You might also like
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (844)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5814)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Neurology QuestionsDocument58 pagesNeurology QuestionsMonica J Ortiz Pereira100% (2)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
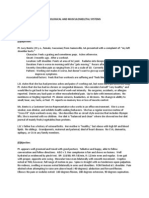
- Soap Note - Musculoskeletal and Nervous SystemsDocument2 pagesSoap Note - Musculoskeletal and Nervous SystemsSummer Keller88% (8)
- Neuro Psych - Antiepileptic Drug ChartDocument5 pagesNeuro Psych - Antiepileptic Drug ChartMonica J Ortiz Pereira100% (1)
- Schematic Pathophysiology CVADocument10 pagesSchematic Pathophysiology CVAheiyu100% (5)
- Charlotte Esser (Eds.) - Environmental Influences On The Immune System-Springer-Verlag Wien (2016) PDFDocument389 pagesCharlotte Esser (Eds.) - Environmental Influences On The Immune System-Springer-Verlag Wien (2016) PDFHemanth Kumar BoyapatiNo ratings yet
- Elmhurst Teacher's Council's Filing With The Illinois Educational Labor Relations BoardDocument27 pagesElmhurst Teacher's Council's Filing With The Illinois Educational Labor Relations BoardDavid GiulianiNo ratings yet
- Ent EssaysDocument78 pagesEnt EssaysNektarios Tsakalos100% (1)
- Coagulation Tests: Clotting Time, Bleeding Time, Prothrombin Time, Activated Partial Thromboplastin TimeDocument15 pagesCoagulation Tests: Clotting Time, Bleeding Time, Prothrombin Time, Activated Partial Thromboplastin TimeAnastasiaNo ratings yet
- Evelyn Handel-Pharmaceutical Care in Targeted Therapy PDFDocument49 pagesEvelyn Handel-Pharmaceutical Care in Targeted Therapy PDFaisyahNo ratings yet
- Mov1. GENERAL - Extrapyramidal Movement DisordersDocument25 pagesMov1. GENERAL - Extrapyramidal Movement DisordersMonica J Ortiz PereiraNo ratings yet
- Mov22. Hyperkinetic Disorders 3 (Tics, Myoclonus, Other)Document6 pagesMov22. Hyperkinetic Disorders 3 (Tics, Myoclonus, Other)Monica J Ortiz PereiraNo ratings yet
- Gastroenterology - Pancreatitis PDFDocument2 pagesGastroenterology - Pancreatitis PDFMonica J Ortiz PereiraNo ratings yet
- Met5. Mitochondrial DisordersDocument8 pagesMet5. Mitochondrial DisordersMonica J Ortiz PereiraNo ratings yet
- Gastroenterology - Pancreatitis PDFDocument2 pagesGastroenterology - Pancreatitis PDFMonica J Ortiz PereiraNo ratings yet
- The Basic Science of Articular Cartilage: Structure, Composition, and FunctionDocument8 pagesThe Basic Science of Articular Cartilage: Structure, Composition, and FunctionMonica J Ortiz PereiraNo ratings yet
- Gastroenterology - Malabsorption PDFDocument1 pageGastroenterology - Malabsorption PDFMonica J Ortiz PereiraNo ratings yet
- Vitamins: Endocrine System, Metabolism: VitaminsDocument25 pagesVitamins: Endocrine System, Metabolism: VitaminsMonica J Ortiz PereiraNo ratings yet
- Cancer Trials Terminology Study Design StatsDocument3 pagesCancer Trials Terminology Study Design StatsMonica J Ortiz PereiraNo ratings yet
- Nephrology MCQ PDFDocument7 pagesNephrology MCQ PDFMonica J Ortiz PereiraNo ratings yet
- Generic Name Brand Name Abbreviation: © 2017 Find Your Script HIV Medications - Drug Names Quick SheetDocument1 pageGeneric Name Brand Name Abbreviation: © 2017 Find Your Script HIV Medications - Drug Names Quick SheetMonica J Ortiz PereiraNo ratings yet
- Usmlestep2cs 2Document100 pagesUsmlestep2cs 2Monica J Ortiz PereiraNo ratings yet
- Note. Includes Dietary and Supplemental Nutrition IntakeDocument5 pagesNote. Includes Dietary and Supplemental Nutrition IntakeMonica J Ortiz PereiraNo ratings yet
- Neurosyphilis: Pathology, Clinical FeaturesDocument6 pagesNeurosyphilis: Pathology, Clinical FeaturesMonica J Ortiz PereiraNo ratings yet
- DS SalbutamolDocument1 pageDS SalbutamolLarr SumalpongNo ratings yet
- Topic 1: Pros and Cons of Making Friends Virtually Claim of Fact Claim of Policy Claim of ValueDocument2 pagesTopic 1: Pros and Cons of Making Friends Virtually Claim of Fact Claim of Policy Claim of ValueChristian GinebreNo ratings yet
- Civil Society and COVID-19 Pandemic in Nagaland: Response in A Democratic SocietyDocument6 pagesCivil Society and COVID-19 Pandemic in Nagaland: Response in A Democratic SocietyMamta AgarwalNo ratings yet
- Streptococcus SPPDocument52 pagesStreptococcus SPPdrnuaman5No ratings yet
- Akta Binatang 1953Document48 pagesAkta Binatang 1953Nur AnisaNo ratings yet
- 4973618841167dcf734ab5fa9d6c6f47Document8 pages4973618841167dcf734ab5fa9d6c6f47Nazarii KordupelNo ratings yet
- Hearing Assessment in Co-Existing Condition With Developmental DisordersDocument43 pagesHearing Assessment in Co-Existing Condition With Developmental DisordersMSc Audio BNo ratings yet
- Cast Techniques For Ortho-1Document74 pagesCast Techniques For Ortho-1Quentene odongoNo ratings yet
- Barrett OesephegusDocument22 pagesBarrett Oesephegusnour mohammadNo ratings yet
- Prevalence and Factors Associated With Hypertension in Pregnancy Among Pregnant Women Attending Fort Portal Regional Referral Hospital in UgandaDocument10 pagesPrevalence and Factors Associated With Hypertension in Pregnancy Among Pregnant Women Attending Fort Portal Regional Referral Hospital in UgandaKIU PUBLICATION AND EXTENSIONNo ratings yet
- Cancer Rehabilitation.: Particularly With Aspects On Physical ImpairmentsDocument10 pagesCancer Rehabilitation.: Particularly With Aspects On Physical Impairmentsnandhini raguNo ratings yet
- 10.7556 Jaoa.1997.97.1.22Document2 pages10.7556 Jaoa.1997.97.1.22Brandon CoombsNo ratings yet
- Intestinal FlukesDocument3 pagesIntestinal FlukesStephany Polinar0% (1)
- DeliriumDocument37 pagesDeliriumalishba iqbal 1112No ratings yet
- Report NaveenDocument3 pagesReport NaveennaveenNo ratings yet
- Interesting Phobias (Fears) : Preda Călin Ștefan Cls. A VII - A B Școala Gimnazială Sfinții Voievozi"Document4 pagesInteresting Phobias (Fears) : Preda Călin Ștefan Cls. A VII - A B Școala Gimnazială Sfinții Voievozi"Preda MirelaNo ratings yet
- Tyrosinemia Type 1Document8 pagesTyrosinemia Type 1Muhammad LawalNo ratings yet
- MCN National HealthDocument4 pagesMCN National HealthCamille RamosNo ratings yet
- Taller Hardy WeinbergDocument2 pagesTaller Hardy WeinbergValery Johana Bohorquez GarciaNo ratings yet
- Ettinger 2005Document7 pagesEttinger 2005Santy P Vásconez CalderónNo ratings yet
- RetinaDocument76 pagesRetinaSarahNo ratings yet
- Management of Disease Through Yoga and Nature CureDocument17 pagesManagement of Disease Through Yoga and Nature CureAnushree ChauhanNo ratings yet
- CIF - Version 7wordDocument3 pagesCIF - Version 7wordBALIUAG DISTRICT LABORATORYNo ratings yet