You might also like
- Wrigley CalculationDocument13 pagesWrigley CalculationAnindito W WicaksonoNo ratings yet
- Understanding Acute Heart Failure: Pathophysiology and DiagnosisDocument8 pagesUnderstanding Acute Heart Failure: Pathophysiology and DiagnosisdidiNo ratings yet
- Físico Patología Falla CardiacaDocument19 pagesFísico Patología Falla CardiacavictorNo ratings yet
- Kjim 2017 355Document12 pagesKjim 2017 355Carolina Aguilar OtáloraNo ratings yet
- Primer: Acute Heart FailureDocument15 pagesPrimer: Acute Heart FailurenicolasNo ratings yet
- ADHF ManagementDocument6 pagesADHF ManagementEsti YunitaNo ratings yet
- Decompensated Heart Failure: Insuficiência Cardíaca DescompensadaDocument9 pagesDecompensated Heart Failure: Insuficiência Cardíaca DescompensadakunkkonkNo ratings yet
- Hiponatremia in CHFDocument5 pagesHiponatremia in CHFnurminsyahNo ratings yet
- Insuficiencia Cardiaca Neyssa KimeeDocument33 pagesInsuficiencia Cardiaca Neyssa KimeeNEYSSA KIMEE SAINT VILNo ratings yet
- Pulmonary Hypertension in Heart Failure With Preserved Ejection FractionDocument9 pagesPulmonary Hypertension in Heart Failure With Preserved Ejection FractiondidiNo ratings yet
- Pathophysiology and Clinical Evaluation of Acute Heart FailureDocument8 pagesPathophysiology and Clinical Evaluation of Acute Heart FailurenicolasNo ratings yet
- Anemia in Heart Failure: Pathophysiology, Pathogenesis, Treatment, and IncognitaeDocument13 pagesAnemia in Heart Failure: Pathophysiology, Pathogenesis, Treatment, and IncognitaeHedya Nadhrati SururaNo ratings yet
- Vasopresores en Choque Séptico 2007Document12 pagesVasopresores en Choque Séptico 2007YESSICA CARENALGANo ratings yet
- Inotropic and Vasoactive Drugs in Pediatric ICUDocument6 pagesInotropic and Vasoactive Drugs in Pediatric ICUCandy RevolloNo ratings yet
- Diuretics in Heart Failure GuidelinesDocument8 pagesDiuretics in Heart Failure GuidelinesMihai CebotariNo ratings yet
- Heart Failure and Atrial Fibrillation: New Concepts in Pathophysiology, Management, and Future DirectionsDocument10 pagesHeart Failure and Atrial Fibrillation: New Concepts in Pathophysiology, Management, and Future Directionsdr_antonio81No ratings yet
- Nefropatia Congestiva 21Document21 pagesNefropatia Congestiva 21John Wesley BragaNo ratings yet
- Patofizyoloji Based Management of PPHTDocument20 pagesPatofizyoloji Based Management of PPHTFunda TüzünNo ratings yet
- Heart Failure in EDDocument17 pagesHeart Failure in EDJean Pierre FakhouryNo ratings yet
- Hypotension in Cirrhosis: ReviewDocument5 pagesHypotension in Cirrhosis: ReviewKarl Martin PinedaNo ratings yet
- Referat Dysfunction Diastolic and Implication in AnathesiaDocument32 pagesReferat Dysfunction Diastolic and Implication in AnathesiaRia Raissa FalaNo ratings yet
- Anesthesia For Non Cardiac Surgery in Children With Congenital Heart DiseaseDocument3 pagesAnesthesia For Non Cardiac Surgery in Children With Congenital Heart Diseasevenkatesh chowdaryNo ratings yet
- Heart Failure - ReferatDocument10 pagesHeart Failure - ReferatAlbert ShantoNo ratings yet
- Fluid Managemnet-HfDocument16 pagesFluid Managemnet-HfAri Dwi PrasetyoNo ratings yet
- Meghan E.Document11 pagesMeghan E.Dr. Jatin GargNo ratings yet
- ES-Eisenmenger Syndrome - Not Always Inoperable. HuangDocument8 pagesES-Eisenmenger Syndrome - Not Always Inoperable. HuangRamaNo ratings yet
- Acute Heart FailureDocument24 pagesAcute Heart FailureTeddy MauriceNo ratings yet
- Hyponatremia Pathophysiology Impact and ManagementDocument5 pagesHyponatremia Pathophysiology Impact and ManagementREMAN ALINGASANo ratings yet
- CFR D-Elia WEBDocument9 pagesCFR D-Elia WEBLuis Rafael Suárez U.No ratings yet
- Intradialitic HypotensionDocument7 pagesIntradialitic HypotensionanitaNo ratings yet
- Congestive Nephropathy: A Neglected Entity? Proposal For Diagnostic Criteria and Future PerspectivesDocument21 pagesCongestive Nephropathy: A Neglected Entity? Proposal For Diagnostic Criteria and Future PerspectivesMuhammad SyammNo ratings yet
- ICCFEP, TX Farmacologico No Farmacologico, 2021Document20 pagesICCFEP, TX Farmacologico No Farmacologico, 2021GeovannaHGNo ratings yet
- Acute Heart Failure in Elderly Patients: A Review of Invasive and Non-Invasive ManagementDocument17 pagesAcute Heart Failure in Elderly Patients: A Review of Invasive and Non-Invasive ManagementErika A. Rodriguez JaureguiNo ratings yet
- Mechanisms, Clinical Implications, and Treatment of Intradialytic HypotensionDocument7 pagesMechanisms, Clinical Implications, and Treatment of Intradialytic Hypotensionhemer hadyn calderon alvitesNo ratings yet
- Pathogenesis and Clinical Presentation of Acute Heart FailureDocument7 pagesPathogenesis and Clinical Presentation of Acute Heart FailureNICOLAS ESTEBAN PARDO DIAZNo ratings yet
- Pathophysiology Diagnosis and Treatment of Orthostatic Hypotension and Vasovagal Syncope1Document17 pagesPathophysiology Diagnosis and Treatment of Orthostatic Hypotension and Vasovagal Syncope1Idha ANo ratings yet
- AFib in ICUDocument11 pagesAFib in ICUvarunNo ratings yet
- Pathophysiologyof Advancedheartfailure: What Knowledge Is Needed For Clinical Management?Document13 pagesPathophysiologyof Advancedheartfailure: What Knowledge Is Needed For Clinical Management?Carlos Hernan Castañeda RuizNo ratings yet
- Ebp 8 72 PDFDocument10 pagesEbp 8 72 PDFMelati HasnailNo ratings yet
- Anemic Heart Disease (Hellenic Journal of Cardiology) 2005Document4 pagesAnemic Heart Disease (Hellenic Journal of Cardiology) 2005abinadivegaNo ratings yet
- Liver International - 2017 - M Ller - The Pathophysiology of Arterial Vasodilatation and Hyperdynamic Circulation inDocument11 pagesLiver International - 2017 - M Ller - The Pathophysiology of Arterial Vasodilatation and Hyperdynamic Circulation inVero GiraldoNo ratings yet
- Fluid Management Strategies in Heart Failure PDFDocument16 pagesFluid Management Strategies in Heart Failure PDFFandy Hazzy AlfataNo ratings yet
- Nihms 1813067Document34 pagesNihms 1813067Marlyn SuciningtiasNo ratings yet
- JPM 13 00140 v2Document17 pagesJPM 13 00140 v2YeseniaNo ratings yet
- 10 1016@j Anclin 2020 08 004Document11 pages10 1016@j Anclin 2020 08 004Luis David Gárate CastañedaNo ratings yet
- Prevalence of Anemia in Patients With Heart Failure: Edition: 29.1 - 12 Article(s)Document13 pagesPrevalence of Anemia in Patients With Heart Failure: Edition: 29.1 - 12 Article(s)Novia KurniantiNo ratings yet
- Pulmonary Hypertension and SclerodermaDocument6 pagesPulmonary Hypertension and SclerodermaManuel MendezNo ratings yet
- European J of Heart Fail - 2023 - Gustafsson - Inotropic Therapy in Patients With Advanced Heart Failure A ClinicalDocument12 pagesEuropean J of Heart Fail - 2023 - Gustafsson - Inotropic Therapy in Patients With Advanced Heart Failure A ClinicalFerBullknockNo ratings yet
- Heart Failure With Preserved Ejection Fraction: Controversies, Challenges and Future DirectionsDocument9 pagesHeart Failure With Preserved Ejection Fraction: Controversies, Challenges and Future DirectionsOngky AristianNo ratings yet
- Heart Failure in Adult Congenital Heart Disease Nonpharmacologic Treatment StrategiesDocument10 pagesHeart Failure in Adult Congenital Heart Disease Nonpharmacologic Treatment StrategiesAndhika DNo ratings yet
- Pulmonary Hypertension: Annals of Internal MedicinetDocument16 pagesPulmonary Hypertension: Annals of Internal MedicinetAlicia TGNo ratings yet
- Chronic Heart Failure-Part IDocument18 pagesChronic Heart Failure-Part IdrtpkNo ratings yet
- Inotrópicos en ICC Avanzada DRUGS 2011 PDFDocument11 pagesInotrópicos en ICC Avanzada DRUGS 2011 PDFCsr ArsNo ratings yet
- Updates in Cardiorenal SyndromeDocument18 pagesUpdates in Cardiorenal SyndromeSaulVillaseñorNo ratings yet
- Fibrliación Auricular en Falla Cardiaca, Qué Debemos de Hacer ESC 2015Document11 pagesFibrliación Auricular en Falla Cardiaca, Qué Debemos de Hacer ESC 2015alanRV12No ratings yet
- Beyond Mean Arterial Pressure and Lactate Perfusion End Points For Managing The Shocked PatientDocument14 pagesBeyond Mean Arterial Pressure and Lactate Perfusion End Points For Managing The Shocked PatientLuis Miguel VillanuevaNo ratings yet
- Posterior Reversible Encephalopathy SyndromeDocument9 pagesPosterior Reversible Encephalopathy SyndromejuanmontoyaseNo ratings yet
- Evaluation and Management of Hyponatremia in Heart Failure: Giulio M. Mondellini Frederik H. VerbruggeDocument10 pagesEvaluation and Management of Hyponatremia in Heart Failure: Giulio M. Mondellini Frederik H. VerbruggeHugo EspinozaNo ratings yet
- Diabetic CardiomyopathyDocument7 pagesDiabetic Cardiomyopathyakbar011512No ratings yet
- Dengue Haemorrhagic FeverDocument5 pagesDengue Haemorrhagic FeverYS NateNo ratings yet
- Clinical Cases in Chronic Thromboembolic Pulmonary HypertensionFrom EverandClinical Cases in Chronic Thromboembolic Pulmonary HypertensionWilliam R. AugerNo ratings yet
- Cia 10 287Document9 pagesCia 10 287al jaynNo ratings yet
- Environment, Human Reproduction, Menopause, and Andropause: by Alex VermeulenDocument10 pagesEnvironment, Human Reproduction, Menopause, and Andropause: by Alex Vermeulenal jaynNo ratings yet
- Plastic Waste: Ecological and Human Health Impacts November 2011Document52 pagesPlastic Waste: Ecological and Human Health Impacts November 2011al jaynNo ratings yet
- Clinicopathologic Features of Agranulocytosis in The Setting of Levamisole-Tainted CocaineDocument7 pagesClinicopathologic Features of Agranulocytosis in The Setting of Levamisole-Tainted Cocaineal jaynNo ratings yet
- NannsDocument9 pagesNannsal jaynNo ratings yet
- Infectious Diseases & TherapyDocument6 pagesInfectious Diseases & Therapyal jaynNo ratings yet
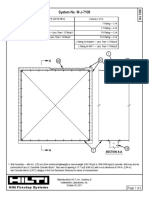
- Ul Fs On Max Rectangular Duct Block WallDocument2 pagesUl Fs On Max Rectangular Duct Block WallhossamNo ratings yet
- Aditya Hrudaya SthotramDocument8 pagesAditya Hrudaya SthotramRajiv Warrier100% (1)
- Daytona Lifestyle LP111 ProgrammersDocument2 pagesDaytona Lifestyle LP111 ProgrammersJohn WalesNo ratings yet
- Management Companies Are, However, A Relatively Novel Concept in Terms of Centuries. The Early YearsDocument7 pagesManagement Companies Are, However, A Relatively Novel Concept in Terms of Centuries. The Early Yearsmaria cristina pascualNo ratings yet
- Answer Key - Employee Benefits PDFDocument3 pagesAnswer Key - Employee Benefits PDFglobeth berbanoNo ratings yet
- NCVPS Honors Chemistry M2L4N1 Guided NotesDocument7 pagesNCVPS Honors Chemistry M2L4N1 Guided NotesTydenNo ratings yet
- Acfrogbdptmf56s1siyxu2og1 J8mpghw0xmlmenslfrleoetc66rt7stitnmyxvnbbl2rccbikgrlrtllqdlnljwt6y Adokixllnd6 Rj1cjewjiie7ee4ol1muvu0jof N6vysa79et2lzln7Document5 pagesAcfrogbdptmf56s1siyxu2og1 J8mpghw0xmlmenslfrleoetc66rt7stitnmyxvnbbl2rccbikgrlrtllqdlnljwt6y Adokixllnd6 Rj1cjewjiie7ee4ol1muvu0jof N6vysa79et2lzln7Komang Indra Kurnia TriatmajaNo ratings yet
- Chapter 37 Fire Detection, Protection and Suppression SystemsDocument4 pagesChapter 37 Fire Detection, Protection and Suppression SystemsDanny Dukeran100% (1)
- Peter Paul CatalogDocument112 pagesPeter Paul Catalogcristian cendejasNo ratings yet
- TNSOP 5.0 Infection Prevention Control at Various Levels PDFDocument1 pageTNSOP 5.0 Infection Prevention Control at Various Levels PDFSridhar KrishnamurthiNo ratings yet
- Pengantar Anatomi NBSDocument65 pagesPengantar Anatomi NBSHa HaNo ratings yet
- Wa0000Document16 pagesWa0000dasakshyat098No ratings yet
- Yearii 1Document1 pageYearii 1chaos4everNo ratings yet
- Analysis and Prevention of Bearing FailuresDocument76 pagesAnalysis and Prevention of Bearing Failurestahazeeshan100% (1)
- Immunology Lecture 03 - Antibodies Part 1 - 2018Document36 pagesImmunology Lecture 03 - Antibodies Part 1 - 2018api-273068056No ratings yet
- Project Report On Nokia Vs SamsungDocument72 pagesProject Report On Nokia Vs SamsungMahesh Dua71% (21)
- Tegumenta Si Parti MoiDocument8 pagesTegumenta Si Parti MoiCiorescu AlinaNo ratings yet
- Elisa TestDocument11 pagesElisa Testtofan widyaNo ratings yet
- Sohagi Barwa Wildlife SanctuaryDocument21 pagesSohagi Barwa Wildlife SanctuaryRachanaNo ratings yet
- SUN2000 - 215KTL-H0 - DatasheetDocument2 pagesSUN2000 - 215KTL-H0 - DatasheetCamila 4SENo ratings yet
- Accelerated Academic Calendar Grades XI-XII 2020-21Document109 pagesAccelerated Academic Calendar Grades XI-XII 2020-21Madiha BabarNo ratings yet
- GEN - Instrument List (2014 - 08 - 09 13 - 13 - 18 UTC) PDFDocument11 pagesGEN - Instrument List (2014 - 08 - 09 13 - 13 - 18 UTC) PDFVinoth KumarNo ratings yet
- Bangkok Trip PlanDocument5 pagesBangkok Trip PlanKim Hong LYNo ratings yet
- Murphy S Bagel Shops Is A Chain of Bagel Eateries SupportedDocument1 pageMurphy S Bagel Shops Is A Chain of Bagel Eateries SupportedAmit PandeyNo ratings yet
- Group - Koko Be AssignmentDocument10 pagesGroup - Koko Be AssignmentThink BigNo ratings yet
- TORO Filter Press ManualDocument12 pagesTORO Filter Press ManualRamkiNo ratings yet
- Astrology NotebookDocument88 pagesAstrology NotebookCésar Antonio González Urbaneja0% (1)
- Feeding CowDocument8 pagesFeeding CowGigiPetreaNo ratings yet
- Ot SluiceDocument3 pagesOt Sluicegurumurthy38No ratings yet