You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (842)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5806)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- 122 Audio Amplifier ConstructionDocument57 pages122 Audio Amplifier ConstructionsilviaNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- 2018-09-01 Classic Land RoverDocument100 pages2018-09-01 Classic Land RovergufffNo ratings yet
- Operator Manual of Xray GeneratorDocument43 pagesOperator Manual of Xray GeneratorMohamed belhasanNo ratings yet
- Acupuncture Standards China Baoyan 2009Document50 pagesAcupuncture Standards China Baoyan 2009Marlon RamirezNo ratings yet
- Acupuncture Analgesia ResearchDocument27 pagesAcupuncture Analgesia ResearchMarlon RamirezNo ratings yet
- Treatment of Clearing The GovernorDocument5 pagesTreatment of Clearing The GovernorMarlon RamirezNo ratings yet
- Treatment of 36 Cases of Epistaxis With Hydro-Acupuncture at Ear PointsDocument2 pagesTreatment of 36 Cases of Epistaxis With Hydro-Acupuncture at Ear PointsMarlon RamirezNo ratings yet
- Ga110 - Manual de UsuarioDocument118 pagesGa110 - Manual de UsuarioFloydMG TecnominNo ratings yet
- GMMWDocument12 pagesGMMWalvaro valienteNo ratings yet
- Ad 2 Ltac Instrument Approach Chart - Icao Iac 3 - Ils y Cat I Rwy 03RDocument1 pageAd 2 Ltac Instrument Approach Chart - Icao Iac 3 - Ils y Cat I Rwy 03RsaruhanNo ratings yet
- Sphere Comp ManualDocument5 pagesSphere Comp ManualdubmastergNo ratings yet
- Hauser Endress: Capacitance Level Measurement Electronic Inserts EC 37 Z, EC 47 ZDocument8 pagesHauser Endress: Capacitance Level Measurement Electronic Inserts EC 37 Z, EC 47 ZDenisNo ratings yet
- DevopsDocument56 pagesDevopsvidya bvNo ratings yet
- DMCT Unit1 and 2 MCQDocument78 pagesDMCT Unit1 and 2 MCQsNo ratings yet
- Rotel RB-1090 Service ManualDocument10 pagesRotel RB-1090 Service ManualzektorNo ratings yet
- 2.00 Am Report 20 JulyDocument45 pages2.00 Am Report 20 JulyAakarsh VermaNo ratings yet
- Texscan SweepDocument161 pagesTexscan SweepAniello IaccarinoNo ratings yet
- Mobile Communication Technical Seminar DivyaDocument24 pagesMobile Communication Technical Seminar DivyashaikmustaqNo ratings yet
- Rules and Regulations:: First RoundDocument2 pagesRules and Regulations:: First Roundarchana naikNo ratings yet
- Talent Level 3 Revision Unit 1Document1 pageTalent Level 3 Revision Unit 1ana maria csalinas0% (1)
- Simple Model For The Input Impedance of Coax-Fed Rectangular Microstrip Patch Antenna For CADDocument4 pagesSimple Model For The Input Impedance of Coax-Fed Rectangular Microstrip Patch Antenna For CADHoucine HoucineNo ratings yet
- Andrew CNT Braided Cable and Connector CatalogDocument20 pagesAndrew CNT Braided Cable and Connector CatalogCharlesNo ratings yet
- BW Broadcast DSPX-FM Datasheet PDFDocument1 pageBW Broadcast DSPX-FM Datasheet PDFwendyNo ratings yet
- SCIENCE 10 Q2 Module 5 Week 5 REVISEDDocument19 pagesSCIENCE 10 Q2 Module 5 Week 5 REVISEDJohn Clifford Ambaic JayomaNo ratings yet
- Peta Sebaran Rata-Rata Kecepatan Angin April 2014-2018 DI SELAT BALIDocument1 pagePeta Sebaran Rata-Rata Kecepatan Angin April 2014-2018 DI SELAT BALIhpbNo ratings yet
- CQ-DATV95 May 2021Document30 pagesCQ-DATV95 May 2021Benjamin DoverNo ratings yet
- 19 ZTE UMTS HandoverDocument60 pages19 ZTE UMTS Handoverselvam kksNo ratings yet
- Submarine ModelDocument11 pagesSubmarine Modelkvs ptpNo ratings yet
- STRK 685Document52 pagesSTRK 685ProgresionestubeNo ratings yet
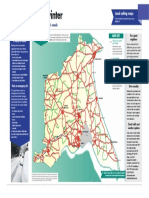
- East Riding Main Road SaltingDocument1 pageEast Riding Main Road SaltingzacklawsNo ratings yet
- How To Setup An Md380 For Use With A DMR RepeaterDocument7 pagesHow To Setup An Md380 For Use With A DMR RepeaternenadbjelicNo ratings yet
- TD-L1550A Instruction ManualDocument68 pagesTD-L1550A Instruction ManualAndaç ÖzkanNo ratings yet
- Kurdistan Institute For Computer Science GSM 4 Stage: 4 Week 3 Week 2 Week 1 Week Month YearDocument2 pagesKurdistan Institute For Computer Science GSM 4 Stage: 4 Week 3 Week 2 Week 1 Week Month YearGoranNo ratings yet
- Syllabus: Wave Analyzers: Frequency Selective Wave Analyzer, Heterodyne Wave Analyzer, DistortionDocument16 pagesSyllabus: Wave Analyzers: Frequency Selective Wave Analyzer, Heterodyne Wave Analyzer, DistortionVineela ThonduriNo ratings yet