You might also like
- Final Coaching NP4 Set 2Document18 pagesFinal Coaching NP4 Set 2STEFFI GABRIELLE GOLEZNo ratings yet
- MS Critical Thinking DrillsDocument18 pagesMS Critical Thinking DrillsSTEFFI GABRIELLE GOLEZ100% (1)
- Final Coaching NP3 Set3Document14 pagesFinal Coaching NP3 Set3STEFFI GABRIELLE GOLEZNo ratings yet
- Top Up Training Center and Research Consultancy Communicable Disease NursingDocument3 pagesTop Up Training Center and Research Consultancy Communicable Disease NursingSTEFFI GABRIELLE GOLEZNo ratings yet
- IMCI Case Management: Classification Focused AssessmentDocument42 pagesIMCI Case Management: Classification Focused AssessmentSTEFFI GABRIELLE GOLEZNo ratings yet
- Final Coaching NP4 Set 1Document13 pagesFinal Coaching NP4 Set 1STEFFI GABRIELLE GOLEZNo ratings yet
- MS TopUp HandoutDocument4 pagesMS TopUp HandoutSTEFFI GABRIELLE GOLEZNo ratings yet
- K - Worksheet 0-5Document1 pageK - Worksheet 0-5STEFFI GABRIELLE GOLEZNo ratings yet
- Endocrine System: Major Hormone Secreting Glands: 1. HypothalamusDocument5 pagesEndocrine System: Major Hormone Secreting Glands: 1. HypothalamusSTEFFI GABRIELLE GOLEZNo ratings yet
- Final Na Living Rosary Script 7Document8 pagesFinal Na Living Rosary Script 7STEFFI GABRIELLE GOLEZNo ratings yet
- University of Santo To MasDocument3 pagesUniversity of Santo To MasSTEFFI GABRIELLE GOLEZNo ratings yet
- Clinphar Lec 4 Diabetes Mellitus 1Document18 pagesClinphar Lec 4 Diabetes Mellitus 1STEFFI GABRIELLE GOLEZNo ratings yet
- POC - Review NotesDocument9 pagesPOC - Review NotesSTEFFI GABRIELLE GOLEZNo ratings yet
- Personal Information: Apartment / Unit / Building / Floor / Etc. Street Address / P.O. Box / Company NameDocument2 pagesPersonal Information: Apartment / Unit / Building / Floor / Etc. Street Address / P.O. Box / Company NameSTEFFI GABRIELLE GOLEZNo ratings yet
- Golez Ca CHN Ola PPTDocument17 pagesGolez Ca CHN Ola PPTSTEFFI GABRIELLE GOLEZNo ratings yet
- Anaphy CKDDocument3 pagesAnaphy CKDSTEFFI GABRIELLE GOLEZNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- HYPOGLYCEMIADocument20 pagesHYPOGLYCEMIAJohn Patrick MacasasaNo ratings yet
- Ferrans and Powers Quality of Life Index Diabetes Version - IiiDocument4 pagesFerrans and Powers Quality of Life Index Diabetes Version - IiiDaniela IpateNo ratings yet
- The Use of Cgms in Redefining Care Delivery For Type 2 DiabetesDocument8 pagesThe Use of Cgms in Redefining Care Delivery For Type 2 DiabetesChrisSandersNo ratings yet
- Glucose Lab ReportDocument12 pagesGlucose Lab ReportKing Everest86% (7)
- Pediatric DiabeticDocument9 pagesPediatric Diabeticperla islasNo ratings yet
- Chapter 34 Insulin & Oral Antidiabetic DrugsDocument24 pagesChapter 34 Insulin & Oral Antidiabetic DrugsIlham RamadhanNo ratings yet
- InsulinDocument1 pageInsulinm.arba'a putradiNo ratings yet
- Sehat Nov 2022Document20 pagesSehat Nov 2022prolanis puskesmaskendal1No ratings yet
- Insulin Adjustment Workbook CompleteDocument53 pagesInsulin Adjustment Workbook CompletetskumarphdNo ratings yet
- Drug-Study-Metformin 1Document2 pagesDrug-Study-Metformin 1Caroline Cha100% (1)
- Nclex Endocrine ReviewerDocument43 pagesNclex Endocrine ReviewerBryle SaladarNo ratings yet
- My Own Type1 Diabetes BookDocument43 pagesMy Own Type1 Diabetes BookElaineBuchhornNo ratings yet
- Diabetes Mellitus: Ma. Tosca Cybil A. Torres, RN, ManDocument66 pagesDiabetes Mellitus: Ma. Tosca Cybil A. Torres, RN, ManyuliNo ratings yet
- Nycocard Reader PrincipleDocument6 pagesNycocard Reader Principlemrhrtn88No ratings yet
- S1 2022 429533 BibliographyDocument7 pagesS1 2022 429533 BibliographyNur WahyuniNo ratings yet
- 15 Easy Ways To Lower Blood Sugar Levels NaturallyDocument12 pages15 Easy Ways To Lower Blood Sugar Levels NaturallyJ SmithNo ratings yet
- Insulin ResistanceDocument12 pagesInsulin ResistancePrabhmeet GroverNo ratings yet
- Diabetes Mellitus: DR Hiew Fu LiongDocument30 pagesDiabetes Mellitus: DR Hiew Fu LiongamminsaffriNo ratings yet
- Diagnostic Report: FinalDocument3 pagesDiagnostic Report: Finalpraveen04715717No ratings yet
- ENDOCRINE PRACTICE Rapid Electronic Article in Press: AACE/ACE Consensus StatementDocument66 pagesENDOCRINE PRACTICE Rapid Electronic Article in Press: AACE/ACE Consensus StatementMUHAMMAD09No ratings yet
- Optium Neo HDocument2 pagesOptium Neo HBella Icahyani Subarsa100% (1)
- Diabetes Blood Glucose Meter & Strip Product Reference - FOR INTERNAL USE ONLYDocument2 pagesDiabetes Blood Glucose Meter & Strip Product Reference - FOR INTERNAL USE ONLYLorie FadolNo ratings yet
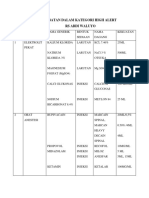
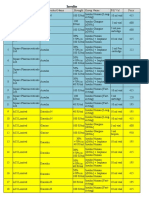
- Obat High AlertDocument5 pagesObat High AlertChia GracellaNo ratings yet
- Diabetes PPT FianlDocument31 pagesDiabetes PPT FianlUqba MishalNo ratings yet
- Hansen 2016 Impact of Endurance Exercise Training in The Fasted StateDocument14 pagesHansen 2016 Impact of Endurance Exercise Training in The Fasted StateYo Vivo Fit Pablo y KarlaNo ratings yet
- Pump SuppDocument3 pagesPump SuppAkshit R ShahNo ratings yet
- Gestational Diabetes Mellitus - Glycemic Control and Maternal Prognosis - UpToDateDocument46 pagesGestational Diabetes Mellitus - Glycemic Control and Maternal Prognosis - UpToDateBruno FernandesNo ratings yet
- Causes of Metabolic AcidosisDocument10 pagesCauses of Metabolic AcidosisKimberly Anne SP PadillaNo ratings yet
- Insulin InfoDocument4 pagesInsulin Infomonoj5859No ratings yet
- MSC Unit 7 Insulin Pharmacology 1 & 2 ATTOUBDocument29 pagesMSC Unit 7 Insulin Pharmacology 1 & 2 ATTOUBalsuwaijiNo ratings yet