiation Therapyafdhal.888980No ratings yet
- Comparison of Different Number of Beams in Intensity Modulated Radiotherapy in Head and Neck CancerDocument11 pagesComparison of Different Number of Beams in Intensity Modulated Radiotherapy in Head and Neck CancerInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Relationship Between Patient Centering, Mean Computed Tomography Numbers and Noise in Abdominal Computed Tomography Influence of Anthropomorphic ParametersDocument7 pagesRelationship Between Patient Centering, Mean Computed Tomography Numbers and Noise in Abdominal Computed Tomography Influence of Anthropomorphic Parameterslorenz_gtlNo ratings yet
- Multiparametric Whole Body MRI With Diffusion Weighted Imaging - 2018 - AcademiDocument10 pagesMultiparametric Whole Body MRI With Diffusion Weighted Imaging - 2018 - AcademiRicardo MirandaNo ratings yet
- RM Rayos Carcinoma Canal AnalDocument9 pagesRM Rayos Carcinoma Canal Analouf81No ratings yet
- Imaging and Radiotherapy Physics - Proposal For PHD Degree: Kathrine - Redalen@Ntnu - NoDocument6 pagesImaging and Radiotherapy Physics - Proposal For PHD Degree: Kathrine - Redalen@Ntnu - Noali alasdyNo ratings yet
- Radiotherapy and Oncology: Original ArticleDocument6 pagesRadiotherapy and Oncology: Original ArticleJheyson Javier Barrios PereiraNo ratings yet
- Magnetic Resonance Only Workflow and Validation of Dose Calculations For Radiotherapy of Prostate CancerDocument6 pagesMagnetic Resonance Only Workflow and Validation of Dose Calculations For Radiotherapy of Prostate CancerJenna WuNo ratings yet
- Whole Tumor Histogram Analysis of DWI and QSI For Differentiating Between Meningioma and Schwannoma: A Pilot StudyDocument7 pagesWhole Tumor Histogram Analysis of DWI and QSI For Differentiating Between Meningioma and Schwannoma: A Pilot StudyKhương Hà NguyễnNo ratings yet
- Magnetic Resonance Only Simulation and Dose Calculation in External Beam Radiation Therapy A Feasibility Study For Pelvic CancersDocument8 pagesMagnetic Resonance Only Simulation and Dose Calculation in External Beam Radiation Therapy A Feasibility Study For Pelvic CancersJenna WuNo ratings yet
- TCRT 2012 500394Document12 pagesTCRT 2012 500394WALTERNo ratings yet
- ANALISIS PERBEDAAN HASIL TREATMENT PLANNING SYSTEM ANTARA TEKNIK PENYINARAN RADIOTERAPI 3D-CRT DAN IMRT PADA KASUS KANKER NASOFARINGDocument6 pagesANALISIS PERBEDAAN HASIL TREATMENT PLANNING SYSTEM ANTARA TEKNIK PENYINARAN RADIOTERAPI 3D-CRT DAN IMRT PADA KASUS KANKER NASOFARINGAnita FitrianaNo ratings yet
- The Role of Magnetic Resonance Imaging in OncologyDocument8 pagesThe Role of Magnetic Resonance Imaging in OncologyHarishNo ratings yet
- Pancreatic Duct TextureDocument9 pagesPancreatic Duct TextureAdarsh GhoshNo ratings yet
- Research ArticleDocument11 pagesResearch Articletsania nkdNo ratings yet
- Dosimetric Comparison of Axilla and Groin Radiotherapy Techniques For High-Risk and Locally Advanced Skin CancerDocument11 pagesDosimetric Comparison of Axilla and Groin Radiotherapy Techniques For High-Risk and Locally Advanced Skin CancergunganiNo ratings yet
- (Review) Comparison of The Clinical Application Value of Mo-Targeted X-Ray, Color Doppler Ultrasound and MRI in Preoperative Comprehensive Evaluation of Breast CancerDocument5 pages(Review) Comparison of The Clinical Application Value of Mo-Targeted X-Ray, Color Doppler Ultrasound and MRI in Preoperative Comprehensive Evaluation of Breast Cancer최윤No ratings yet
- SimuladasDocument9 pagesSimuladasHENRIQUE AUGUSTO LINONo ratings yet
- Magnetic Resonance Imaging - 2012 - Curvo Semedo - Diffusion Weighted MRI in Rectal Cancer Apparent Diffusion CoefficientDocument7 pagesMagnetic Resonance Imaging - 2012 - Curvo Semedo - Diffusion Weighted MRI in Rectal Cancer Apparent Diffusion CoefficientLuis Curvo SemedoNo ratings yet
- Pengaruh Parameter Milliampere-Second (Mas) Terhadap Kualitas Citra Dan Dosis Radiasipada Pemeriksan CT Scan Kepal PediatrikDocument8 pagesPengaruh Parameter Milliampere-Second (Mas) Terhadap Kualitas Citra Dan Dosis Radiasipada Pemeriksan CT Scan Kepal PediatrikAlex BurhanNo ratings yet
- Cine MRI Based Analysis of Intrafractional Motion in Radiation Treatment PlanninDocument14 pagesCine MRI Based Analysis of Intrafractional Motion in Radiation Treatment Planninyuta titeNo ratings yet
- Gadoxetic Acid MRI Predicts Outcomes in Liver CancerDocument10 pagesGadoxetic Acid MRI Predicts Outcomes in Liver CancerMihaela ToaderNo ratings yet
- Three-Dimensional Conformal Radiation Therapy (3DCRT) For Prostate CancerDocument34 pagesThree-Dimensional Conformal Radiation Therapy (3DCRT) For Prostate CancerMuhammad Safwan Ahmad FadzilNo ratings yet
- Image and Pathological Changes After Microwave Ablation of Breast CancerDocument7 pagesImage and Pathological Changes After Microwave Ablation of Breast CancerMalekseuofi مالك السيوفيNo ratings yet
- Magnetic Resonance Imaging - 2002 - Padhani - Dynamic Contrast Enhanced MRI in Clinical Oncology Current Status and FutureDocument16 pagesMagnetic Resonance Imaging - 2002 - Padhani - Dynamic Contrast Enhanced MRI in Clinical Oncology Current Status and FutureWade WilsonNo ratings yet
- CT and MR Imaging of Chronic Subdural Haematomas: A Comparative StudyDocument6 pagesCT and MR Imaging of Chronic Subdural Haematomas: A Comparative StudyYhafapCezNo ratings yet
- Berger 2007Document9 pagesBerger 2007Benfredj KhalilNo ratings yet
- Radiation Physics and ChemistryDocument7 pagesRadiation Physics and ChemistrySiti FairuzNo ratings yet
- Haga 2017Document9 pagesHaga 2017tsania nkdNo ratings yet
- Curroncol 29 00159 v2Document20 pagesCurroncol 29 00159 v2rachid oumouloudNo ratings yet
- Tractography of The BrainDocument11 pagesTractography of The BrainLina ArancibiaNo ratings yet
- Robot-Assisted Microwave Thermoablation of Liver Tumors: A Single-Center ExperienceDocument9 pagesRobot-Assisted Microwave Thermoablation of Liver Tumors: A Single-Center ExperienceMamanya Fadhil HaniNo ratings yet
- A Case Study of DIBH To Spare Abdominal Organs at Risk For Renal Cell Carcinoma MR-Guided RadiotherapyDocument14 pagesA Case Study of DIBH To Spare Abdominal Organs at Risk For Renal Cell Carcinoma MR-Guided Radiotherapyapi-525837437No ratings yet
- Radiotherapy and OncologyDocument7 pagesRadiotherapy and OncologyMichael Steve Camelo GuevaraNo ratings yet
- Vial 2017Document5 pagesVial 2017Varun RathodNo ratings yet
- Establishing diagnostic reference levels for common CT examsDocument5 pagesEstablishing diagnostic reference levels for common CT examsjamesNo ratings yet
- Tander UpDocument8 pagesTander UpGiovanniNo ratings yet
- Assessment of central cartilaginous tumor of the appendicular bone: inter-observer and intermodality agreement and comparison of diagnostic performance of CT and MRIDocument11 pagesAssessment of central cartilaginous tumor of the appendicular bone: inter-observer and intermodality agreement and comparison of diagnostic performance of CT and MRIsilvana mendoncaNo ratings yet
- s40134 018 0262 ZDocument15 pagess40134 018 0262 Zrahmat alfi syahriNo ratings yet
- Differentiation of Benign and Malignant Skeletal Lesions With Quantitative Diffusion Wiughted MRIDocument7 pagesDifferentiation of Benign and Malignant Skeletal Lesions With Quantitative Diffusion Wiughted MRITika wahyuNo ratings yet
- Effect of CT Modality on Pediatric Radiation Doses and Image QualityDocument9 pagesEffect of CT Modality on Pediatric Radiation Doses and Image QualitySoma SweetNo ratings yet
- Diffusion MRIDocument7 pagesDiffusion MRIMoh Hidayat ThahaNo ratings yet
- Artikel MBT Flowrate DCEMRIDocument9 pagesArtikel MBT Flowrate DCEMRILucas ParretNo ratings yet
- 1369 Full PDFDocument9 pages1369 Full PDFIqbal AbdillahNo ratings yet
- Qims 12 01 766Document15 pagesQims 12 01 766Hamza ArjahNo ratings yet
- 11 - Espectroscopia Desmiel Tumefactive - Ikeguchi2018Document8 pages11 - Espectroscopia Desmiel Tumefactive - Ikeguchi2018Henry DanielNo ratings yet
- XDocument6 pagesXShelaErlanggaPutriNo ratings yet
- JCDR 10 TC01Document5 pagesJCDR 10 TC01Muhammad Azhar ImranNo ratings yet
- Immobilisation FFFDocument8 pagesImmobilisation FFFSrinivas VenkataramanNo ratings yet
- 163 FullDocument3 pages163 FullVola FaurisNo ratings yet
- tmp4DFB TMPDocument4 pagestmp4DFB TMPFrontiersNo ratings yet
- NRG Consensus Contouring Guidelines For Postop emCA + CervixDocument12 pagesNRG Consensus Contouring Guidelines For Postop emCA + Cervixgermanfutbol7No ratings yet
- CT venography reliability vs DSADocument7 pagesCT venography reliability vs DSAwan hanisaNo ratings yet
- JMP 41 162Document7 pagesJMP 41 162Ɗḯøɠø Ƥ.No ratings yet
- Ovarian Collision Tumors: Imaging Findings, Pathological Characteristics, Diagnosis, and Differential DiagnosisDocument13 pagesOvarian Collision Tumors: Imaging Findings, Pathological Characteristics, Diagnosis, and Differential DiagnosisPradanaNurOviyantiNo ratings yet
- List Ilmiah Maret 2021Document250 pagesList Ilmiah Maret 2021PradanaNurOviyantiNo ratings yet
- ABC of Heart DiseaseDocument78 pagesABC of Heart DiseaseRolando Reyna100% (2)
- WHO Grading & Diagnostic Imaging For Brain Tumor: Yuyun YueniwatiDocument65 pagesWHO Grading & Diagnostic Imaging For Brain Tumor: Yuyun YueniwatiPradanaNurOviyantiNo ratings yet
- Staging of Multiple Sclerosis (MS) Lesions: Pathology of The Time Frame of MSDocument9 pagesStaging of Multiple Sclerosis (MS) Lesions: Pathology of The Time Frame of MSPradanaNurOviyantiNo ratings yet
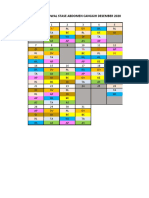
- Jadwal Stase Abdomen DesemberDocument3 pagesJadwal Stase Abdomen DesemberPradanaNurOviyantiNo ratings yet
- Vascular of BodyDocument6 pagesVascular of BodyPradanaNurOviyantiNo ratings yet
- Glioblastoma (GBM) : Corticospinal Tracts Corpus CallosumDocument1 pageGlioblastoma (GBM) : Corticospinal Tracts Corpus CallosumPradanaNurOviyantiNo ratings yet
- 5 6066520397975650349Document9 pages5 6066520397975650349PradanaNurOviyantiNo ratings yet
- Tonsillotomy - Partial - and Complete Tonsillectomy Surgical TechniqueDocument18 pagesTonsillotomy - Partial - and Complete Tonsillectomy Surgical Techniquearsalan adilNo ratings yet
- Andrew Solomon Case Study - EditedDocument5 pagesAndrew Solomon Case Study - EditedJefferson KagiriNo ratings yet
- Introduction in Skeletal System1Document11 pagesIntroduction in Skeletal System1joana cortezNo ratings yet
- 10 Reasons Smoking Is Bad For YouDocument6 pages10 Reasons Smoking Is Bad For YouYuNa YoshinoyaNo ratings yet
- A and P Week 7Document3 pagesA and P Week 7api-316035237No ratings yet
- PT Joint Mobilization TechniquesDocument5 pagesPT Joint Mobilization TechniquesHari PrasadNo ratings yet
- Herd/Flock Health and Medicine for the Exotic Animal PractitionerDocument3 pagesHerd/Flock Health and Medicine for the Exotic Animal PractitionerElena -No ratings yet
- Choledochal CystDocument68 pagesCholedochal CystSyed Waqas HasanNo ratings yet
- Supraglottic Airway Devices A Review in A New Era of Airway Management 2155 6148 1000647Document9 pagesSupraglottic Airway Devices A Review in A New Era of Airway Management 2155 6148 1000647Riris SihotangNo ratings yet
- Iloilo Doctors' College College of Nursing: West Avenue, Molo, Iloilo CityDocument2 pagesIloilo Doctors' College College of Nursing: West Avenue, Molo, Iloilo CityAudrie Allyson GabalesNo ratings yet
- First Aid For Gunshot Wounds and FracturesDocument42 pagesFirst Aid For Gunshot Wounds and FracturesIfedigbo-Ejidike NwamakaNo ratings yet
- Research Article: Garbha Sanskar-Need of Every Expectant Mother For Healthy ProgenyDocument4 pagesResearch Article: Garbha Sanskar-Need of Every Expectant Mother For Healthy ProgenySayaliNo ratings yet
- Establishing Food Allergens Thresholds (Simon Brooke-Taylor PHD)Document40 pagesEstablishing Food Allergens Thresholds (Simon Brooke-Taylor PHD)ARdian RizkyNo ratings yet
- 19 AD CBT Mock Questions A4 V1 PDFDocument29 pages19 AD CBT Mock Questions A4 V1 PDFAncy JustineNo ratings yet
- Topical Antibiotics Appropriate Skin InfectionsDocument4 pagesTopical Antibiotics Appropriate Skin InfectionsniklukNo ratings yet
- Urethral Trauma - Injuries Poisoning - MSD Manual Professional EditionDocument2 pagesUrethral Trauma - Injuries Poisoning - MSD Manual Professional EditionNaufal NaswanNo ratings yet
- (Grade 9) MAPEH (Health) - Drugs (2nd)Document3 pages(Grade 9) MAPEH (Health) - Drugs (2nd)KenNo ratings yet
- Ankylosed Teeth As Abutments For Maxillary Protraction: A Case ReportDocument5 pagesAnkylosed Teeth As Abutments For Maxillary Protraction: A Case Reportdrgeorgejose7818No ratings yet
- NHM Letter World Diabetes DayDocument9 pagesNHM Letter World Diabetes DayAnonymous RCDcVGlFpzNo ratings yet
- Management of Alkali Eye Injury: Abdulla A. Almoosa, MD Muhammad Atif Mian, FrcsedDocument3 pagesManagement of Alkali Eye Injury: Abdulla A. Almoosa, MD Muhammad Atif Mian, FrcsedChandra WulanNo ratings yet
- Typhoid Fever Journal ArticleDocument5 pagesTyphoid Fever Journal ArticleDiana MargaretaNo ratings yet
- Cortical Visual ImpairmentDocument15 pagesCortical Visual ImpairmentsrihandayaniakbarNo ratings yet
- Invasive Cervical Traction Gardner Wells TongsDocument3 pagesInvasive Cervical Traction Gardner Wells TongsErvan Hartanto ErvanNo ratings yet
- K FerhatovicDocument2 pagesK Ferhatovicapi-522063622No ratings yet
- Saritha Front Page HeddingsDocument13 pagesSaritha Front Page Heddingssaritha OrugantiNo ratings yet