You might also like
- Tuberculous Meningitis: Manual of Diagnosis and TherapyFrom EverandTuberculous Meningitis: Manual of Diagnosis and TherapyJerome ChinNo ratings yet
- 1 s2.0 S120197122030031X Main PDFDocument5 pages1 s2.0 S120197122030031X Main PDFJoana MirandaNo ratings yet
- Adewole - Flexible Fiberoptic Bronchoscopy in Respiratory Care Diagnostic Yield, Complications, and Challenges in A Nigerian Tertiary CenterDocument5 pagesAdewole - Flexible Fiberoptic Bronchoscopy in Respiratory Care Diagnostic Yield, Complications, and Challenges in A Nigerian Tertiary CenterXaralyn XaviereNo ratings yet
- Tuberculous Peritonitis The Effectiveness of Diagnostic Laparoscopy and The Perioperative Infectious Prevention - A Case ReportDocument4 pagesTuberculous Peritonitis The Effectiveness of Diagnostic Laparoscopy and The Perioperative Infectious Prevention - A Case ReportDumitru RadulescuNo ratings yet
- Post-Infectious Bronchiolitis Obliterans in Children: A Review of 42 CasesDocument6 pagesPost-Infectious Bronchiolitis Obliterans in Children: A Review of 42 CasescarlaNo ratings yet
- Adhrence Article 1Document6 pagesAdhrence Article 1OBIOMA LILIAN OKWUONUNo ratings yet
- International Journal of Infectious Diseases: SciencedirectDocument8 pagesInternational Journal of Infectious Diseases: SciencedirectMada Pasalli SaludungNo ratings yet
- Use of Inhaled Corticosteroids and The Risk of TubDocument11 pagesUse of Inhaled Corticosteroids and The Risk of TubRuby FirdausNo ratings yet
- Barratt 2018Document21 pagesBarratt 2018Examenes LaboratorioNo ratings yet
- Group C PresentationDocument45 pagesGroup C PresentationFELICIA KASIMUNo ratings yet
- Shankar 2021Document9 pagesShankar 2021fsdfNo ratings yet
- Consensus Statement Management of Drug-Induced LivDocument8 pagesConsensus Statement Management of Drug-Induced LivShannon Marcella EvangelinaNo ratings yet
- Aspergillus Fumigatus During COPD Exacerbation: A Pair-Matched Retrospective StudyDocument8 pagesAspergillus Fumigatus During COPD Exacerbation: A Pair-Matched Retrospective StudyJames 'jps' SimanjuntakNo ratings yet
- Salud Bucal Post CovidDocument14 pagesSalud Bucal Post CovidBelez Jum JumNo ratings yet
- s13741 021 00214 3Document12 pagess13741 021 00214 3Carlos Daniel Rangel MartinezNo ratings yet
- 19 Ninan EtalDocument6 pages19 Ninan EtaleditorijmrhsNo ratings yet
- Perioperative Antibiotic Use in Sleep Surgery: Clinical RelevanceDocument10 pagesPerioperative Antibiotic Use in Sleep Surgery: Clinical RelevanceBRENDA VANESSA TREVIZO ESTRADANo ratings yet
- Etiologi Efusi PleuraDocument5 pagesEtiologi Efusi Pleuratriska antonyNo ratings yet
- Extrapulmonary TuberculosisDocument19 pagesExtrapulmonary Tuberculosisanitaabreu123No ratings yet
- Idiopathic Pulmonary Fibrosis: EditorsDocument260 pagesIdiopathic Pulmonary Fibrosis: EditorsjorgechungNo ratings yet
- The Diagnosis of Pulmonary Tuberculosis: A Korean PerspectiveDocument11 pagesThe Diagnosis of Pulmonary Tuberculosis: A Korean PerspectiveErnest Ang GrekNo ratings yet
- Ref Lapsus 5Document6 pagesRef Lapsus 5ainunNo ratings yet
- Vaccination Efficacy Against post-COVID-19 Symptoms in Delta and Omicron Waves: A Prospective Cohort in East IndonesiaDocument9 pagesVaccination Efficacy Against post-COVID-19 Symptoms in Delta and Omicron Waves: A Prospective Cohort in East IndonesiaIJPHSNo ratings yet
- Dynamic Alterations in The Respiratory Tract Microbiota of Patients With COVID-19 and Its Association With Microbiota in The GutDocument15 pagesDynamic Alterations in The Respiratory Tract Microbiota of Patients With COVID-19 and Its Association With Microbiota in The GutEdgar VázquezNo ratings yet
- International Journal of Infectious Diseases: SciencedirectDocument5 pagesInternational Journal of Infectious Diseases: SciencedirectMuh Syukriadi AnsarNo ratings yet
- Knowledge and Practice of Preventive Measures AgaiDocument28 pagesKnowledge and Practice of Preventive Measures AgaiJoann PunzalanNo ratings yet
- IntJMycobacteriol63258-523108 000843Document6 pagesIntJMycobacteriol63258-523108 000843Andrés UribeNo ratings yet
- Proning in Non-Intubated (PINI) in Times of COVID-19: Case Series and A ReviewDocument7 pagesProning in Non-Intubated (PINI) in Times of COVID-19: Case Series and A ReviewCarlos ZepedaNo ratings yet
- (2021) Pneumoconiosis Current Status and FutureDocument10 pages(2021) Pneumoconiosis Current Status and Futuremuhammad prabu aryandaNo ratings yet
- GulhanDocument9 pagesGulhanYezekael Sebastian QuintinusNo ratings yet
- Laparoscopic Compared With Open Surgery TOADocument7 pagesLaparoscopic Compared With Open Surgery TOARizka AdiNo ratings yet
- Hospital Management of Community-AcquiredDocument5 pagesHospital Management of Community-AcquiredJaerom BernadasNo ratings yet
- Synopsis Frequency of Non-Adherence To Previous Treatment in Relapse Tuberculosis PatientsDocument5 pagesSynopsis Frequency of Non-Adherence To Previous Treatment in Relapse Tuberculosis PatientsAneesUrRahmanNo ratings yet
- Cureus 0010 00000003664Document13 pagesCureus 0010 00000003664Hadley AuliaNo ratings yet
- 23rd Respimirror Bronchiectasis PDFDocument16 pages23rd Respimirror Bronchiectasis PDFmeddyaaNo ratings yet
- 23rd Respimirror BronchiectasisDocument16 pages23rd Respimirror BronchiectasismeddyaaNo ratings yet
- Sino-Orbital Mucormycosis in A COVID-19 Patient: A Case ReportDocument5 pagesSino-Orbital Mucormycosis in A COVID-19 Patient: A Case Reportkarol castellonNo ratings yet
- Ponv InternasionalDocument4 pagesPonv InternasionalRandi KhampaiNo ratings yet
- Active Cycle of Breathing To Respiratory Rate in Patients With Lung TuberculosisDocument10 pagesActive Cycle of Breathing To Respiratory Rate in Patients With Lung TuberculosissiskaNo ratings yet
- Clinical and Radiological Study of Pulmonary Tuberculosis in Diabetes MellitusDocument6 pagesClinical and Radiological Study of Pulmonary Tuberculosis in Diabetes MellitusIJAR JOURNALNo ratings yet
- 34 Iajps34102020Document7 pages34 Iajps34102020iajpsNo ratings yet
- Post-Renal Transplant Infections: Single-Center Experience From NigeriaDocument9 pagesPost-Renal Transplant Infections: Single-Center Experience From NigeriaRaquel JimenezNo ratings yet
- Lio2 7 1909Document6 pagesLio2 7 1909sugar povaNo ratings yet
- Post-Infectious Bronchiolitis Obliterans in Children: A Review of 42 CasesDocument6 pagesPost-Infectious Bronchiolitis Obliterans in Children: A Review of 42 CasesSoniJfreeNo ratings yet
- Thesis TB and ChestDocument5 pagesThesis TB and Chestirugqgajd100% (1)
- Peritoneal Tuberculosis: Advances and Controversies: March 2018Document6 pagesPeritoneal Tuberculosis: Advances and Controversies: March 2018Woobin I Adore YouNo ratings yet
- Convalescent Plasma Therapy in Patients With COVID-19: ConcisereviewDocument7 pagesConvalescent Plasma Therapy in Patients With COVID-19: ConcisereviewendaNo ratings yet
- Adesunkanmi2021 Article ImpactOfTheCOVID-19PandemicOnSDocument8 pagesAdesunkanmi2021 Article ImpactOfTheCOVID-19PandemicOnSCarlosA.DíazNo ratings yet
- 9.tuberculosis Preventive Therapy (TPT) To Prevent Tuberculosis Co-InfectionDocument13 pages9.tuberculosis Preventive Therapy (TPT) To Prevent Tuberculosis Co-InfectionmdvalentNo ratings yet
- Ijcm 2022120215192480 230124 231203 PDFDocument10 pagesIjcm 2022120215192480 230124 231203 PDFVinna KusumawatiNo ratings yet
- Chronic Kidney Disease Risk Factors in Workers ofDocument7 pagesChronic Kidney Disease Risk Factors in Workers ofAmin BashyrNo ratings yet
- Diagnostic Approaches of Pneumonia For Commercial-Scale Biomedical Applications: An OverviewDocument18 pagesDiagnostic Approaches of Pneumonia For Commercial-Scale Biomedical Applications: An OverviewJuviely PremacioNo ratings yet
- Elderly AsthmaDocument16 pagesElderly AsthmarizwanasNo ratings yet
- Diagnostic Approaches of Pneumonia For Commercial-Scale Biomedical Applications: An OverviewDocument18 pagesDiagnostic Approaches of Pneumonia For Commercial-Scale Biomedical Applications: An OverviewNecy Tessa C. AcostaNo ratings yet
- Lung Abscess Secondary To Lung Cancer With Eikenella Corrodens and Streptococcus Anginosus: A Case ReportDocument6 pagesLung Abscess Secondary To Lung Cancer With Eikenella Corrodens and Streptococcus Anginosus: A Case ReportWidiaika Melrisda1106No ratings yet
- ECCO-manage Infections in IBD2021Document35 pagesECCO-manage Infections in IBD2021Ramez AntakiaNo ratings yet
- Epistimologi B.inggrisDocument3 pagesEpistimologi B.inggrisbudiNo ratings yet
- A Descriptive Study To Assess The Knowledge and Practice Regarding Ventilator Associated Pneumonia VAP Critical Care Bundle Among Students of Selected Nursing Colleges of Distt. Mohali, PunjabDocument5 pagesA Descriptive Study To Assess The Knowledge and Practice Regarding Ventilator Associated Pneumonia VAP Critical Care Bundle Among Students of Selected Nursing Colleges of Distt. Mohali, PunjabEditor IJTSRDNo ratings yet
- Prevalence of SARS-COV-2 Units Among Achievers University Students, NigeriaDocument8 pagesPrevalence of SARS-COV-2 Units Among Achievers University Students, NigeriaKIU PUBLICATION AND EXTENSIONNo ratings yet
- Radiologic Manifestations of Pulmonary Tuberculosis in Patients of Intensive Care UnitsDocument6 pagesRadiologic Manifestations of Pulmonary Tuberculosis in Patients of Intensive Care UnitsAnonymous qwH3D0KrpNo ratings yet
- Burn-Like Skin Necrosis in A Patient Following Infusion of Sodium BicarbonateDocument3 pagesBurn-Like Skin Necrosis in A Patient Following Infusion of Sodium BicarbonateViniFortunataNo ratings yet
- Autoimmunity in Common Variable Immunodeficiency A Systematic Review and Meta-AnalysisDocument27 pagesAutoimmunity in Common Variable Immunodeficiency A Systematic Review and Meta-AnalysisPanagiotisStoikosNo ratings yet
- Chromosomal DisorderDocument23 pagesChromosomal DisorderUmair RizwanNo ratings yet
- Head Trauma & Management: Dr. Utham Murali. M.S M.B.A. Asso - Prof of Surgery IMS / MSU / MalaysiaDocument48 pagesHead Trauma & Management: Dr. Utham Murali. M.S M.B.A. Asso - Prof of Surgery IMS / MSU / MalaysiaNinaNo ratings yet
- Concept MapDocument2 pagesConcept MapSkyla FiestaNo ratings yet
- Edward Hammond, Andrew McIndoe, Mark Blunt, John Isaac, Ravi Gill, Mike Herbertson, Sundeep Karadia, Elfyn Thomas, Gareth Wrathall - QBase Anaesthesia_ Volume 2, MCQs for the Final FRCA (v. 2)-Greenwi.pdfDocument249 pagesEdward Hammond, Andrew McIndoe, Mark Blunt, John Isaac, Ravi Gill, Mike Herbertson, Sundeep Karadia, Elfyn Thomas, Gareth Wrathall - QBase Anaesthesia_ Volume 2, MCQs for the Final FRCA (v. 2)-Greenwi.pdfFiaz medicoNo ratings yet
- Diagnosis and Treatment of Ossification of The Posterior Longitudinal Ligament of The Spine: Report of Eight Cases Aad Literature ReviewDocument11 pagesDiagnosis and Treatment of Ossification of The Posterior Longitudinal Ligament of The Spine: Report of Eight Cases Aad Literature Reviewcanhtung1989No ratings yet
- Tumors of Head and Neck RegionDocument94 pagesTumors of Head and Neck Regionpoornima vNo ratings yet
- Jansen Koh SummaryDocument54 pagesJansen Koh SummaryLorraineYongNo ratings yet
- HematomyeliaDocument8 pagesHematomyeliaJessica Seunghye ParkNo ratings yet
- Auticoids Review - of - PharmacologyDocument38 pagesAuticoids Review - of - PharmacologyIqra NasirNo ratings yet
- NSAIDSDocument19 pagesNSAIDSDonna Kelly DuranNo ratings yet
- Renal MCQ DiDocument10 pagesRenal MCQ Diahmed100% (1)
- Pathophysiology SimplifiedDocument321 pagesPathophysiology SimplifiedShaik zubairNo ratings yet
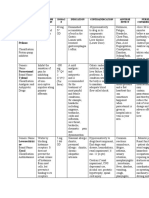
- Sexually Transmitted Diseases: Case Studies 2015 WV Public Health SymposiumDocument28 pagesSexually Transmitted Diseases: Case Studies 2015 WV Public Health SymposiumNikole CrastaNo ratings yet
- Demyelinating DisordersDocument29 pagesDemyelinating Disordersbpt2100% (1)
- BUERGER's Inavasc IV Bandung 8 Nov 2013Document37 pagesBUERGER's Inavasc IV Bandung 8 Nov 2013Deviruchi GamingNo ratings yet
- NCM 118 - Lesson 4 (ARDS)Document4 pagesNCM 118 - Lesson 4 (ARDS)Bobby Christian DuronNo ratings yet
- Continuous Renal Replacement TherapyDocument38 pagesContinuous Renal Replacement Therapyanju rachel joseNo ratings yet
- Pancreatic Function TestsDocument12 pagesPancreatic Function TestsDhera CharlesNo ratings yet
- Psoriasis History OSCEDocument1 pagePsoriasis History OSCEjoseph curranNo ratings yet
- EvaluareDocument2 pagesEvaluareChifor FlorinNo ratings yet
- Nerve Conduction VelocityDocument28 pagesNerve Conduction VelocitySheron MathewNo ratings yet
- Chapter 10 - Trigeminal NeuralgiaDocument5 pagesChapter 10 - Trigeminal NeuralgiaMuhammad IkbarNo ratings yet
- Solution Manual For Understanding The Essentials of Critical Care Nursing 2nd Edition by PerrinDocument15 pagesSolution Manual For Understanding The Essentials of Critical Care Nursing 2nd Edition by PerrinMarieHughesebgjp100% (75)
- Choose The Most Accurate Single Answer: (1 Mark Each)Document9 pagesChoose The Most Accurate Single Answer: (1 Mark Each)Salmonella TyphiNo ratings yet
- Drug StudyDocument3 pagesDrug StudyPsalms Aubrey Domingo AcostaNo ratings yet
- Optic Nerve Tumours: Presenter-Dr Adheela Abdulla Moderator - DR Shikha BassiDocument54 pagesOptic Nerve Tumours: Presenter-Dr Adheela Abdulla Moderator - DR Shikha BassiMohammed Jazeel 2549No ratings yet
- Twenty Pages in The Life of Scheussler Cell Salts FinalDocument23 pagesTwenty Pages in The Life of Scheussler Cell Salts FinalSadia AfrozeNo ratings yet
- Histology of Nervous TissueDocument35 pagesHistology of Nervous TissueGlenn Rey D. AninoNo ratings yet
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDFrom EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDRating: 5 out of 5 stars5/5 (5)
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (404)
- Love Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)From EverandLove Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)Rating: 3 out of 5 stars3/5 (1)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 4.5 out of 5 stars4.5/5 (84)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.From EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Rating: 4.5 out of 5 stars4.5/5 (110)
- The Twentysomething Treatment: A Revolutionary Remedy for an Uncertain AgeFrom EverandThe Twentysomething Treatment: A Revolutionary Remedy for an Uncertain AgeRating: 5 out of 5 stars5/5 (4)
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (39)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsFrom EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo ratings yet
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 4 out of 5 stars4/5 (6)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaFrom EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaRating: 4.5 out of 5 stars4.5/5 (267)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsRating: 5 out of 5 stars5/5 (1)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 4 out of 5 stars4/5 (5)
- I Shouldn't Feel This Way: Name What’s Hard, Tame Your Guilt, and Transform Self-Sabotage into Brave ActionFrom EverandI Shouldn't Feel This Way: Name What’s Hard, Tame Your Guilt, and Transform Self-Sabotage into Brave ActionNo ratings yet
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisFrom EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisRating: 4.5 out of 5 stars4.5/5 (44)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeRating: 2 out of 5 stars2/5 (1)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsFrom EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsRating: 4.5 out of 5 stars4.5/5 (170)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryFrom EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryRating: 4 out of 5 stars4/5 (46)
- Summary: It Didn't Start with You: How Inherited Family Trauma Shapes Who We Are and How to End the Cycle By Mark Wolynn: Key Takeaways, Summary & AnalysisFrom EverandSummary: It Didn't Start with You: How Inherited Family Trauma Shapes Who We Are and How to End the Cycle By Mark Wolynn: Key Takeaways, Summary & AnalysisRating: 5 out of 5 stars5/5 (4)
- To Explain the World: The Discovery of Modern ScienceFrom EverandTo Explain the World: The Discovery of Modern ScienceRating: 3.5 out of 5 stars3.5/5 (51)
- Manipulation: The Ultimate Guide To Influence People with Persuasion, Mind Control and NLP With Highly Effective Manipulation TechniquesFrom EverandManipulation: The Ultimate Guide To Influence People with Persuasion, Mind Control and NLP With Highly Effective Manipulation TechniquesRating: 4.5 out of 5 stars4.5/5 (1412)
- Self-Care for Autistic People: 100+ Ways to Recharge, De-Stress, and Unmask!From EverandSelf-Care for Autistic People: 100+ Ways to Recharge, De-Stress, and Unmask!Rating: 5 out of 5 stars5/5 (1)