You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Levels of Theoretical Thinking in NursingDocument5 pagesLevels of Theoretical Thinking in NursingAmelia ArnisNo ratings yet
- (Bioethics 2) 2.02.01 - Case - Kimberly Bergalis (Pat G)Document3 pages(Bioethics 2) 2.02.01 - Case - Kimberly Bergalis (Pat G)Asylum AllegoryNo ratings yet
- Α Α Α Α-Amylase-Eps: Biosystems S.ADocument1 pageΑ Α Α Α-Amylase-Eps: Biosystems S.ARisqon Anjahiranda AdiputraNo ratings yet
- WGI Benefit GuideDocument32 pagesWGI Benefit GuideSlim ShadyNo ratings yet
- Biomedicines 10 02167Document31 pagesBiomedicines 10 02167Manuela Martín-Bejarano GarcíaNo ratings yet
- Ni Hms 648717Document20 pagesNi Hms 648717Manuela Martín-Bejarano GarcíaNo ratings yet
- Posttraumatic Stress Disorder Subsequent To Apparent Mild Traumatic Brain InjuryDocument12 pagesPosttraumatic Stress Disorder Subsequent To Apparent Mild Traumatic Brain InjuryManuela Martín-Bejarano GarcíaNo ratings yet
- 2016 04 Lancet Article Testosterone Therapy TransgenderDocument3 pages2016 04 Lancet Article Testosterone Therapy TransgenderManuela Martín-Bejarano GarcíaNo ratings yet
- Detecting axonal injury in individual TBI patients using DTIDocument22 pagesDetecting axonal injury in individual TBI patients using DTIManuela Martín-Bejarano GarcíaNo ratings yet
- Functional Connectivity Within Lateral Posterior Parietal Cortex in Moderate To Severe Traumatic Brain InjuryDocument18 pagesFunctional Connectivity Within Lateral Posterior Parietal Cortex in Moderate To Severe Traumatic Brain InjuryManuela Martín-Bejarano GarcíaNo ratings yet
- Chronic White Matter Changes Detected Using Diffusion Tensor Imaging Following Adult Traumatic Brain Injury and Their Relationship To CognitionDocument13 pagesChronic White Matter Changes Detected Using Diffusion Tensor Imaging Following Adult Traumatic Brain Injury and Their Relationship To CognitionManuela Martín-Bejarano GarcíaNo ratings yet
- A Preliminary High-Definition Fiber Tracking Study of The Executive Control Network in Blast-Induced Traumatic Brain InjuryDocument17 pagesA Preliminary High-Definition Fiber Tracking Study of The Executive Control Network in Blast-Induced Traumatic Brain InjuryManuela Martín-Bejarano GarcíaNo ratings yet
- Musindo_2018. Neurocognitive functioning of HIV positive children attending the comprehensive care clinic at Kenyatta national hospital_Exploring neurocognitive deficits and psychosocial risk factors-Musindo18Document6 pagesMusindo_2018. Neurocognitive functioning of HIV positive children attending the comprehensive care clinic at Kenyatta national hospital_Exploring neurocognitive deficits and psychosocial risk factors-Musindo18Manuela Martín-Bejarano GarcíaNo ratings yet
- Weber - 2017. Neurocognitive Development in HIV-positive Children Is Correlated With Plasma Viral Loads in Early Childhood-Weber17Document6 pagesWeber - 2017. Neurocognitive Development in HIV-positive Children Is Correlated With Plasma Viral Loads in Early Childhood-Weber17Manuela Martín-Bejarano GarcíaNo ratings yet
- Judd - 2016. Cognitive Function in Young Persons With and Without Perinatal HIV in The AALPHI Cohort in England: Role of Non-HIV-Related FactorsDocument8 pagesJudd - 2016. Cognitive Function in Young Persons With and Without Perinatal HIV in The AALPHI Cohort in England: Role of Non-HIV-Related FactorsManuela Martín-Bejarano GarcíaNo ratings yet
- Winston - 2013. Neurocognitive Function in HIV+ARTDocument8 pagesWinston - 2013. Neurocognitive Function in HIV+ARTManuela Martín-Bejarano GarcíaNo ratings yet
- Hyperbaric Oxygen For Post Concussive SyndromeDocument28 pagesHyperbaric Oxygen For Post Concussive Syndrometonylee24No ratings yet
- The Effect of Traumatic Brain Injury (TBI) On Cognitive Performance in A Sample of Active Duty U.S. Military Service MembersDocument6 pagesThe Effect of Traumatic Brain Injury (TBI) On Cognitive Performance in A Sample of Active Duty U.S. Military Service MembersManuela Martín-Bejarano GarcíaNo ratings yet
- Arenas-Pinto - 2014. Two Methods To Define Ncog ImpairmentDocument7 pagesArenas-Pinto - 2014. Two Methods To Define Ncog ImpairmentManuela Martín-Bejarano GarcíaNo ratings yet
- Zilioli - 2017. Sueño en Niños Con Padres VihDocument8 pagesZilioli - 2017. Sueño en Niños Con Padres VihManuela Martín-Bejarano GarcíaNo ratings yet
- POTTERTON - 2009. The Effect of A Basic Home Stimulation Programme On Thedevelopment of Young Children Infected With HIV-Potterton10Document5 pagesPOTTERTON - 2009. The Effect of A Basic Home Stimulation Programme On Thedevelopment of Young Children Infected With HIV-Potterton10Manuela Martín-Bejarano GarcíaNo ratings yet
- Meade - 2011. Nihms254795Document19 pagesMeade - 2011. Nihms254795Manuela Martín-Bejarano GarcíaNo ratings yet
- Şalvarlı-Griffiths2019 Article InternetGamingDisorderAndItsAsDocument23 pagesŞalvarlı-Griffiths2019 Article InternetGamingDisorderAndItsAsManuela Martín-Bejarano GarcíaNo ratings yet
- Trail Making TestDocument12 pagesTrail Making TestSónia Mendes100% (1)
- Rice - 2017. Risk For Speech and Language Impairments in Pre-School Aged PHEU-1Document31 pagesRice - 2017. Risk For Speech and Language Impairments in Pre-School Aged PHEU-1Manuela Martín-Bejarano GarcíaNo ratings yet
- Enhanced Recovery After Spine Surgery: A Systematic Review: Neurosurgical FOCUS April 2019Document9 pagesEnhanced Recovery After Spine Surgery: A Systematic Review: Neurosurgical FOCUS April 2019Manuela Martín-Bejarano GarcíaNo ratings yet
- Fpsyt 06 00151Document16 pagesFpsyt 06 00151Manuela Martín-Bejarano GarcíaNo ratings yet
- Clinical and Functional Correlates of Processing Speed in Pediatric Attention-Deficit/Hyperactivity Disorder: A Systematic Review and Meta-AnalysisDocument20 pagesClinical and Functional Correlates of Processing Speed in Pediatric Attention-Deficit/Hyperactivity Disorder: A Systematic Review and Meta-AnalysisManuela Martín-Bejarano GarcíaNo ratings yet
- The PRISMA StatementDocument6 pagesThe PRISMA StatementJeremiahOmwoyoNo ratings yet
- Petranovich 2015Document17 pagesPetranovich 2015Manuela Martín-Bejarano GarcíaNo ratings yet
- Researcharticle Open AccessDocument13 pagesResearcharticle Open AccessManuela Martín-Bejarano GarcíaNo ratings yet
- Van Den HofI - 2019Document12 pagesVan Den HofI - 2019Manuela Martín-Bejarano GarcíaNo ratings yet
- Structural Language, Pragmatic Communication, Behavior, and Social Competence in Children Adopted Internationally: A Pilot StudyDocument12 pagesStructural Language, Pragmatic Communication, Behavior, and Social Competence in Children Adopted Internationally: A Pilot StudyManuela Martín-Bejarano GarcíaNo ratings yet
- Book Excerpt: 'Psychology's Ghost: The Crisis in The Profession and The Way Back'Document5 pagesBook Excerpt: 'Psychology's Ghost: The Crisis in The Profession and The Way Back'WBURNo ratings yet
- PHD Thesis in Prevalence of AsthmaDocument7 pagesPHD Thesis in Prevalence of Asthmabk3q07k5100% (1)
- HOAXESDocument2 pagesHOAXESRovelyn S DupraNo ratings yet
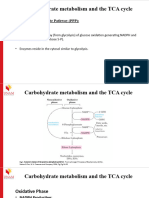
- Carbohydrate Metabolism TCA Cycle - (PPP and Glycogen Metabolism)Document17 pagesCarbohydrate Metabolism TCA Cycle - (PPP and Glycogen Metabolism)Frolian MichaelNo ratings yet
- 2007 CASLPA Position Paper On Dysphagia in AdultsDocument8 pages2007 CASLPA Position Paper On Dysphagia in AdultsEva Sala RenauNo ratings yet
- Quality of Life After Functional Endoscopic Sinus Surgery in Patients With Chronic RhinosinusitisDocument15 pagesQuality of Life After Functional Endoscopic Sinus Surgery in Patients With Chronic RhinosinusitisNarendraNo ratings yet
- An Insight Into Gut Microbiota and Its Functionalities: Atanu Adak Mojibur R. KhanDocument21 pagesAn Insight Into Gut Microbiota and Its Functionalities: Atanu Adak Mojibur R. Khanmacihi7305No ratings yet
- Colibacillosis in Poultry A Disease Overview and TDocument14 pagesColibacillosis in Poultry A Disease Overview and TMonik TanNo ratings yet
- Mrunal Emotional Intelligence:Meaning, Benefits, Models, Case StudiesDocument8 pagesMrunal Emotional Intelligence:Meaning, Benefits, Models, Case StudiesPrateek BayalNo ratings yet
- THE ANTIFUNGAL PROPERTY OF RADISH EXTRACT (RaphanusDocument35 pagesTHE ANTIFUNGAL PROPERTY OF RADISH EXTRACT (RaphanusJaroq Aljon HipolitoNo ratings yet
- Nerve conduction studies normal adult valuesDocument4 pagesNerve conduction studies normal adult valuesFawad JanNo ratings yet
- Drug StudyDocument1 pageDrug StudyTHERESE YZABEL CLOMANo ratings yet
- Cold Chain Distribution Issues at Indo-Euro PharmaDocument19 pagesCold Chain Distribution Issues at Indo-Euro Pharmaely100% (2)
- Reglan Indication Side Effects NursingDocument2 pagesReglan Indication Side Effects NursingRem remNo ratings yet
- Ent Bhalni AnswerDocument120 pagesEnt Bhalni Answerpatilysh1No ratings yet
- MLS & IMT Reading List 3-13Document2 pagesMLS & IMT Reading List 3-13Joseph SabidoNo ratings yet
- Recat Medical BoardDocument5 pagesRecat Medical BoardNavara Naveen kumarNo ratings yet
- Poster of SeptilinDocument1 pagePoster of SeptilinNishtha KumarNo ratings yet
- Jurnal SkripsiDocument10 pagesJurnal Skripsinorma. nlmhNo ratings yet
- TonsilitisDocument23 pagesTonsilitisCrisantaMadrid0% (1)
- Trend Analysis of Exponential Increase of COVID-19 Cases in Pakistan: An InterpretationDocument21 pagesTrend Analysis of Exponential Increase of COVID-19 Cases in Pakistan: An InterpretationBongoNo ratings yet
- Baystate Med CTR Rapid Response Team Recordwith SBARDocument3 pagesBaystate Med CTR Rapid Response Team Recordwith SBARDanishyana DhiwaneoNo ratings yet
- A Study On "Corporate Social Responsibility": Bachelor of Business Management (2011-2014)Document65 pagesA Study On "Corporate Social Responsibility": Bachelor of Business Management (2011-2014)MubeenNo ratings yet
- ACHAI DLaboratory Actiivty 11 - The HeartDocument6 pagesACHAI DLaboratory Actiivty 11 - The HeartSYDNEY JILL ACHAINo ratings yet
- Music Therapy For Non - Alzheimer's Disease Dementia: A Systematic ReviewDocument9 pagesMusic Therapy For Non - Alzheimer's Disease Dementia: A Systematic ReviewMaría DiazNo ratings yet
- Memory Reconsolidation Applied - Calm Your Past To Live Your FutureDocument177 pagesMemory Reconsolidation Applied - Calm Your Past To Live Your Futureiskieh100% (7)