You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (844)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5810)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (346)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- CNA InserviceDocument13 pagesCNA InserviceGeorgeWazuNo ratings yet
- Acyanotic Congenital Heart DiseaseDocument7 pagesAcyanotic Congenital Heart DiseaseSam Raj100% (1)
- Med Tech Sept 2019 Microbiology and ParasitologyDocument7 pagesMed Tech Sept 2019 Microbiology and ParasitologyDavid DollagaNo ratings yet
- Dipon Group: Standard Operating Procedure For Work Resumption During The Coronavirus PandemicDocument13 pagesDipon Group: Standard Operating Procedure For Work Resumption During The Coronavirus PandemictanoycometNo ratings yet
- Classification of AntibioticsDocument4 pagesClassification of AntibioticsNico AvellanaNo ratings yet
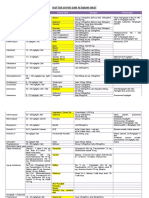
- Daftar Dosis Dan Sediaan ObatDocument7 pagesDaftar Dosis Dan Sediaan Obatdoru ubungNo ratings yet
- Ebook Gabbes Obstetrics Essentials Normal Problem Pregnancies PDF Full Chapter PDFDocument67 pagesEbook Gabbes Obstetrics Essentials Normal Problem Pregnancies PDF Full Chapter PDFandre.davis379100% (29)
- 3 FINAL LESSON PLAN ON UTI in PREGNANCYDocument24 pages3 FINAL LESSON PLAN ON UTI in PREGNANCYAkansha gandharvNo ratings yet
- Dhammarakshit Keshorao HirekhanDocument1 pageDhammarakshit Keshorao HirekhanDharmendra PantawaneNo ratings yet
- School RecordsDocument11 pagesSchool RecordsMohamed EbrahemNo ratings yet
- Toaz - Info Pedia1 09 Preventive Pediatric Healthcare PRDocument7 pagesToaz - Info Pedia1 09 Preventive Pediatric Healthcare PRCarla Elize DerainNo ratings yet
- Neonatal Abstinence SyndromeDocument9 pagesNeonatal Abstinence Syndromeapi-376040443No ratings yet
- Ballard Score Calculator: CalculatorsDocument1 pageBallard Score Calculator: Calculatorsbazlin syabrinaNo ratings yet
- Mod 105Document3 pagesMod 105ellithNo ratings yet
- Pathophysiology of HemorrhoidsDocument2 pagesPathophysiology of HemorrhoidsTrixie FayeNo ratings yet
- SteviaDocument10 pagesSteviaavagaliciousNo ratings yet
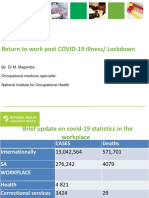
- Return To Work Post COVID-19 Illness/ LockdownDocument20 pagesReturn To Work Post COVID-19 Illness/ LockdownHuynh Luong Huy ThongNo ratings yet
- Rtog1005 Protocol PresentationDocument9 pagesRtog1005 Protocol Presentationapi-634067897No ratings yet
- Urinary Incontinence in The Older Adult: by Kristen Cook, Pharm.D., BCPS and Linda M. Sobeski, Pharm.D., BCPSDocument18 pagesUrinary Incontinence in The Older Adult: by Kristen Cook, Pharm.D., BCPS and Linda M. Sobeski, Pharm.D., BCPSNurul HafizaNo ratings yet
- Hospital For Free Treatment - Star Foundation Designed PDFDocument14 pagesHospital For Free Treatment - Star Foundation Designed PDFSagar ShiriskarNo ratings yet
- RBC AliquotsDocument1 pageRBC AliquotsARIF AHAMMEDNo ratings yet
- Study Questions Chapter 3: Health-Risk BehaviourDocument3 pagesStudy Questions Chapter 3: Health-Risk BehaviourZakariaNo ratings yet
- Canal of Nuck Hernia in An Elderly Patient A Case ReportDocument8 pagesCanal of Nuck Hernia in An Elderly Patient A Case ReportAthenaeum Scientific PublishersNo ratings yet
- ACC Vaccine-Related Injury ClaimsDocument7 pagesACC Vaccine-Related Injury ClaimsLaura WaltersNo ratings yet
- Health Information For Travelers To India - Clinician View - Travelers' Health - CDCDocument9 pagesHealth Information For Travelers To India - Clinician View - Travelers' Health - CDCRumana AliNo ratings yet
- 14230-Article Text-64397-1-10-20170503Document5 pages14230-Article Text-64397-1-10-20170503IqF SayNo ratings yet
- A Case of Medication Error: Conversion Factors in Clinical CalculationsDocument4 pagesA Case of Medication Error: Conversion Factors in Clinical CalculationsSherein ShalabyNo ratings yet
- Daftar PustakaDocument3 pagesDaftar PustakamuhammadrikiNo ratings yet
- Lincomycin HydrochlorideDocument1 pageLincomycin HydrochlorideDiego TorresNo ratings yet
- Ibufen 600 Caplets: Summary of Product CharacteristicsDocument13 pagesIbufen 600 Caplets: Summary of Product Characteristicsddandan_2No ratings yet