You might also like
- Intermittent ExotropiaDocument15 pagesIntermittent ExotropiakarenafiafiNo ratings yet
- Environmental Risk Factors For Multiple Sclerosis. Part II: Noninfectious FactorsDocument10 pagesEnvironmental Risk Factors For Multiple Sclerosis. Part II: Noninfectious FactorsGerry SanjayaNo ratings yet
- Risk Factors of Multiple Sclerosis: A Case-Control StudyDocument6 pagesRisk Factors of Multiple Sclerosis: A Case-Control StudyGerry SanjayaNo ratings yet
- The Role of Disease and Demographic Factors in The Employment of Patients With Multiple SclerosisDocument12 pagesThe Role of Disease and Demographic Factors in The Employment of Patients With Multiple SclerosisGerry SanjayaNo ratings yet
- 1 s2.0 S2213058614000096 Main PDFDocument8 pages1 s2.0 S2213058614000096 Main PDFMadalina VladNo ratings yet
- DHF Menurut WHO 2011Document212 pagesDHF Menurut WHO 2011Jamal SutrisnaNo ratings yet
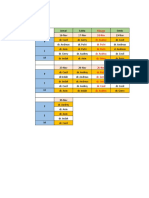
- Jadwal Isip November Fixed BangetttttttDocument3 pagesJadwal Isip November Fixed BangetttttttGerry SanjayaNo ratings yet
- Jadwal Manual PKCDocument5 pagesJadwal Manual PKCGerry SanjayaNo ratings yet
- Reviews: Environmental Factors and Their Timing in Adult-Onset Multiple SclerosisDocument11 pagesReviews: Environmental Factors and Their Timing in Adult-Onset Multiple SclerosisGerry SanjayaNo ratings yet
- Jadwal Promkes PKLDocument5 pagesJadwal Promkes PKLGerry SanjayaNo ratings yet
- Journal 2Document10 pagesJournal 2Gerry SanjayaNo ratings yet
- Jadwal Manual PKCDocument5 pagesJadwal Manual PKCGerry SanjayaNo ratings yet
- G PTL PDFDocument26 pagesG PTL PDFGerry SanjayaNo ratings yet
- Coronary Artery Anatomy ReviewDocument6 pagesCoronary Artery Anatomy ReviewGerry SanjayaNo ratings yet
- Aafp Pprom PDFDocument6 pagesAafp Pprom PDFGerry SanjayaNo ratings yet
- 356 1732 1 PB PDFDocument12 pages356 1732 1 PB PDFGerry SanjayaNo ratings yet
- Intermittent ExotropiaDocument15 pagesIntermittent ExotropiakarenafiafiNo ratings yet
- 356 1732 1 PB PDFDocument12 pages356 1732 1 PB PDFGerry SanjayaNo ratings yet
- Jadwal Sunday Market Obsgyn: Senin 14/8/17 Selasa 15/8/17 Rabu 16/8/17 Jumat 18/8/17 Sabtu 19/8/17Document8 pagesJadwal Sunday Market Obsgyn: Senin 14/8/17 Selasa 15/8/17 Rabu 16/8/17 Jumat 18/8/17 Sabtu 19/8/17Gerry SanjayaNo ratings yet
- Preterm Labour and Birth: Maternity and Neonatal Clinical GuidelineDocument26 pagesPreterm Labour and Birth: Maternity and Neonatal Clinical GuidelineGerry SanjayaNo ratings yet
- AIP Chap15 Preterm Labour Preterm Birth PDFDocument9 pagesAIP Chap15 Preterm Labour Preterm Birth PDFGerry SanjayaNo ratings yet
- 2046 4745 2 PBDocument4 pages2046 4745 2 PBGerry SanjayaNo ratings yet
- Wa0000Document7 pagesWa0000Gerry SanjayaNo ratings yet
- Strabismus: - Symptoms, Pathophysiology, Management & PrecautionsDocument5 pagesStrabismus: - Symptoms, Pathophysiology, Management & PrecautionsGerry SanjayaNo ratings yet
- Nutrisi Klinis Journal Provides Guidelines on Clinical Nutrition in SurgeryDocument31 pagesNutrisi Klinis Journal Provides Guidelines on Clinical Nutrition in SurgeryGerry SanjayaNo ratings yet
- 08Document4 pages08Gerry SanjayaNo ratings yet
- PDFDocument6 pagesPDFArdianSyah PtrNo ratings yet
- Case Report DewiDocument2 pagesCase Report DewiGerry SanjayaNo ratings yet
- 05 - 195drug Use in Patients With Renal Failure PDFDocument5 pages05 - 195drug Use in Patients With Renal Failure PDFGerry SanjayaNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Chemotherapy and Biotherapeutic Agents For Autoimmune DiseasesDocument17 pagesChemotherapy and Biotherapeutic Agents For Autoimmune DiseasesIriani Dewi SetiawanNo ratings yet
- Multiple SclerosisDocument10 pagesMultiple Sclerosisrazan asadNo ratings yet
- Multiple Sclerosis Nursing Care PlanDocument4 pagesMultiple Sclerosis Nursing Care PlanCHRISTIE MONTANONo ratings yet
- Action Potential - The Resting Membrane Potential - Generation of Action Potentials - TeachMePhysiologAyDocument4 pagesAction Potential - The Resting Membrane Potential - Generation of Action Potentials - TeachMePhysiologAymohammed awolNo ratings yet
- Multiple SclerosisDocument3 pagesMultiple SclerosisCarmella CollantesNo ratings yet
- Multiple SclerosisDocument204 pagesMultiple SclerosisOctavian Babcinschi100% (1)
- A Guide For Patients and Physicians: The Washington State Medical Marijuana ActDocument4 pagesA Guide For Patients and Physicians: The Washington State Medical Marijuana Actelioom100% (2)
- IELTS Practice Test Answer KeysDocument4 pagesIELTS Practice Test Answer Keysfikri fikriNo ratings yet
- Treating Yourself Magazine #19Document132 pagesTreating Yourself Magazine #19murciano207100% (4)
- FULL-TEXT - NCLEX-RN Practice Quiz Test Bank 3 - NurseslabsDocument91 pagesFULL-TEXT - NCLEX-RN Practice Quiz Test Bank 3 - NurseslabsRonaldo Matos PerezNo ratings yet
- A Case Study of Multiple Sclerosis (MS)Document31 pagesA Case Study of Multiple Sclerosis (MS)william2young-136543No ratings yet
- Charles Barker Patent: Copper I Vto Heal Lyme's Disease - Video, PatentsDocument20 pagesCharles Barker Patent: Copper I Vto Heal Lyme's Disease - Video, Patentssmart_chrisNo ratings yet
- LDN Fact Sheet Provides Dosing and Mechanism DetailsDocument8 pagesLDN Fact Sheet Provides Dosing and Mechanism DetailscristiNo ratings yet
- JCN 14 487Document5 pagesJCN 14 487Yanny LabokNo ratings yet
- A Complex Relation Between Depression and Multiple Sclerosis: A Descriptive ReviewDocument8 pagesA Complex Relation Between Depression and Multiple Sclerosis: A Descriptive ReviewGilvan ValdevinoNo ratings yet
- His 5Document167 pagesHis 5Anjum100% (5)
- MS DiseaseDocument2 pagesMS Diseasesundareswar perumalNo ratings yet
- Zapper DigitalDocument9 pagesZapper DigitalolopezNo ratings yet
- Vol 28.4 - Multiple Sclerosis and Related Disorders.2022Document295 pagesVol 28.4 - Multiple Sclerosis and Related Disorders.2022Cibele100% (1)
- # Davidson - Review # Neurology - 1Document42 pages# Davidson - Review # Neurology - 1emtiaz zamanNo ratings yet
- Yoga For Neurogenic Bladder PDFDocument7 pagesYoga For Neurogenic Bladder PDFsg3569No ratings yet
- 6 Birth DefectsDocument40 pages6 Birth DefectsjulieNo ratings yet
- Multiple Sclerosis Society of Canada - London-Grand Bend Bicycle TourDocument6 pagesMultiple Sclerosis Society of Canada - London-Grand Bend Bicycle TourUjjwal Gahlot100% (1)
- Newsletter v5n2Document92 pagesNewsletter v5n2Transverse Myelitis AssociationNo ratings yet
- Article MSQOL-54Document21 pagesArticle MSQOL-54bogdanneamtuNo ratings yet
- Acquired Demyelinating SyndromesDocument13 pagesAcquired Demyelinating SyndromesfbonillaNo ratings yet
- Multiple SclerosisDocument6 pagesMultiple SclerosisMBENOYNo ratings yet
- Upper Motor Neuron DiseasesDocument7 pagesUpper Motor Neuron DiseasesRyl WonNo ratings yet
- Spinal Cord Anatomy and DiseasesDocument37 pagesSpinal Cord Anatomy and DiseasesDek SriNo ratings yet
- Transverse Myelitis - UpToDateDocument27 pagesTransverse Myelitis - UpToDateFabiola Javiera Reales NúñezNo ratings yet