You might also like
- CCU Clinical GuidelinesDocument63 pagesCCU Clinical GuidelinesHAMMYER ALROKHAMINo ratings yet
- 001 Admission APP MED 001Document7 pages001 Admission APP MED 001HAMMYER ALROKHAMINo ratings yet
- 1-Call Consultant Specialist For Opinions-App-001Document2 pages1-Call Consultant Specialist For Opinions-App-001HAMMYER ALROKHAMINo ratings yet
- 17 Admission APP MED 001Document8 pages17 Admission APP MED 001HAMMYER ALROKHAMINo ratings yet
- SFMC-AnesthesiabPolicies and Procedures (2017)Document77 pagesSFMC-AnesthesiabPolicies and Procedures (2017)HAMMYER ALROKHAMINo ratings yet
- 2019 Policy Manual 20190812Document88 pages2019 Policy Manual 20190812HAMMYER ALROKHAMINo ratings yet
- The Washington Manual of Critical Care - 2nd Edition Export - En.arDocument2 pagesThe Washington Manual of Critical Care - 2nd Edition Export - En.arHAMMYER ALROKHAMINo ratings yet
- Chest Physiotherapy For Patients Admitted To Hospital With An Acute Exacerbation of Chronic Obstructive Pulmonary Disease (COPD)Document13 pagesChest Physiotherapy For Patients Admitted To Hospital With An Acute Exacerbation of Chronic Obstructive Pulmonary Disease (COPD)HAMMYER ALROKHAMINo ratings yet
- Physiotherapy - Breath Stacking TechniqueDocument3 pagesPhysiotherapy - Breath Stacking TechniqueHAMMYER ALROKHAMINo ratings yet
- EHDN Physio Guide1Document11 pagesEHDN Physio Guide1HAMMYER ALROKHAMINo ratings yet
- Acid Base BalaneceDocument11 pagesAcid Base BalaneceHAMMYER ALROKHAMINo ratings yet
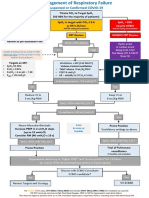
- Suspected or Confirmed Covid-19: Spo 92% Despite NRBM Urgent CRT Review WardDocument1 pageSuspected or Confirmed Covid-19: Spo 92% Despite NRBM Urgent CRT Review WardHAMMYER ALROKHAMINo ratings yet
- Cardiovascular & Pulmonary Physiotherapy - WikipediaDocument13 pagesCardiovascular & Pulmonary Physiotherapy - WikipediaHAMMYER ALROKHAMINo ratings yet
- Ret Clinical HandbookDocument89 pagesRet Clinical HandbookHAMMYER ALROKHAMINo ratings yet
- Acid Base PhysiologyDocument1 pageAcid Base PhysiologyHAMMYER ALROKHAMINo ratings yet
- ABG Interpretation - ATSDocument5 pagesABG Interpretation - ATSHAMMYER ALROKHAMINo ratings yet
- Physiotherapy in Respiratory MedicineDocument8 pagesPhysiotherapy in Respiratory MedicineHAMMYER ALROKHAMINo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5795)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Inhalation Injury From Heat, Smoke, or Chemical IrritantsDocument29 pagesInhalation Injury From Heat, Smoke, or Chemical IrritantsJulian SalazarNo ratings yet
- Respiratory Symptoms and Signs: Key PointsDocument9 pagesRespiratory Symptoms and Signs: Key PointsAna LopezNo ratings yet
- NCP BaiaeDocument7 pagesNCP BaiaeJonathan Delos ReyesNo ratings yet
- High Flow Nasal Cannula Versus Continuous Positive Airway PressureDocument13 pagesHigh Flow Nasal Cannula Versus Continuous Positive Airway PressurefitriNo ratings yet
- Nursing Care PlanDocument3 pagesNursing Care PlanMarielle SorianoNo ratings yet
- Edited Final ProjectDocument67 pagesEdited Final ProjectIbsa GetachoNo ratings yet
- Mechanical Ventilation 101: DR Paul Healey ICU Fellow John Hunter Hospital NewcastleDocument95 pagesMechanical Ventilation 101: DR Paul Healey ICU Fellow John Hunter Hospital NewcastlePatrick ValentinoNo ratings yet
- Chest Trauma3Document120 pagesChest Trauma3Rojelle LezamaNo ratings yet
- Chest Physiotherapy in Paediatric Patients Hospitalised With Community-Acquired Pneumonia: A Randomised Clinical TrialDocument7 pagesChest Physiotherapy in Paediatric Patients Hospitalised With Community-Acquired Pneumonia: A Randomised Clinical Trialaufa memeyNo ratings yet
- Mechanical VentilationDocument42 pagesMechanical VentilationWiz SamNo ratings yet
- Carefusion CircuitsDocument20 pagesCarefusion Circuitsrubenr25No ratings yet
- 1 - Spirometry Simplified With CRF's PEFR PDFDocument80 pages1 - Spirometry Simplified With CRF's PEFR PDFyayatiNo ratings yet
- Guideline On The Management of AsthmaDocument151 pagesGuideline On The Management of AsthmaJohn HolmesNo ratings yet
- Acute Respiratory Distress Syndrome: South Tipperary General Hospital Emergency DepartmentDocument17 pagesAcute Respiratory Distress Syndrome: South Tipperary General Hospital Emergency DepartmentRoya FarooqNo ratings yet
- What Are The Respiratory Causes of Clubbing?Document8 pagesWhat Are The Respiratory Causes of Clubbing?Ahmed NazarNo ratings yet
- HAMILTON C2 Technical SpecificationsDocument4 pagesHAMILTON C2 Technical SpecificationsZarghamKhanNo ratings yet
- Advanced Trauma Life SupportDocument8 pagesAdvanced Trauma Life SupportazlanajaibNo ratings yet
- Spesifikasi Draeger Evita V300Document3 pagesSpesifikasi Draeger Evita V300yusrimurahNo ratings yet
- SuctioningDocument24 pagesSuctioningLanz LlnsNo ratings yet
- Lesson Plan VentilatorDocument25 pagesLesson Plan VentilatorLoma Waghmare (Jadhav)100% (1)
- Mucus Color Guidee BookDocument9 pagesMucus Color Guidee BookRyn ShadowNo ratings yet
- Spirometry in Primary Care: DR Max Matonhodze FRCP (London) M A Med Ed (Keele)Document60 pagesSpirometry in Primary Care: DR Max Matonhodze FRCP (London) M A Med Ed (Keele)Alkaustariyah LubisNo ratings yet
- Shortness of Breath: Checklist PMPF Checklist PMPFDocument1 pageShortness of Breath: Checklist PMPF Checklist PMPFanz_4191No ratings yet
- Respiratory Case StudiesDocument6 pagesRespiratory Case Studiesadom09No ratings yet
- 02-02-2023 Yasir PDFDocument12 pages02-02-2023 Yasir PDFNASER HUSSAIN SHAHNo ratings yet
- Oxygen Insufficiency: Presented byDocument66 pagesOxygen Insufficiency: Presented byHardeep KaurNo ratings yet
- Anaesthesia in Asthmatic (Read)Document39 pagesAnaesthesia in Asthmatic (Read)Parvathy R NairNo ratings yet
- Principles of Chest Physiotherapy in ICUDocument42 pagesPrinciples of Chest Physiotherapy in ICUKapil Lakhwara100% (3)
- V60 Pocket GuideDocument20 pagesV60 Pocket GuideJohnny CotzitoNo ratings yet
- NCP - Impaired Gas Exchange (COPD)Document3 pagesNCP - Impaired Gas Exchange (COPD)Karen Joy ItoNo ratings yet