You might also like
- Core-Rules WarcryDocument26 pagesCore-Rules WarcryMiriam H BorowskiNo ratings yet
- Kill Team 2022: Intercession Kill TeamDocument12 pagesKill Team 2022: Intercession Kill Teamminiwars100% (1)
- Parent Safety QuestionsDocument1 pageParent Safety QuestionsKilty ONealNo ratings yet
- Kill Team Balance Dataslate Q2 2022Document1 pageKill Team Balance Dataslate Q2 2022Kilty ONealNo ratings yet
- Regas Basicas Kill Team 2022 InglesDocument3 pagesRegas Basicas Kill Team 2022 InglesminiwarsNo ratings yet
- Kill Team 21 Data Slate 27/09Document2 pagesKill Team 21 Data Slate 27/09Etienne CollignonNo ratings yet
- Safety ScenariosDocument2 pagesSafety ScenariosKilty ONealNo ratings yet
- Knowing My Rules For SafetyDocument2 pagesKnowing My Rules For SafetyKilty ONealNo ratings yet
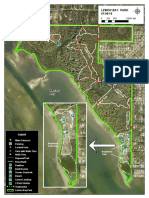
- Lemon Bay Park Florida Map 2018Document1 pageLemon Bay Park Florida Map 2018Kilty ONealNo ratings yet
- J.D. Power 2020 U.S. Insurance Shopping StudyDocument4 pagesJ.D. Power 2020 U.S. Insurance Shopping StudyKilty ONealNo ratings yet
- nc198 1Document2 pagesnc198 1رجول بي الف رجولNo ratings yet
- Physical Fitness Guide PDFDocument20 pagesPhysical Fitness Guide PDFbuckley1212085No ratings yet
- Protecting Your Kids OnlineDocument1 pageProtecting Your Kids OnlineKilty ONealNo ratings yet
- City of Columbus Ohio - Electric Permit ApplicationDocument1 pageCity of Columbus Ohio - Electric Permit ApplicationKilty ONealNo ratings yet
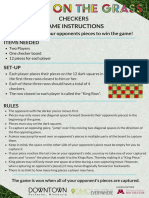
- Checkers InstructionsDocument1 pageCheckers InstructionsKilty ONealNo ratings yet
- Fish Ohio 2020 Catch ReportDocument344 pagesFish Ohio 2020 Catch ReportKilty ONealNo ratings yet
- Glacier Bay Soap Dispenser Kit Installation Guide - HD67726WDocument3 pagesGlacier Bay Soap Dispenser Kit Installation Guide - HD67726WKilty ONealNo ratings yet
- Replacement Parts List: Fairhurst Single-Handle Pull-Down Sprayer Kitchen FaucetDocument1 pageReplacement Parts List: Fairhurst Single-Handle Pull-Down Sprayer Kitchen FaucetKilty ONealNo ratings yet
- Osha 3990Document35 pagesOsha 3990Kilty ONealNo ratings yet
- Glacier Bay Faucet Specifications - HD67726WDocument1 pageGlacier Bay Faucet Specifications - HD67726WKilty ONealNo ratings yet
- Glacier Bay Faucet Installation Guide - HD67726WDocument20 pagesGlacier Bay Faucet Installation Guide - HD67726WKilty ONealNo ratings yet
- Data For K-12 Schools: 14-Day COVID-19 Case Rate by CountyDocument4 pagesData For K-12 Schools: 14-Day COVID-19 Case Rate by Countysonia makloufNo ratings yet
- Citadel Painting SystemDocument1 pageCitadel Painting Systemplume1978100% (1)
- Quarantine Guidance For COVID-19: Who Needs To Quarantine?Document5 pagesQuarantine Guidance For COVID-19: Who Needs To Quarantine?Kilty ONealNo ratings yet
- Essentials of Great SceneryDocument13 pagesEssentials of Great SceneryKilty ONeal100% (1)
- Workbench GuideDocument14 pagesWorkbench GuideKilty ONealNo ratings yet
- LocalTesting FQHCs 12.28.2020Document1 pageLocalTesting FQHCs 12.28.2020Kilty ONealNo ratings yet
- Prevention HDocument2 pagesPrevention Hapi-521325345No ratings yet
- 5 Easy Track PlansDocument12 pages5 Easy Track PlansGlennSheils100% (7)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Womens Health - Post Clinical ReflectionDocument5 pagesWomens Health - Post Clinical Reflectionapi-494643478100% (1)
- Communication Skills For OSCEs Marking SchemeDocument26 pagesCommunication Skills For OSCEs Marking Schememarina shawky100% (1)
- A Simple Approach To Shared Decision Making in Cancer ScreeningDocument6 pagesA Simple Approach To Shared Decision Making in Cancer ScreeningariskaNo ratings yet
- Ebook Ebook PDF Practicing Primary Health Care in Nursing Caring For Populations PDFDocument47 pagesEbook Ebook PDF Practicing Primary Health Care in Nursing Caring For Populations PDFbarbara.coakley466100% (37)
- Autonomy As A Systemic Virtue: A Spinozist Analysis of Autonomy and Shared Decision-Making in HealthcareDocument269 pagesAutonomy As A Systemic Virtue: A Spinozist Analysis of Autonomy and Shared Decision-Making in HealthcareÉlaina Gauthier-MamarilNo ratings yet
- Personalised Care Operating Model 2021Document1 pagePersonalised Care Operating Model 2021daniel.pavonianNo ratings yet
- Population Needs Assessment: A Workbook For Assessing Patients' and Practitioners' Decision Making NeedsDocument40 pagesPopulation Needs Assessment: A Workbook For Assessing Patients' and Practitioners' Decision Making NeedsManuela VituNo ratings yet
- Importance of Risk/benefit Communication in Patient Care and Pharmacy Education: An Expert OpinionDocument7 pagesImportance of Risk/benefit Communication in Patient Care and Pharmacy Education: An Expert OpinionAllyssa FernandezNo ratings yet
- Manual Physical Therapy For Chronic Pain The Complex Whole Is Greater Than The Sum of Its PartsDocument4 pagesManual Physical Therapy For Chronic Pain The Complex Whole Is Greater Than The Sum of Its PartsVizaNo ratings yet
- Nurs FPX 4050 Assessment 3 Care Coordination Presentation To ColleaguesDocument5 pagesNurs FPX 4050 Assessment 3 Care Coordination Presentation To Colleaguesjoohnsmith070No ratings yet
- Do No Harm The Balance of Beneficence And.2Document7 pagesDo No Harm The Balance of Beneficence And.2akunpalsuNo ratings yet
- Evaluating Collaborative Public-Private Partnerships - The Case of Toronto's Smart CityDocument13 pagesEvaluating Collaborative Public-Private Partnerships - The Case of Toronto's Smart CityBusri BusriNo ratings yet
- Review: Historical Origins of Evidence-Based MedicineDocument9 pagesReview: Historical Origins of Evidence-Based MedicineAna PaulaNo ratings yet
- Digital Literac-WPS Office1Document21 pagesDigital Literac-WPS Office1Yamah PrincewillNo ratings yet
- Guidelines For The Provision of Anaesthesia Services (GPAS)Document33 pagesGuidelines For The Provision of Anaesthesia Services (GPAS)florencebucsitNo ratings yet
- 2023 e M Descriptors GuidelinesDocument42 pages2023 e M Descriptors GuidelinesKarunyaNo ratings yet
- Clinical Reasoning in The Health Professions 4th Edition 2019Document1,142 pagesClinical Reasoning in The Health Professions 4th Edition 2019abrazeleke1612No ratings yet
- Interpersonal Relationships e Book Professional Communication Skills For NursesDocument62 pagesInterpersonal Relationships e Book Professional Communication Skills For Nursesjay.huie75398% (44)
- Running Head: Iturralde V. Hilo Medical Center Usa: Case Study 1Document11 pagesRunning Head: Iturralde V. Hilo Medical Center Usa: Case Study 1HugsNo ratings yet
- Physician-Patient Relationship: Four Models of TheDocument6 pagesPhysician-Patient Relationship: Four Models of ThesinghmundayNo ratings yet
- Nursing Student Guide: Associate in Applied Science (A.A.S.)Document42 pagesNursing Student Guide: Associate in Applied Science (A.A.S.)Kenny SharpensteenNo ratings yet
- Maternal and Child Health NursingDocument17 pagesMaternal and Child Health NursingSarah Jane MaganteNo ratings yet
- Use of The Council Health Survey To Assess Shared Governance in A Pediatric Hospital During The COVID-19 PandemicDocument10 pagesUse of The Council Health Survey To Assess Shared Governance in A Pediatric Hospital During The COVID-19 PandemicNurulfitrahhafidNo ratings yet
- Towards Patient-Centered Care For People Living With Kidney DiseaseDocument8 pagesTowards Patient-Centered Care For People Living With Kidney DiseaseEva RetniNo ratings yet
- VA-DoD Clinical Practice Guideline For The Non-Surgical Management of Hip and Knee Osteoarthritis (2020)Document127 pagesVA-DoD Clinical Practice Guideline For The Non-Surgical Management of Hip and Knee Osteoarthritis (2020)william_davison1873No ratings yet
- Patient Education and Counseling: Nicky BrittenDocument5 pagesPatient Education and Counseling: Nicky BrittenEva MutiarasariNo ratings yet
- Self ManagementDocument218 pagesSelf ManagementRiza Muhammad Nuur100% (1)
- ACOG Revises Breast Cancer Screening Guidance - Ob-Gyns Promote Shared Decision Making - ACOGDocument7 pagesACOG Revises Breast Cancer Screening Guidance - Ob-Gyns Promote Shared Decision Making - ACOGLaura RojasNo ratings yet
- Participation in Decision Making QuestionnaireDocument21 pagesParticipation in Decision Making QuestionnaireMorrison Omokiniovo Jessa SnrNo ratings yet
- Filipino Family Physician 2022 60 Pages 23 29Document7 pagesFilipino Family Physician 2022 60 Pages 23 29Pia PalaciosNo ratings yet