You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (842)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5806)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- 1.psychiatric Neuroscience - Incorporating Pathophysiology Into Clinical Case Formulation - ClinicalKeyDocument43 pages1.psychiatric Neuroscience - Incorporating Pathophysiology Into Clinical Case Formulation - ClinicalKeyClaudia0% (1)
- Rescue and Carry Methods Power PointDocument75 pagesRescue and Carry Methods Power PointJean Minette Prado88% (8)
- Trauma Focused CBT ArticleDocument14 pagesTrauma Focused CBT ArticleClaudiaNo ratings yet
- Intrahepatic Cholestasis of Pregnancy: Clinical Obstetrics and Gynecology Volume 63, Number 1, 134-151Document19 pagesIntrahepatic Cholestasis of Pregnancy: Clinical Obstetrics and Gynecology Volume 63, Number 1, 134-151Von BernalNo ratings yet
- Pharmacology of AntimycobacterialDocument7 pagesPharmacology of Antimycobacterialselflessdoctor100% (1)
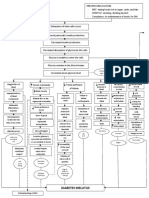
- Diabetes Mellitus: Hyperglycemia (304 MG/DL, 13.2 MG/DL)Document3 pagesDiabetes Mellitus: Hyperglycemia (304 MG/DL, 13.2 MG/DL)John Henry ValenciaNo ratings yet
- Buteyko Manual PDFDocument130 pagesButeyko Manual PDFPauloCarvalho92% (12)
- Pathophysiology HemothoraxDocument1 pagePathophysiology HemothoraxFlauros Ryu Jabien50% (4)
- Maxwell's Manual of Malicious MaladiesDocument35 pagesMaxwell's Manual of Malicious MaladiesJean Ariehn100% (1)
- Impacts of Drugs On Neurotransmission - National Institute On Drug Abuse (NIDA)Document16 pagesImpacts of Drugs On Neurotransmission - National Institute On Drug Abuse (NIDA)ClaudiaNo ratings yet
- Child Abuse and NeglectDocument17 pagesChild Abuse and NeglectClaudiaNo ratings yet
- Recognizing Child Abuse: What Parents Should KnowDocument4 pagesRecognizing Child Abuse: What Parents Should KnowClaudiaNo ratings yet
- Violencia Rueda de Poder y ControlDocument1 pageViolencia Rueda de Poder y ControlClaudiaNo ratings yet
- Lecture 5Document3 pagesLecture 5Shakil MahmodNo ratings yet
- Passive Somking: G Hrithik Roger Kumar Reg No 20BLB1089Document12 pagesPassive Somking: G Hrithik Roger Kumar Reg No 20BLB1089Sathyanarayanan KalyanasundaramNo ratings yet
- Indranila 2021Document22 pagesIndranila 2021reski utamiNo ratings yet
- News Bulletin Script TemplateDocument2 pagesNews Bulletin Script TemplateSantisha Chattergoon100% (3)
- Youth ItumelengDocument18 pagesYouth ItumelengKeneilwe CalistusNo ratings yet
- Health Sector Reform in IndiaDocument21 pagesHealth Sector Reform in Indiajouhar21No ratings yet
- Review Article: Investigation On Cardiovascular Risk Prediction Using Physiological ParametersDocument22 pagesReview Article: Investigation On Cardiovascular Risk Prediction Using Physiological ParametersNnaemeka NwobodoNo ratings yet
- MovicolDocument2 pagesMovicolreadalotbutnowisdomyetNo ratings yet
- EHSS PLAN - Petrokemya - ABS PlantDocument44 pagesEHSS PLAN - Petrokemya - ABS PlantOvais FarooqNo ratings yet
- GREENLEAFDocument5 pagesGREENLEAF-Cabinet de traduction NETWORDTNo ratings yet
- Hypertensive Disorders in Pregnancy: Abdallah Al-MawazrehDocument36 pagesHypertensive Disorders in Pregnancy: Abdallah Al-MawazrehAbdallahMousaNo ratings yet
- Seoul - Contagion of CausalityDocument28 pagesSeoul - Contagion of CausalityJason ItalianoNo ratings yet
- Managing Safety and HealthDocument40 pagesManaging Safety and HealthFairooz RaisaNo ratings yet
- Public Health Competencies HandbookDocument33 pagesPublic Health Competencies Handbookapi-556450573No ratings yet
- Challenging Neurological Manifestations in Large Cell Neuroendocrine Carcinoma Lcnec A Case Study of Extensive Intracranial and Intradural MetastasesDocument3 pagesChallenging Neurological Manifestations in Large Cell Neuroendocrine Carcinoma Lcnec A Case Study of Extensive Intracranial and Intradural MetastasesHerald Scholarly Open AccessNo ratings yet
- 04 Huang v. Philippine Hoteliers, Inc, G.R. No. 180440, 5 December 2012Document15 pages04 Huang v. Philippine Hoteliers, Inc, G.R. No. 180440, 5 December 2012Andrei Da JoseNo ratings yet
- Coping With Diabetes-Denial, AngerDocument13 pagesCoping With Diabetes-Denial, AngerShwetal ShindeNo ratings yet
- Nremt Study GuideDocument20 pagesNremt Study GuideKhaled AltaherNo ratings yet
- EASD2021-Final Programme LowresDocument304 pagesEASD2021-Final Programme LowresMajeedNo ratings yet
- Association of The MTHFR 677C T Polymorphism With Obesity and Biochemical Variables in A Young Population of MexicoDocument7 pagesAssociation of The MTHFR 677C T Polymorphism With Obesity and Biochemical Variables in A Young Population of MexicoMauro Porcel de PeraltaNo ratings yet
- History of Abnormal Psychology Chap 2Document20 pagesHistory of Abnormal Psychology Chap 2ahmadNo ratings yet
- Rheumatoid Factor FS : Order Information SpecimenDocument3 pagesRheumatoid Factor FS : Order Information SpecimenHadi BitarNo ratings yet
- A Case Study On Occupational Health and Safety of Footwear Manufacturing IndustryDocument6 pagesA Case Study On Occupational Health and Safety of Footwear Manufacturing IndustryZakir KhanNo ratings yet