You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (844)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5810)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (346)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Human Body WorkbookDocument25 pagesHuman Body Workbookjk centralNo ratings yet
- Hypertensive Heart DiseasesDocument5 pagesHypertensive Heart DiseasesserubimNo ratings yet
- Disorders of The Thyroid and Parathyroid Glands: Ms TeamDocument36 pagesDisorders of The Thyroid and Parathyroid Glands: Ms TeamShy Dela PuertaNo ratings yet
- Usmle QDocument46 pagesUsmle QRoh Jiten100% (1)
- Lower Extremity Arterial Protocol 14 1Document2 pagesLower Extremity Arterial Protocol 14 1api-3494022400% (1)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Waveform Questions /critical Care Board ReviewDocument14 pagesWaveform Questions /critical Care Board ReviewAzmachamberAzmacare100% (1)
- Anxiolytic and Hypnotic DrugsDocument27 pagesAnxiolytic and Hypnotic DrugsEjaj SumitNo ratings yet
- Framingham Risk Score SaDocument8 pagesFramingham Risk Score Saapi-301624030No ratings yet
- Gaseous SterilizationDocument12 pagesGaseous SterilizationEjaj SumitNo ratings yet
- Eto SterilizationDocument9 pagesEto SterilizationEjaj SumitNo ratings yet
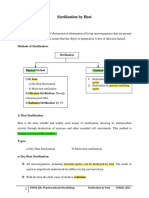
- Sterilization by HeatDocument8 pagesSterilization by HeatEjaj SumitNo ratings yet
- Sterilization by RadiationDocument11 pagesSterilization by RadiationEjaj SumitNo ratings yet
- Aseptic Processing: Sterilization by FiltrationDocument10 pagesAseptic Processing: Sterilization by FiltrationEjaj SumitNo ratings yet
- Diuretics: PHRM 306: Drugs Affecting CVSDocument51 pagesDiuretics: PHRM 306: Drugs Affecting CVSEjaj SumitNo ratings yet
- Checklist For Local Anesthetic Toxicity Treatment 1-18-12Document2 pagesChecklist For Local Anesthetic Toxicity Treatment 1-18-12Akilesh RamasamyNo ratings yet
- Lactated Ringer'sDocument10 pagesLactated Ringer'sJeannette Richelle DacilloNo ratings yet
- FBOA-Etiology and Clinical FeaturesDocument8 pagesFBOA-Etiology and Clinical FeaturesKuchh BhiiNo ratings yet
- Guidelines Made Simple Chest PainDocument18 pagesGuidelines Made Simple Chest PainPaul JohnNo ratings yet
- HyperlipidemiaDocument38 pagesHyperlipidemiaAadhan ArveeNo ratings yet
- Management of Thoracic Aortic DissectionDocument2 pagesManagement of Thoracic Aortic DissectionKarina ResendeNo ratings yet
- Rational Clinical Examination - Evidence-Based Clinical DiagnosisDocument11 pagesRational Clinical Examination - Evidence-Based Clinical DiagnosisDanteNo ratings yet
- GP MCQ 2Document4 pagesGP MCQ 2Marta MoreiraNo ratings yet
- Michael W, COMAT PedsDocument17 pagesMichael W, COMAT PedsSeanNo ratings yet
- Topic List Q&ADocument63 pagesTopic List Q&APop D. MadalinaNo ratings yet
- Cardioversion and DefibDocument16 pagesCardioversion and DefibSami FreijyNo ratings yet
- Intracranial HypertensionDocument28 pagesIntracranial HypertensionHussein TarhiniNo ratings yet
- The Heart Manual: Post Myocardial Infarction (Post MI) EditionDocument18 pagesThe Heart Manual: Post Myocardial Infarction (Post MI) EditionPablo L RodriguezNo ratings yet
- Defense Against Infectious Disease: Skin As A Barrier To InfectionDocument8 pagesDefense Against Infectious Disease: Skin As A Barrier To InfectionFranchesca Rosabel BudimanNo ratings yet
- Superior MediastinumDocument4 pagesSuperior MediastinumYheng GaosaiiNo ratings yet
- AUBF Gastric AnalysisDocument3 pagesAUBF Gastric AnalysisRichelyn Grace B. VenusNo ratings yet
- Guidelines For The Diagnosis and Treatment of Chronic Heart FailureDocument26 pagesGuidelines For The Diagnosis and Treatment of Chronic Heart FailurecubewormNo ratings yet
- Powerpoint The HeartDocument13 pagesPowerpoint The HeartjavadkollamNo ratings yet
- Pathophysiology ErDocument3 pagesPathophysiology ErAlexa A. AldayNo ratings yet
- Cardiacassessmentppt 170323092148Document48 pagesCardiacassessmentppt 170323092148sasNo ratings yet
- Carp TrialDocument10 pagesCarp TrialIMNo ratings yet
- List of Autoimmune DiseasesDocument11 pagesList of Autoimmune DiseasesDuwa AhmadNo ratings yet
- Cardiovascular Pharmacology OutlineDocument11 pagesCardiovascular Pharmacology OutlineLhay de OcampoNo ratings yet