You might also like
- Comprehensive Guide On Lucid Dreaming PDFDocument52 pagesComprehensive Guide On Lucid Dreaming PDFJohn Dean91% (11)
- Acupuncture Point GroupingsDocument8 pagesAcupuncture Point Groupingskm_ananthNo ratings yet
- Worksheet Circulation Grade 10 PDFDocument2 pagesWorksheet Circulation Grade 10 PDFCarl Agape DavisNo ratings yet
- NIPPVDocument35 pagesNIPPVAnusha VergheseNo ratings yet
- CPAPDocument53 pagesCPAPvibhurocksNo ratings yet
- Mechanical VentilationDocument18 pagesMechanical VentilationM BNo ratings yet
- Introduction To Mechanical Ventilation PDFDocument46 pagesIntroduction To Mechanical Ventilation PDFDaniel Edward Ricardo MalauNo ratings yet
- Midterm Last TopicDocument3 pagesMidterm Last TopicLynette BalodNo ratings yet
- Bubble Nasal CPAPDocument83 pagesBubble Nasal CPAPJunior763No ratings yet
- Introduction to Mechanical VentilatorsDocument22 pagesIntroduction to Mechanical VentilatorsGurinder GillNo ratings yet
- Mechanical Ventilator Modes and Settings ExplainedDocument32 pagesMechanical Ventilator Modes and Settings Explainedarshad209No ratings yet
- Non Invasive VentilationDocument22 pagesNon Invasive VentilationOrion JohnNo ratings yet
- Neonatal VentilationDocument65 pagesNeonatal VentilationBadr Chaban100% (5)
- Bipap Ventilation Basic and MonitoringDocument33 pagesBipap Ventilation Basic and MonitoringPradip ChougaleNo ratings yet
- Care and Basic Settings of Portable Ventilator 2Document27 pagesCare and Basic Settings of Portable Ventilator 2febian_henryNo ratings yet
- Overview of Respiratory Failure & Mechanical VentilationDocument89 pagesOverview of Respiratory Failure & Mechanical VentilationsheharyarNo ratings yet
- Care and Basic Settings of Portable VentilatorDocument22 pagesCare and Basic Settings of Portable Ventilatorfebian_henry100% (2)
- Mechanical+Ventilation-Basics+for+Beginners (Unlocked by ComDocument49 pagesMechanical+Ventilation-Basics+for+Beginners (Unlocked by Comdokidok100% (14)
- Sleep Assessment Diagnosis PlanDocument2 pagesSleep Assessment Diagnosis PlanKenneth Gabriel Catulin50% (2)
- Cpap-Bipap: Sussan Soltani Mohammadi - MDDocument41 pagesCpap-Bipap: Sussan Soltani Mohammadi - MDbandarascbNo ratings yet
- Dr. Rosi - CPAPDocument65 pagesDr. Rosi - CPAPtom24No ratings yet
- CH 14 Digestive System and Body MetabolismDocument21 pagesCH 14 Digestive System and Body MetabolismKim Buenaflor GaloyoNo ratings yet
- Acute Respiratory FailureDocument34 pagesAcute Respiratory FailureStuDIEng100% (1)
- Continuous Positive Airway Pressure (CPAP)Document53 pagesContinuous Positive Airway Pressure (CPAP)indiamahesh100% (1)
- Health Assessment of Bronchial Asthma PatientDocument3 pagesHealth Assessment of Bronchial Asthma PatientShetal SharmaNo ratings yet
- Optional (AEMT), Optional (Paramedic)Document76 pagesOptional (AEMT), Optional (Paramedic)Mark ReinhardtNo ratings yet
- NIV Pediatric Respiratory SupportDocument96 pagesNIV Pediatric Respiratory SupportbhongskirnNo ratings yet
- NIV (Non-Invasive Ventilation) : Dr.S.MagimaiguberanDocument38 pagesNIV (Non-Invasive Ventilation) : Dr.S.MagimaiguberanDr mahi sNo ratings yet
- Federal Democratic Republic of Ethiopia Ministry of HealthDocument43 pagesFederal Democratic Republic of Ethiopia Ministry of HealthdagemNo ratings yet
- CPAP IMV BookDocument33 pagesCPAP IMV BooksiputamaliaputriNo ratings yet
- CPAP NEONATES RESPIRATORY SUPPORTDocument33 pagesCPAP NEONATES RESPIRATORY SUPPORTSam RassamNo ratings yet
- Final VentilatorDocument62 pagesFinal VentilatorDrmirfat AlkashifNo ratings yet
- My Own Critical Care NotesDocument4 pagesMy Own Critical Care NotesSamer GobreialNo ratings yet
- DR - Rajalakshmi.C: Emergency Physician MMHRC Institute of Emergency MedicineDocument22 pagesDR - Rajalakshmi.C: Emergency Physician MMHRC Institute of Emergency MedicineP Vinod KumarNo ratings yet
- HIGH FLOW NASAL CANNULADocument6 pagesHIGH FLOW NASAL CANNULALord King LlamasNo ratings yet
- Nasalintermittentpositive Pressureventilationfor Neonatalrespiratorydistress SyndromeDocument20 pagesNasalintermittentpositive Pressureventilationfor Neonatalrespiratorydistress SyndromeBella FebriantiNo ratings yet
- Nasal IMV - Gatot PDFDocument43 pagesNasal IMV - Gatot PDFtutiarlyNo ratings yet
- MomvDocument68 pagesMomvSaddamNo ratings yet
- Jorrnal Reading NIV HFNO ChogaDocument23 pagesJorrnal Reading NIV HFNO ChogaChoga ArlandoNo ratings yet
- Lecture Anwar Ventilation Managment COVIDDocument28 pagesLecture Anwar Ventilation Managment COVIDمحمدرزازالتبعيNo ratings yet
- High Frequency VentilationDocument33 pagesHigh Frequency VentilationMarie PetalcorinNo ratings yet
- Oxygen Delivery Devices: Reported By: Marvin PermisonDocument18 pagesOxygen Delivery Devices: Reported By: Marvin PermisonMedeah Faye AbesNo ratings yet
- Non-Invasive Ventilation 2Document25 pagesNon-Invasive Ventilation 2Ramanesh DNo ratings yet
- Oxygen InsufficiencyDocument52 pagesOxygen InsufficiencyAnn Merlin JobinNo ratings yet
- 8 - PEEP in Emergency RoomDocument30 pages8 - PEEP in Emergency Roomsyahputra88No ratings yet
- Mechanical Ventilation: An Overview of Types, Parameters, and Nursing CareDocument123 pagesMechanical Ventilation: An Overview of Types, Parameters, and Nursing CareKristine C.No ratings yet
- Performing a PAP Titration: Understanding PAP Therapy and EquipmentDocument53 pagesPerforming a PAP Titration: Understanding PAP Therapy and EquipmentSamNo ratings yet
- NIV TeachingDocument12 pagesNIV TeachingZahraa Al-MayahiNo ratings yet
- Guidelines For Use of Bubble-CPAP ConcentratorsDocument10 pagesGuidelines For Use of Bubble-CPAP ConcentratorsevanNo ratings yet
- Ventilator Settings GuideDocument7 pagesVentilator Settings Guidearnol3090No ratings yet
- Positive Expiratory PressureDocument21 pagesPositive Expiratory PressureVijayalaxmi KathareNo ratings yet
- Bi-Level and Non-Invasive Intermittent Postive Pressure VentilationDocument51 pagesBi-Level and Non-Invasive Intermittent Postive Pressure VentilationHaryaman JustisiaNo ratings yet
- Respiratory Support (IMTs PAs)Document30 pagesRespiratory Support (IMTs PAs)Steve McLarenNo ratings yet
- Respiratory Medical Residents PresentationDocument50 pagesRespiratory Medical Residents PresentationRayhan ShariffNo ratings yet
- Mechanical Ventilation: Gian Carlo T. Rabago RN MD Tondo Medical Center Department of SurgeryDocument16 pagesMechanical Ventilation: Gian Carlo T. Rabago RN MD Tondo Medical Center Department of SurgeryGian Carlo RabagoNo ratings yet
- Care of Patients Requiring Oxygen Therapy or TracheostomyDocument5 pagesCare of Patients Requiring Oxygen Therapy or TracheostomyAnnie Rose Dorothy MamingNo ratings yet
- PepDocument8 pagesPepUdayakrishnan P Kanhangad100% (1)
- Practical Application of CPAP: Dr. Srinivas MurkiDocument8 pagesPractical Application of CPAP: Dr. Srinivas MurkiRaji MohanNo ratings yet
- CPAPDocument13 pagesCPAPआशिष दादाNo ratings yet
- Gian Carlo T. Rabago RN MD Tondo Medical Center Department of SurgeryDocument16 pagesGian Carlo T. Rabago RN MD Tondo Medical Center Department of SurgeryGian Carlo RabagoNo ratings yet
- Gian Carlo T. Rabago RN MD Tondo Medical Center Department of SurgeryDocument16 pagesGian Carlo T. Rabago RN MD Tondo Medical Center Department of SurgeryGian Carlo RabagoNo ratings yet
- Ventilatory Support in NeonatesDocument27 pagesVentilatory Support in NeonatesGaylinel BongyadNo ratings yet
- Mechanical VentilatorsDocument11 pagesMechanical VentilatorsIra Katrina Bernales MendozaNo ratings yet
- Oxygenation - Peri Intubation, Apnoeic, THRIVEDocument40 pagesOxygenation - Peri Intubation, Apnoeic, THRIVEMahima LakhanpalNo ratings yet
- Respiratory Monitoring in Mechanical Ventilation: Techniques and ApplicationsFrom EverandRespiratory Monitoring in Mechanical Ventilation: Techniques and ApplicationsJian-Xin ZhouNo ratings yet
- KRTN Sejarah Pengertian Umum Karantina TumbuhanDocument35 pagesKRTN Sejarah Pengertian Umum Karantina TumbuhanYoga EkoNo ratings yet
- Dilemma in Treating GERD and CAD PatientsDocument8 pagesDilemma in Treating GERD and CAD PatientsYoga EkoNo ratings yet
- Rights and Responsibilities of Doctors and Patients: PreambleDocument6 pagesRights and Responsibilities of Doctors and Patients: PreambleYoga EkoNo ratings yet
- Approaches, Skills and Styles of LeadershipDocument7 pagesApproaches, Skills and Styles of LeadershipRoger MoyoNo ratings yet
- Doctor and Patient (Edit)Document3 pagesDoctor and Patient (Edit)Yoga EkoNo ratings yet
- Doctor and Patient (Edit)Document3 pagesDoctor and Patient (Edit)Yoga EkoNo ratings yet
- Heterotrophic Nutrition ExplainedDocument12 pagesHeterotrophic Nutrition ExplainedSankalp MouryaNo ratings yet
- Digestive System Organs AnswersDocument6 pagesDigestive System Organs AnswersralucaNo ratings yet
- AMI Equipment Services and Solutions, Inc. Biomedical Engineering DepartmentDocument11 pagesAMI Equipment Services and Solutions, Inc. Biomedical Engineering Departmentvandolph siribanNo ratings yet
- Circadian-LightingDocument2 pagesCircadian-Lightingiklem79No ratings yet
- Privação Do SonoDocument3 pagesPrivação Do SonoHugo BarbosaNo ratings yet
- Jawaban Tugas Kelompok 1 - B.Inggris KesehatanDocument7 pagesJawaban Tugas Kelompok 1 - B.Inggris KesehatanRia NurevitaNo ratings yet
- Edid6508group 3 Storyboardcorrectedversion1Document35 pagesEdid6508group 3 Storyboardcorrectedversion1api-349780383No ratings yet
- Raspored 2020-2021 Medicinski Engleski IIIDocument5 pagesRaspored 2020-2021 Medicinski Engleski IIIGracia GrabarićNo ratings yet
- Year 6 Science and Reading The Circulatory System Comprehension 3 Levels With AnswersDocument6 pagesYear 6 Science and Reading The Circulatory System Comprehension 3 Levels With AnswersVeronica NiemNo ratings yet
- Circulatory Pathway Through The Heart: Biology - CirculationDocument34 pagesCirculatory Pathway Through The Heart: Biology - CirculationLejNo ratings yet
- Vital Signs and Oxygen AdministrationDocument11 pagesVital Signs and Oxygen AdministrationCrisha Shane BoticarioNo ratings yet
- Quiz - ScienceDocument22 pagesQuiz - ScienceGregoryNo ratings yet
- Respiratory SystemDocument16 pagesRespiratory SystemCristel Marie Matan Rojas100% (3)
- CH 15Document26 pagesCH 15Mohd Khairidzman BoeranNo ratings yet
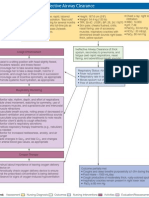
- Oxygenation strategies for ineffective airway clearanceDocument1 pageOxygenation strategies for ineffective airway clearanceNikki Beverly G. BacaleNo ratings yet
- Body System Checklist 1Document6 pagesBody System Checklist 1api-421876825No ratings yet
- Diagnosis and Treatment of Obstructive Sleep Apnea in AdultsDocument8 pagesDiagnosis and Treatment of Obstructive Sleep Apnea in AdultsTeuku Ilham AkbarNo ratings yet
- Sleeping Twice British English TeacherDocument12 pagesSleeping Twice British English TeacherIgorNo ratings yet
- Body SystemsDocument44 pagesBody SystemsRodgen GerasolNo ratings yet
- Mitochondria Is The Powerhouse of The CellDocument2 pagesMitochondria Is The Powerhouse of The CellSenap AwitNo ratings yet
- Bio 6.4 Quick QuizDocument2 pagesBio 6.4 Quick QuizMaya PlewniaNo ratings yet
- Blood Bank Data Collection FormDocument3 pagesBlood Bank Data Collection Formpbta punjab100% (1)
- The Endocrine System and HormonesDocument3 pagesThe Endocrine System and HormonesBrylle GandaNo ratings yet