You might also like
- Oral Soft Tissue Biopsies in Oporto, Portugal: An Eight Year Retrospective AnalysisDocument9 pagesOral Soft Tissue Biopsies in Oporto, Portugal: An Eight Year Retrospective Analysisjuan pablo meneses rojasNo ratings yet
- Posición Ante Los Antibióticos 2016Document40 pagesPosición Ante Los Antibióticos 2016Sydney LópezNo ratings yet
- Efficacy of A Mandibular Advancement Intraoral App PDFDocument8 pagesEfficacy of A Mandibular Advancement Intraoral App PDFJazmin CrNo ratings yet
- 49 IEJ Antibiotics 2010Document9 pages49 IEJ Antibiotics 2010tiara23No ratings yet
- Diagnosis and Treatment of Neurogenic Oropharyngeal DysphagiaFrom EverandDiagnosis and Treatment of Neurogenic Oropharyngeal DysphagiaNo ratings yet
- Anquiloglosia 2Document9 pagesAnquiloglosia 2trilceNo ratings yet
- Medoralv24 I5 p562Document9 pagesMedoralv24 I5 p562katherineNo ratings yet
- Antibiotics in Endodontics: A ReviewDocument16 pagesAntibiotics in Endodontics: A ReviewHisham HameedNo ratings yet
- Diagnosis and treatment of dentinal hypersensitivity: A reviewDocument10 pagesDiagnosis and treatment of dentinal hypersensitivity: A reviewadzhanahadyanNo ratings yet
- Review Article: Diagnostic Features of Common Oral Ulcerative Lesions: An Updated Decision TreeDocument15 pagesReview Article: Diagnostic Features of Common Oral Ulcerative Lesions: An Updated Decision TreemutiaNo ratings yet
- Clinical Characterization of Gingival Type of Burning Mouth Syndrome: A Cross-Sectional StudyDocument6 pagesClinical Characterization of Gingival Type of Burning Mouth Syndrome: A Cross-Sectional StudydaruNo ratings yet
- Diagnosis and Treatment of Dentinal HypersensitivityDocument11 pagesDiagnosis and Treatment of Dentinal Hypersensitivity21-010 AisyahNo ratings yet
- A Pragmatic Evidence-Based Clinical Management Algorithm For Burning Mouth SyndromeDocument6 pagesA Pragmatic Evidence-Based Clinical Management Algorithm For Burning Mouth SyndromeMémoire StomatodynieNo ratings yet
- Headache - 2013 - Shephard - Orofacial Pain A Guide For The Headache PhysicianDocument18 pagesHeadache - 2013 - Shephard - Orofacial Pain A Guide For The Headache PhysicianNatalie JaraNo ratings yet
- 22826Document9 pages22826Ghina Mukti LuthfiaNo ratings yet
- Angle Class II Correction: Stepwise Mandibular Advancement or Bite Jumping?Document15 pagesAngle Class II Correction: Stepwise Mandibular Advancement or Bite Jumping?Esther Zapata FernándezNo ratings yet
- Topical Application in Burning Mouth Syndrome: SciencedirectDocument6 pagesTopical Application in Burning Mouth Syndrome: SciencedirectlepouletNo ratings yet
- Effectiveness of Myofunctional Therapy in Ankyloglossia: A Systematic ReviewDocument18 pagesEffectiveness of Myofunctional Therapy in Ankyloglossia: A Systematic Reviewmistic0No ratings yet
- Arto AtmDocument9 pagesArto AtmELIS JOHANA PATERNINA MOGUEANo ratings yet
- Ocular Complications Following Dental Local Anaesthesia (2011)Document7 pagesOcular Complications Following Dental Local Anaesthesia (2011)JohnNo ratings yet
- Polak Et Al-2015-Journal of Clinical Periodontology PDFDocument13 pagesPolak Et Al-2015-Journal of Clinical Periodontology PDFChristine HacheNo ratings yet
- Severe Odontogenic Infections: Epidemiological, Microbiological and Therapeutic FactorsDocument7 pagesSevere Odontogenic Infections: Epidemiological, Microbiological and Therapeutic FactorsPipin HeryantoNo ratings yet
- Tongue Injury Healing in Epileptic Teen: Case ReportDocument12 pagesTongue Injury Healing in Epileptic Teen: Case ReportJoão EduardoNo ratings yet
- Update On Oral Lichen PlanusDocument38 pagesUpdate On Oral Lichen PlanusBimalKrishnaNo ratings yet
- Diagnosis and Treatment of Chronic CoughFrom EverandDiagnosis and Treatment of Chronic CoughSang Heon ChoNo ratings yet
- Sindrome de SjrogenDocument10 pagesSindrome de SjrogenWesley RodriguesNo ratings yet
- Jced 10 E1145Document4 pagesJced 10 E1145lily oktarizaNo ratings yet
- Joor 12417Document9 pagesJoor 12417Javier Ramos GascaNo ratings yet
- Dental Pulp Testing - A ReviewDocument12 pagesDental Pulp Testing - A ReviewSara Loureiro da LuzNo ratings yet
- Orofacialpain:: A PrimerDocument10 pagesOrofacialpain:: A Primeranon_768201406No ratings yet
- Burian 2017Document5 pagesBurian 2017Saraswita Gabriellah SaetikhoNo ratings yet
- Is There An Association Between The Use of Antidepressants and Complications Involving Dental Implantes - A Systematic Review and Meta-AnalysisDocument8 pagesIs There An Association Between The Use of Antidepressants and Complications Involving Dental Implantes - A Systematic Review and Meta-AnalysisCaio GonçalvesNo ratings yet
- Population CellDocument9 pagesPopulation CellIana RusuNo ratings yet
- Univers Complu Madrid NBF - Cordales Alveolitis Por Extra.Document8 pagesUnivers Complu Madrid NBF - Cordales Alveolitis Por Extra.juan perezNo ratings yet
- 1807 3107 Bor 32 s01 E068 PDFDocument16 pages1807 3107 Bor 32 s01 E068 PDFCristina MagañaNo ratings yet
- Orofacial PainDocument7 pagesOrofacial PainAkram AlsharaeeNo ratings yet
- Interdisciplinary Diagnostic Research For Identification of BrushismDocument6 pagesInterdisciplinary Diagnostic Research For Identification of BrushismViviane MarquesNo ratings yet
- Ekso 1Document8 pagesEkso 1HASANUDDIN STNo ratings yet
- Effects of A Standard Versus Comprehensive Oral Care Protocol Among Intubated Neuroscience ICU Patients: Results of A Randomized Controlled TrialDocument13 pagesEffects of A Standard Versus Comprehensive Oral Care Protocol Among Intubated Neuroscience ICU Patients: Results of A Randomized Controlled TrialMohammed Falih HassanNo ratings yet
- Diagnosis and Treatment of Dentinal HypersensitivityDocument10 pagesDiagnosis and Treatment of Dentinal Hypersensitivitysuluv15No ratings yet
- DentalUpdate Classificationarticle PDFDocument8 pagesDentalUpdate Classificationarticle PDFdr vidyaNo ratings yet
- Incidence and Factors Associated With Flare-Ups in A Post Graduate Programme in The Indian PopulationDocument6 pagesIncidence and Factors Associated With Flare-Ups in A Post Graduate Programme in The Indian PopulationLeticia RiveraNo ratings yet
- Signs and Symptoms of Temporomandibular Joint Disorders Related To The Degree of Mouth Opening and Hearing LossDocument9 pagesSigns and Symptoms of Temporomandibular Joint Disorders Related To The Degree of Mouth Opening and Hearing LossFelipeSanzNo ratings yet
- Orthodontics in Obstructive Sleep Apnea Patients: A Guide to Diagnosis, Treatment Planning, and InterventionsFrom EverandOrthodontics in Obstructive Sleep Apnea Patients: A Guide to Diagnosis, Treatment Planning, and InterventionsSu-Jung KimNo ratings yet
- Medoralv16 I3 p425Document5 pagesMedoralv16 I3 p425Diana OliveiraNo ratings yet
- PneumoniaDocument8 pagesPneumoniaSoffie FitriyahNo ratings yet
- 1. Occl. Interf. and.Parafunct.Document9 pages1. Occl. Interf. and.Parafunct.daniel.correaNo ratings yet
- Temporomandibular Disorders - A Review of Current Concepts in Aetiology, Diagnosis, and ManagementDocument33 pagesTemporomandibular Disorders - A Review of Current Concepts in Aetiology, Diagnosis, and ManagementMatheus FalkenbachNo ratings yet
- SC12 Liu 2008Document9 pagesSC12 Liu 2008Ashish DambhareNo ratings yet
- Researcharticle Open Access: S. L. Forster, T. Real, K. P. Doucette and S. B. KingDocument11 pagesResearcharticle Open Access: S. L. Forster, T. Real, K. P. Doucette and S. B. KingVinny Vania ParindingNo ratings yet
- Retrospective analysis of benign oral tumours and lesionsDocument8 pagesRetrospective analysis of benign oral tumours and lesionspaolaNo ratings yet
- Animal StudiesDocument11 pagesAnimal StudiesmmyahooscribdNo ratings yet
- 2 Evaluation of The Short Term Effectiveness of Education Versus An Occlusal Splint For The Treatment of Myofascial Pain of The Jaw Muscles 1Document7 pages2 Evaluation of The Short Term Effectiveness of Education Versus An Occlusal Splint For The Treatment of Myofascial Pain of The Jaw Muscles 1Michael KronovNo ratings yet
- Steroid Control of Acute Middle Ear Inflammation in A Mouse ModelDocument5 pagesSteroid Control of Acute Middle Ear Inflammation in A Mouse ModelfryancakaNo ratings yet
- Technical Aspects of Treatment in Relation To Treatment OutcomeDocument14 pagesTechnical Aspects of Treatment in Relation To Treatment OutcomekochikaghochiNo ratings yet
- Medoral 21 E579Document8 pagesMedoral 21 E579AngiPaolaPuiconRuizNo ratings yet
- LiquenDocument10 pagesLiquenAna RiveraNo ratings yet
- Odontogenic Cysts - A Descriptive Clinicopathological StudyDocument6 pagesOdontogenic Cysts - A Descriptive Clinicopathological StudyAvif PutraNo ratings yet
- Assessment of Mri Findings and Clinical Symptoms in Patients With Temporomandibular Joint DisordersDocument8 pagesAssessment of Mri Findings and Clinical Symptoms in Patients With Temporomandibular Joint DisordersMarcela RibeiroNo ratings yet
- Pinto 2019Document7 pagesPinto 2019Marcela RibeiroNo ratings yet
- Segami 2001Document5 pagesSegami 2001Marcela RibeiroNo ratings yet
- Rosenbrg-Goss2020 Article AModifiedTechniqueOfTemporomanDocument10 pagesRosenbrg-Goss2020 Article AModifiedTechniqueOfTemporomanMarcela RibeiroNo ratings yet
- DC-TMD Brazilian Portuguese Assessment Instruments - 2020JUL14Document75 pagesDC-TMD Brazilian Portuguese Assessment Instruments - 2020JUL14Marcela RibeiroNo ratings yet
- Current and Emerging Evidence Based Treatment Options in Chronic MigraineDocument9 pagesCurrent and Emerging Evidence Based Treatment Options in Chronic MigraineMarcela RibeiroNo ratings yet
- Peterson's Principles of Oral and Maxillofacial Surgery 2nd Ed 2004Document1,477 pagesPeterson's Principles of Oral and Maxillofacial Surgery 2nd Ed 2004Hakan Iyisu89% (63)
- Cho2019 Clinical Features of Chronic Cluster Headache Based On Third EditionDocument13 pagesCho2019 Clinical Features of Chronic Cluster Headache Based On Third EditionMarcela RibeiroNo ratings yet
- Kenya National Oral Halth - SDocument72 pagesKenya National Oral Halth - SMaria Fernanda Garzon RojasNo ratings yet
- SRMJResDentSci73158-2129782 003529Document4 pagesSRMJResDentSci73158-2129782 003529MarsyaNo ratings yet
- ISTANBUL AYDIN UNIVERSITY STUDENTS PREPARE FOR EXCHANGE PROGRAMDocument12 pagesISTANBUL AYDIN UNIVERSITY STUDENTS PREPARE FOR EXCHANGE PROGRAMemiraksopNo ratings yet
- 14 Talking About Sickness and SymptomsDocument9 pages14 Talking About Sickness and SymptomsAdin SukamtoNo ratings yet
- Morning Case Report: Thursday, December 16 2021Document71 pagesMorning Case Report: Thursday, December 16 2021dikiprestya391No ratings yet
- Paper 1Document9 pagesPaper 1Gloria JaisonNo ratings yet
- 10 DOH Approved Herbal Medicine: Prepared By: Washington, Luis D. Student Nurse BSN 2H-DDocument11 pages10 DOH Approved Herbal Medicine: Prepared By: Washington, Luis D. Student Nurse BSN 2H-DLuis WashingtonNo ratings yet
- Pellitory Root Qualities and Benefits According To AyurvedaDocument8 pagesPellitory Root Qualities and Benefits According To Ayurvedavijender AtriNo ratings yet
- History of Endodontic TherapyDocument47 pagesHistory of Endodontic TherapyMohhamad Reza JouyandehNo ratings yet
- Schuessler Tissue Salts HandbookDocument52 pagesSchuessler Tissue Salts HandbookBashir Ahmed100% (2)
- v8s6b1m6 (Stu) EngDocument42 pagesv8s6b1m6 (Stu) EngFongVoonYukeNo ratings yet
- Lecture 2A The Chief Complaint Its HistoryDocument20 pagesLecture 2A The Chief Complaint Its HistoryAhmed HegazyNo ratings yet
- Reffered PainDocument26 pagesReffered PainHappy Septianto SNo ratings yet
- Diagnosing Dental ConditionsDocument136 pagesDiagnosing Dental Conditionsareej alblowi60% (10)
- PBL Pain/pulp VitalityDocument13 pagesPBL Pain/pulp VitalityVenukumar SanggarNo ratings yet
- 30 Natural Remedies You Need To Know AboutDocument38 pages30 Natural Remedies You Need To Know AboutMaria BarbaliaNo ratings yet
- Aviation Dentistry - Current Concepts and PracticeDocument6 pagesAviation Dentistry - Current Concepts and PracticeMaria Gerber RozaNo ratings yet
- Perawatan Gigi Goyang Dengan SplintingDocument5 pagesPerawatan Gigi Goyang Dengan SplintingibagaspNo ratings yet
- William Boericke Homeopathic Materia MedicaiiDocument592 pagesWilliam Boericke Homeopathic Materia MedicaiiWilson Bernardes100% (3)
- ĐỀ SỐ 29Document7 pagesĐỀ SỐ 29Joy English TeachersNo ratings yet
- Methods of Diagnosis and Treatment in Endodontics: A Systematic ReviewDocument32 pagesMethods of Diagnosis and Treatment in Endodontics: A Systematic ReviewHadil Altilbani100% (2)
- Tooth AcheDocument8 pagesTooth AcheWerly Eka LiaNo ratings yet
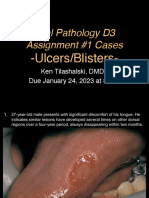
- D3 Ulcers Blisters Cases Due01242023 8amDocument13 pagesD3 Ulcers Blisters Cases Due01242023 8amLinh PhanNo ratings yet
- 27 Univerzalnih Kombinacija Tkivnih SoliDocument3 pages27 Univerzalnih Kombinacija Tkivnih SolimafkoNo ratings yet
- Reading Comprehension Marys Visit To The Dentist Reading Comprehension Exercises 138065Document2 pagesReading Comprehension Marys Visit To The Dentist Reading Comprehension Exercises 138065Stefania Popa50% (2)
- Toothache Pain: Dentist Teeth Tooth DecayDocument2 pagesToothache Pain: Dentist Teeth Tooth DecayRestu Yogi FahleviNo ratings yet
- Science of The Ancestors by D Keightley PDFDocument45 pagesScience of The Ancestors by D Keightley PDFMetcher Maa AkhiNo ratings yet
- EW20 - English Within 20 MinutesDocument81 pagesEW20 - English Within 20 MinutesNur Syakirah Isabel AbdullahNo ratings yet
- Pathological Repertory of NosodesDocument20 pagesPathological Repertory of Nosodespawajee100% (1)
- dōTERRA Clove OilDocument5 pagesdōTERRA Clove OilJacqui Decker100% (2)