You might also like
- SR - Implant SurvivalDocument13 pagesSR - Implant Survivalformula marolisNo ratings yet
- RCT-implant StabilityDocument12 pagesRCT-implant Stabilityformula marolisNo ratings yet
- Archives of Oral Biology: ReviewDocument8 pagesArchives of Oral Biology: Reviewformula marolisNo ratings yet
- Fracture Resistance-ImplantDocument8 pagesFracture Resistance-Implantformula marolisNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5806)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (842)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Safety Data Sheet Electroplating CompoundDocument6 pagesSafety Data Sheet Electroplating CompoundjakinNo ratings yet
- Thermopress 400: One System For Five Thermoplastic MaterialsDocument16 pagesThermopress 400: One System For Five Thermoplastic MaterialsMilan BojovicNo ratings yet
- Employee Satisfaction: Hindustan Zinc Smelter DebariDocument65 pagesEmployee Satisfaction: Hindustan Zinc Smelter Debarirjjain07No ratings yet
- BS 416-1.1990 PDFDocument27 pagesBS 416-1.1990 PDFHaris KyriazisNo ratings yet
- Invatex: AC Cracking AgentDocument4 pagesInvatex: AC Cracking Agentsasko100% (1)
- Technical Card Ck45 Mechanical PropertiesDocument3 pagesTechnical Card Ck45 Mechanical PropertiesNuno Miguel TorcatoNo ratings yet
- The Nano Word 1Document41 pagesThe Nano Word 1Mark Darius A. MabborangNo ratings yet
- Trimethylaluminum/Tma Material Safety Data Sheet: APK (Shanghai) Gas Co., LTDDocument9 pagesTrimethylaluminum/Tma Material Safety Data Sheet: APK (Shanghai) Gas Co., LTDBerkin DereliNo ratings yet
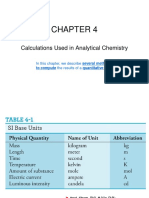
- Calculations Used in Analytical Chemistry: in This Chapter, We Describe Several Methods UsedDocument34 pagesCalculations Used in Analytical Chemistry: in This Chapter, We Describe Several Methods UsedBeyza SuvernNo ratings yet
- Bun PT Introducere - Removal of Cytostatic Drugs From Aquatic Environment A ReviewDocument18 pagesBun PT Introducere - Removal of Cytostatic Drugs From Aquatic Environment A ReviewsorinamotocNo ratings yet
- 4-Kimia Dasar 2 AminaDocument25 pages4-Kimia Dasar 2 AminaDiafabil SpaceNo ratings yet
- Kinetics Lab ReportDocument3 pagesKinetics Lab ReportSarah B - she herNo ratings yet
- MDEADocument13 pagesMDEAAbdulla Alsowaidi100% (1)
- Solution Manual For Chemistry The Molecular Nature of Matter and Change 9th Edition Martin Silberberg Patricia AmateisDocument19 pagesSolution Manual For Chemistry The Molecular Nature of Matter and Change 9th Edition Martin Silberberg Patricia Amateisunwill.eadishvj8p100% (44)
- Exercises: Not One of The Possible Answers ListedDocument12 pagesExercises: Not One of The Possible Answers ListedSarah ChoiNo ratings yet
- Rubber Lining ProcedureDocument39 pagesRubber Lining ProcedureHoras Canman SianiparNo ratings yet
- AkzoNobel-Butanox LPT PDFDocument4 pagesAkzoNobel-Butanox LPT PDFWafa AjiliNo ratings yet
- Pip Veevj001 Gasket Guidelines: VesselsDocument37 pagesPip Veevj001 Gasket Guidelines: VesselsBhavin ParekhNo ratings yet
- Price List: Rain Water Goods Galvanised Iron GutterDocument31 pagesPrice List: Rain Water Goods Galvanised Iron GutterMADUHU KISUJANo ratings yet
- Confronting The Looming Hexavalent Chromium BanDocument2 pagesConfronting The Looming Hexavalent Chromium BananissaNo ratings yet
- Reactor Design: Design Laboratory - Sarkeys E111 September 1, 8, 15 & 22, 2015 CHE 4262-002 Group EDocument39 pagesReactor Design: Design Laboratory - Sarkeys E111 September 1, 8, 15 & 22, 2015 CHE 4262-002 Group EandriasNo ratings yet
- Glucose, Other Reducing Sugars and KetonesDocument12 pagesGlucose, Other Reducing Sugars and KetonesNICOLE ALEXANDRIA SAMIANo ratings yet
- Technology and Livelihood Education 7: Michael R. AñoraDocument37 pagesTechnology and Livelihood Education 7: Michael R. AñoraMICHAEL ANORANo ratings yet
- Biodesulfurization of Petroleum Distillates-Current Status, Opportunities and Future ChallengesDocument20 pagesBiodesulfurization of Petroleum Distillates-Current Status, Opportunities and Future ChallengesNurul AinNo ratings yet
- Thermoforming Process Guide PDFDocument34 pagesThermoforming Process Guide PDFJose Herman Latorre100% (2)
- Performance Evaluation of Hydraulic Fluids For Piston PumpsDocument23 pagesPerformance Evaluation of Hydraulic Fluids For Piston PumpsMohanadNo ratings yet
- Classification of NanomaterialsDocument19 pagesClassification of NanomaterialsNafis AhmedNo ratings yet
- EXP-5 Experiment On Continuous Gas-Solid Adsorption of Co2 Onto Molecular SieveDocument3 pagesEXP-5 Experiment On Continuous Gas-Solid Adsorption of Co2 Onto Molecular SieveSiddharth MohapatraNo ratings yet
- Edited - (Template) Teaching Common Competencies in AFADocument51 pagesEdited - (Template) Teaching Common Competencies in AFAJerrylyn Alegre80% (5)
- Anchoring of Monolithic Refractories - UkDocument9 pagesAnchoring of Monolithic Refractories - Ukantoniorossini100% (1)