You might also like
- Assessment of Maternal Knowledge, Attitudes, and Practices Regarding Breastfeeding at Kampala International Teaching Hospital A Study Spanning May 2021 To July 2022Document15 pagesAssessment of Maternal Knowledge, Attitudes, and Practices Regarding Breastfeeding at Kampala International Teaching Hospital A Study Spanning May 2021 To July 2022KIU PUBLICATION AND EXTENSIONNo ratings yet
- 9B. Effectiveness of Educational Intervention On Breastfeeding Among Primi Pregnant WomanDocument6 pages9B. Effectiveness of Educational Intervention On Breastfeeding Among Primi Pregnant Womanagaua16No ratings yet
- Gestational Age, Mode of Birth and Breastmilk Feeding All Influence Acute Early Childhood Gastroenteritis: A Record-Linkage Cohort StudyDocument10 pagesGestational Age, Mode of Birth and Breastmilk Feeding All Influence Acute Early Childhood Gastroenteritis: A Record-Linkage Cohort Studynavali rahmaNo ratings yet
- Nutrients 15 00988Document17 pagesNutrients 15 00988VIRGINA PUTRINo ratings yet
- Am J Clin Nutr 2007 Fewtrell 635S 8SDocument4 pagesAm J Clin Nutr 2007 Fewtrell 635S 8SpiterwiselyNo ratings yet
- Am J Clin Nutr 2007 Fewtrell 635S 8SggDocument4 pagesAm J Clin Nutr 2007 Fewtrell 635S 8SggMariaNo ratings yet
- Jurnal Asi EkslusifDocument9 pagesJurnal Asi EkslusifNiine FebriyantiNo ratings yet
- Awareness and Practice of Breast Feeding Among Mothers at Kiryandongo District HospitalDocument12 pagesAwareness and Practice of Breast Feeding Among Mothers at Kiryandongo District HospitalKIU PUBLICATION AND EXTENSIONNo ratings yet
- Breastfeeding and The Risk For Diarrhea Morbidity and MortalityDocument12 pagesBreastfeeding and The Risk For Diarrhea Morbidity and MortalityMariam AbdAlkarimNo ratings yet
- Tuthill, E., & McGrath, J. (2013) - The Importance of Breastfeeding Education For All Women of Childbearing AgeDocument2 pagesTuthill, E., & McGrath, J. (2013) - The Importance of Breastfeeding Education For All Women of Childbearing AgesebastixmasterNo ratings yet
- The Inverted Syringe Technique For Management of I PDFDocument9 pagesThe Inverted Syringe Technique For Management of I PDFAri SapitriNo ratings yet
- How To Achieve Long-Term Breast-Feeding: Factors Associated With Early DiscontinuationDocument8 pagesHow To Achieve Long-Term Breast-Feeding: Factors Associated With Early DiscontinuationSST KNo ratings yet
- Factors Associated With Cessation of Exclusive Breastfeeding at 1 and 2 Months Postpartum in TaiwanDocument7 pagesFactors Associated With Cessation of Exclusive Breastfeeding at 1 and 2 Months Postpartum in TaiwanHilda HildaNo ratings yet
- Effect of Kangaroo Mother Care On The Likelihood of Breastfeeding From Birth Up To 6 Months of Age: A Meta-AnalysisDocument10 pagesEffect of Kangaroo Mother Care On The Likelihood of Breastfeeding From Birth Up To 6 Months of Age: A Meta-AnalysispurplemmyNo ratings yet
- Factors Associated With Cessation of Exclusive Breastfeeding at 1 and 2 Months Postpartum in TaiwanDocument7 pagesFactors Associated With Cessation of Exclusive Breastfeeding at 1 and 2 Months Postpartum in TaiwanHilda HildaNo ratings yet
- Pushpa Synopsis-1Document33 pagesPushpa Synopsis-1mahaNo ratings yet
- Anwar and AzniahDocument10 pagesAnwar and Azniahadhe yuniarNo ratings yet
- s13006 020 00278 9Document11 pagess13006 020 00278 9nosh.rose95No ratings yet
- Studyprotocol Open AccessDocument10 pagesStudyprotocol Open AccessMyrza AkbariNo ratings yet
- Breastfeeding Is Priceless: There Is No Substitute For Human MilkDocument4 pagesBreastfeeding Is Priceless: There Is No Substitute For Human MilkmeetNo ratings yet
- Nutrients: Breastfeeding Di Breastfeeding CessationDocument10 pagesNutrients: Breastfeeding Di Breastfeeding CessationEliyyasa Vina ErikmetikaNo ratings yet
- Contoh JurnalDocument7 pagesContoh Jurnaldr. igaNo ratings yet
- Breastfeeding and The Use of Human MilkDocument4 pagesBreastfeeding and The Use of Human Milkfurqon alNo ratings yet
- Notes On Exclusive BreastfeedingDocument6 pagesNotes On Exclusive BreastfeedingNdem BasseyNo ratings yet
- Jurnal 2 PDFDocument17 pagesJurnal 2 PDFyayu yuliantiNo ratings yet
- The Effect of Education Lactation On Breastfeeding Behavior Infant 0-6 Months in Kendari IndonesiaDocument12 pagesThe Effect of Education Lactation On Breastfeeding Behavior Infant 0-6 Months in Kendari IndonesiaDessy WahyuniNo ratings yet
- Dietary Patterns and Their Association With Breast Milk Macronutrient Composition Among Lactating WomenDocument10 pagesDietary Patterns and Their Association With Breast Milk Macronutrient Composition Among Lactating WomenCamii CvNo ratings yet
- Research Article: An Assessment of The Breastfeeding Practices and Infant Feeding Pattern Among Mothers in MauritiusDocument9 pagesResearch Article: An Assessment of The Breastfeeding Practices and Infant Feeding Pattern Among Mothers in MauritiusNurhikmah RnNo ratings yet
- Nutrients 13 02376Document28 pagesNutrients 13 02376Garuba Olayinka DhikrullahiNo ratings yet
- Zainab ProjectDocument35 pagesZainab ProjectOpeyemi JamalNo ratings yet
- Icash DiarrheaandbrestfeedingDocument8 pagesIcash Diarrheaandbrestfeedingmaryano 0015No ratings yet
- Breastfeeding Awareness and Practices in AbakalikiDocument14 pagesBreastfeeding Awareness and Practices in AbakalikiBusiness ProposalNo ratings yet
- Nutrients: The Early Introduction of Complementary (Solid) Foods: A Prospective Cohort Study of Infants in Chengdu, ChinaDocument10 pagesNutrients: The Early Introduction of Complementary (Solid) Foods: A Prospective Cohort Study of Infants in Chengdu, ChinaCarlosPazNo ratings yet
- International Code of Marketing of BreastDocument4 pagesInternational Code of Marketing of BreastSalsabil Sekar NabilaNo ratings yet
- TRCN Paper 2Document17 pagesTRCN Paper 2Chika JonesNo ratings yet
- Issues Related To Breastfeeding in The First Six Months of Life in An Urban Tertiary Care HospitalDocument7 pagesIssues Related To Breastfeeding in The First Six Months of Life in An Urban Tertiary Care HospitalVanyaNo ratings yet
- Efectele Pe Termen Lung Ale Alaptatului OMSDocument74 pagesEfectele Pe Termen Lung Ale Alaptatului OMSbobocraiNo ratings yet
- RESEARCH093016Document28 pagesRESEARCH093016Satra Sabbuh100% (1)
- 2018 Article 1076Document9 pages2018 Article 1076FandaruzzahraPutriPerdaniNo ratings yet
- Effectiveness of Structured Teaching Programme On Knowledge Regarding Weaning Among Mothers of InfantsDocument5 pagesEffectiveness of Structured Teaching Programme On Knowledge Regarding Weaning Among Mothers of InfantsEditor IJTSRD100% (1)
- Breastfeeding Uncovering Barriers and Offering SolutionsDocument6 pagesBreastfeeding Uncovering Barriers and Offering SolutionsSuéllen EmidioNo ratings yet
- D Rug Excretion Into Breast Milk-Overview: Shinya Ito, Amy LeeDocument11 pagesD Rug Excretion Into Breast Milk-Overview: Shinya Ito, Amy LeeRonald Omar OrellanaNo ratings yet
- 2015 Article 1030 PDFDocument15 pages2015 Article 1030 PDFMini Bekti NingsihNo ratings yet
- Evidence of Inflated Exclusive Breastfeeding Estimates From A Clinical Trial in BangladeshDocument5 pagesEvidence of Inflated Exclusive Breastfeeding Estimates From A Clinical Trial in BangladeshSlamet Tejo PramonoNo ratings yet
- Maternal Child Nutrition - 2011 - Senarath - Complementary Feeding Practices in South Asia Analyses of Recent NationalDocument6 pagesMaternal Child Nutrition - 2011 - Senarath - Complementary Feeding Practices in South Asia Analyses of Recent NationalAdnan AhmadNo ratings yet
- Chapter 1-3 ThesisDocument20 pagesChapter 1-3 ThesisMarianne Gonzales100% (1)
- Adaptation and Psychometric Evaluation of The Breastfeeding Self-Efficacy Scale To Assess Exclusive BreastfeedingDocument14 pagesAdaptation and Psychometric Evaluation of The Breastfeeding Self-Efficacy Scale To Assess Exclusive Breastfeedingcardenala haganinthaNo ratings yet
- Maternal and Child-Related Factors Influencing Breastfeeding Practices Among Children 0 To 24 Months in Bushenyi District, UgandaDocument9 pagesMaternal and Child-Related Factors Influencing Breastfeeding Practices Among Children 0 To 24 Months in Bushenyi District, UgandaKIU PUBLICATION AND EXTENSIONNo ratings yet
- Jurnal A1Document9 pagesJurnal A1Novi JuliasariNo ratings yet
- Intl J Gynecology Obste - 2023 - Killeen - Using FIGO Nutrition Checklist Counselling in Pregnancy A Review To SupportDocument12 pagesIntl J Gynecology Obste - 2023 - Killeen - Using FIGO Nutrition Checklist Counselling in Pregnancy A Review To SupportJuan Carlos CachonNo ratings yet
- Advance Concept in NursingDocument17 pagesAdvance Concept in NursingAnita NakhshabNo ratings yet
- Cato 2017Document13 pagesCato 2017Farin MauliaNo ratings yet
- Drivers and Challenges of Exclusive Breastfeeding in West AfricaDocument5 pagesDrivers and Challenges of Exclusive Breastfeeding in West AfricaKIU PUBLICATION AND EXTENSIONNo ratings yet
- Practices of Exclusive Breastfeeding Among Lactating Mothers Attending Care at HoimaDocument7 pagesPractices of Exclusive Breastfeeding Among Lactating Mothers Attending Care at HoimaKIU PUBLICATION AND EXTENSIONNo ratings yet
- Breastfeeding - Jurnal 1Document7 pagesBreastfeeding - Jurnal 1Sintha MukinNo ratings yet
- Knowledge, Attitude and Practices Towards Breast Feeding Among Lactating Mothers in King George Hospital, A Tertiary Care CenterDocument10 pagesKnowledge, Attitude and Practices Towards Breast Feeding Among Lactating Mothers in King George Hospital, A Tertiary Care CenterIJAR JOURNALNo ratings yet
- Durasi EpingDocument13 pagesDurasi EpingRony TambaNo ratings yet
- Exclusive Breastfeeding and Under-Five Mortality, 2006-2014: A Cross-National Analysis of 57 Low-and-Middle Income CountriesDocument9 pagesExclusive Breastfeeding and Under-Five Mortality, 2006-2014: A Cross-National Analysis of 57 Low-and-Middle Income CountriesBunga RamadhaniNo ratings yet
- Human Milk: Composition, Clinical Benefits and Future Opportunities: 90th Nestlé Nutrition Institute Workshop, Lausanne, October-November 2017From EverandHuman Milk: Composition, Clinical Benefits and Future Opportunities: 90th Nestlé Nutrition Institute Workshop, Lausanne, October-November 2017No ratings yet
- The Effect of Bovine Colostrum/egg Supplementation Compared With Corn/soy Flour in Young Malawian Children: A Randomized, Controlled Clinical TrialDocument8 pagesThe Effect of Bovine Colostrum/egg Supplementation Compared With Corn/soy Flour in Young Malawian Children: A Randomized, Controlled Clinical TrialSukma DewiNo ratings yet
- Late Eating Is Associated With Cardiometabolic Risk Traits, Obesogenic Behaviors, and Impaired Weight LossDocument8 pagesLate Eating Is Associated With Cardiometabolic Risk Traits, Obesogenic Behaviors, and Impaired Weight LossSukma DewiNo ratings yet
- Are Our Babies Off To A Healthy Start? The State of Implementation of The Global Strategy For Infant and Young Child Feeding in EuropeDocument12 pagesAre Our Babies Off To A Healthy Start? The State of Implementation of The Global Strategy For Infant and Young Child Feeding in EuropeSukma DewiNo ratings yet
- Impact of Gestational Diabetes Mellitus On The Duration of Breastfeeding in Primiparous Women: An Observational Cohort StudyDocument8 pagesImpact of Gestational Diabetes Mellitus On The Duration of Breastfeeding in Primiparous Women: An Observational Cohort StudySukma DewiNo ratings yet
- s13006 021 00366 4Document9 pagess13006 021 00366 4Sukma DewiNo ratings yet
- Intimate Partner Violence and Exclusive Breastfeeding of Infants: Analysis of The 2013 Nigeria Demographic and Health SurveyDocument11 pagesIntimate Partner Violence and Exclusive Breastfeeding of Infants: Analysis of The 2013 Nigeria Demographic and Health SurveySukma DewiNo ratings yet
- Using Animation To Teach Breastfeeding Physiology: A Proof of Concept StudyDocument9 pagesUsing Animation To Teach Breastfeeding Physiology: A Proof of Concept StudySukma DewiNo ratings yet
- The Effect of Bovine Colostrum/egg Supplementation Compared With Corn/soy Flour in Young Malawian Children: A Randomized, Controlled Clinical TrialDocument8 pagesThe Effect of Bovine Colostrum/egg Supplementation Compared With Corn/soy Flour in Young Malawian Children: A Randomized, Controlled Clinical TrialSukma DewiNo ratings yet
- Impact of Gestational Diabetes Mellitus On The Duration of Breastfeeding in Primiparous Women: An Observational Cohort StudyDocument8 pagesImpact of Gestational Diabetes Mellitus On The Duration of Breastfeeding in Primiparous Women: An Observational Cohort StudySukma DewiNo ratings yet
- Late Eating Is Associated With Cardiometabolic Risk Traits, Obesogenic Behaviors, and Impaired Weight LossDocument8 pagesLate Eating Is Associated With Cardiometabolic Risk Traits, Obesogenic Behaviors, and Impaired Weight LossSukma DewiNo ratings yet
- s13006 021 00366 4Document9 pagess13006 021 00366 4Sukma DewiNo ratings yet
- EVIDENCE BASED PRACTICE PADA PELAYANAN KEHAMILAN - PPT DownloadDocument1 pageEVIDENCE BASED PRACTICE PADA PELAYANAN KEHAMILAN - PPT DownloadSukma DewiNo ratings yet
- Intimate Partner Violence and Exclusive Breastfeeding of Infants: Analysis of The 2013 Nigeria Demographic and Health SurveyDocument11 pagesIntimate Partner Violence and Exclusive Breastfeeding of Infants: Analysis of The 2013 Nigeria Demographic and Health SurveySukma DewiNo ratings yet
- Intimate Partner Violence and Exclusive Breastfeeding of Infants: Analysis of The 2013 Nigeria Demographic and Health SurveyDocument11 pagesIntimate Partner Violence and Exclusive Breastfeeding of Infants: Analysis of The 2013 Nigeria Demographic and Health SurveySukma DewiNo ratings yet
- Evidence Based Practice Pada Pelayanan Kehamilan - PPT DownloadDocument1 pageEvidence Based Practice Pada Pelayanan Kehamilan - PPT DownloadSukma Dewi100% (1)
- Dietary Fiber Intervention On Gut Microbiota Composition in Healthy Adults: A Systematic Review and Meta-AnalysisDocument19 pagesDietary Fiber Intervention On Gut Microbiota Composition in Healthy Adults: A Systematic Review and Meta-AnalysisSukma DewiNo ratings yet
- Khairiani Askeb PatologiDocument5 pagesKhairiani Askeb PatologiSukma DewiNo ratings yet
- Evidence Based Practice Pada Pelayanan Kehamilan - PPT DownloadDocument1 pageEvidence Based Practice Pada Pelayanan Kehamilan - PPT DownloadSukma DewiNo ratings yet
- Stree Roga Vigyan-Mallikarjuna With MCQs PDFDocument20 pagesStree Roga Vigyan-Mallikarjuna With MCQs PDFCHAUKHAMBHA PRAKASHAKNo ratings yet
- Drugs Producing Uterine CONTRACTIONS (Oxytocic Drugs) : Oxytocin Ergot Alkaloids ProstaglandinsDocument9 pagesDrugs Producing Uterine CONTRACTIONS (Oxytocic Drugs) : Oxytocin Ergot Alkaloids ProstaglandinsFaris Jamal Abu Za'nounehNo ratings yet
- Reproductive Health SUPER NOTES BY SEEPDocument2 pagesReproductive Health SUPER NOTES BY SEEPmohammedibnu456No ratings yet
- Obs & GynDocument121 pagesObs & GynSaya K. AkremNo ratings yet
- Disordered Proliferative Endometrium Causes and SymptomsDocument7 pagesDisordered Proliferative Endometrium Causes and SymptomsMuhammad BabarNo ratings yet
- InfertilityDocument42 pagesInfertilityjoycechicagoNo ratings yet
- Pregnancy Walking WorkoutDocument2 pagesPregnancy Walking WorkoutnaturalchildbirthNo ratings yet
- Clomifene Citrate (Ikaclomin)Document9 pagesClomifene Citrate (Ikaclomin)asdwasdNo ratings yet
- Mirena BrochureDocument24 pagesMirena BrochureNamrata HarishNo ratings yet
- Vital Statistics DefinitionDocument3 pagesVital Statistics Definition0pp0ppNo ratings yet
- Sambit Mukhopadhyay, Edward Morris, Sabaratnam Arulkumaran - Algorithms For Obstetrics and Gynaecology-Oxford University Press (2014)Document327 pagesSambit Mukhopadhyay, Edward Morris, Sabaratnam Arulkumaran - Algorithms For Obstetrics and Gynaecology-Oxford University Press (2014)Asmath100% (1)
- Fix Daftar Pustaka MaiDocument3 pagesFix Daftar Pustaka MaiMaimunahNo ratings yet
- Introduction To Concept of Obstetrical NSGDocument11 pagesIntroduction To Concept of Obstetrical NSGswethashaki100% (2)
- Ceklis APN 1920Document12 pagesCeklis APN 1920wahyu kijang ramadhanNo ratings yet
- Jadwal Simposium Dan Workshop PIT FETOMATERNAL FINALDocument26 pagesJadwal Simposium Dan Workshop PIT FETOMATERNAL FINALBill HarmanNo ratings yet
- Ovarian Cyst: ClassificationDocument31 pagesOvarian Cyst: ClassificationZozo Shadap100% (2)
- ProlapseDocument51 pagesProlapsejijaniNo ratings yet
- Neonatal and Maternal Complications of Placenta Praevia and Its Risk Factors in Tikur Anbessa Specialized and Gandhi Memorial Hospitals. Unmatched Case-Control StudyDocument10 pagesNeonatal and Maternal Complications of Placenta Praevia and Its Risk Factors in Tikur Anbessa Specialized and Gandhi Memorial Hospitals. Unmatched Case-Control StudyLarassati YayaNo ratings yet
- Del Suite Report RSCM 7 April 2017 Final Edit Banget Sekali Dengan DataDocument22 pagesDel Suite Report RSCM 7 April 2017 Final Edit Banget Sekali Dengan DataFedrik Monte Kristo LimbongNo ratings yet
- Benefits of Contraceptives SpeechDocument12 pagesBenefits of Contraceptives SpeechDaniela BallezaNo ratings yet
- Reaction Paper Rizal PlumaDocument33 pagesReaction Paper Rizal PlumaJazzd Sy Gregorio0% (1)
- Abnormal PuerperiumDocument23 pagesAbnormal PuerperiumLynee OlvianaNo ratings yet
- D e M o GR Ap Hy, Fa Mi Ly PL An Ni N G An D C o NTDocument11 pagesD e M o GR Ap Hy, Fa Mi Ly PL An Ni N G An D C o NTDr-Sanjay SinghaniaNo ratings yet
- Fdar-Charting DatoonDocument5 pagesFdar-Charting DatoonDae Nicole Lizbette DatoonNo ratings yet
- Medicult Case StudyDocument3 pagesMedicult Case Studyrandy ambogNo ratings yet
- Jurnal Ultrasound 1Document6 pagesJurnal Ultrasound 1weniNo ratings yet
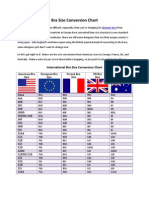
- Bra Size Conversion ChartDocument3 pagesBra Size Conversion ChartTop Drawer Lingerie100% (1)
- Assessment of Labor Progression by Intrapartum Ultrasonography Among Term Nulliparous WomenDocument5 pagesAssessment of Labor Progression by Intrapartum Ultrasonography Among Term Nulliparous WomenFrancesca Doreen VegaNo ratings yet
- Morente, Sonny Ma. HizolaDocument5 pagesMorente, Sonny Ma. HizolasonnymorenteNo ratings yet
- 51 EpisiotomyDocument21 pages51 Episiotomydr_asaleh100% (2)