You might also like
- Long-Term Mechanical Ventilation Toolkit For Adult Acute Care Providers PDFDocument70 pagesLong-Term Mechanical Ventilation Toolkit For Adult Acute Care Providers PDFSelvi SoundararajanNo ratings yet
- The Oxygen AdvantageDocument5 pagesThe Oxygen AdvantageJOHN0% (1)
- Standard Medical Operating Guidelines SMOG For Critical Care Flight PDFDocument278 pagesStandard Medical Operating Guidelines SMOG For Critical Care Flight PDFDaniel VacacelaNo ratings yet
- Nasogastric Tube InsertionDocument15 pagesNasogastric Tube InsertionHOney Maban Makilang100% (1)
- NG TubeDocument23 pagesNG TubeAll Bwin100% (1)
- Nasogastric Tube (NGT)Document31 pagesNasogastric Tube (NGT)annyeong_123No ratings yet
- Confined-Space-Entry ProcedureDocument18 pagesConfined-Space-Entry ProcedureMayur100% (1)
- Procedure ON Bladder Irrigation: SUBMITTED TO: Mr. EKE Lama TamangDocument17 pagesProcedure ON Bladder Irrigation: SUBMITTED TO: Mr. EKE Lama TamangRajaNo ratings yet
- Gastrostomy Tube Placement GuideDocument8 pagesGastrostomy Tube Placement GuideRio Gonzales100% (1)
- Promoting Nutrition (Enteral Nutrition)Document51 pagesPromoting Nutrition (Enteral Nutrition)Yayin Pestaño100% (1)
- Nasogastric Tube InsertionDocument18 pagesNasogastric Tube InsertionSandya PallapotuNo ratings yet
- Nasogastric Tube: - Insertion - FeedingDocument61 pagesNasogastric Tube: - Insertion - FeedingJustine Cagatan75% (4)
- A Clinician - S Guide To Cardiopulmonary Exercise Testing 2 - Test InterpretationDocument23 pagesA Clinician - S Guide To Cardiopulmonary Exercise Testing 2 - Test InterpretationjimurgaNo ratings yet
- Nasogastric TubeDocument41 pagesNasogastric TubeLouela de Asas100% (1)
- Tube FeedingDocument154 pagesTube FeedingMark Alden Padua100% (1)
- Nasogastric Tube GuideDocument7 pagesNasogastric Tube GuideAltrOi AgtangNo ratings yet
- Coanal AtresiaDocument4 pagesCoanal AtresiaBkas GrgNo ratings yet
- Orogastric Tube InsertionDocument5 pagesOrogastric Tube InsertionUday KumarNo ratings yet
- Medical Gas Pipeline SystemsDocument202 pagesMedical Gas Pipeline Systemsshahrul aiman100% (2)
- NutritionDocument53 pagesNutritionalelichengNo ratings yet
- Nasogastric Tube (NGT) Inserting PurposesDocument4 pagesNasogastric Tube (NGT) Inserting PurposesJECYL MAE MENORNo ratings yet
- NGTDocument4 pagesNGTRuthie BangteganNo ratings yet
- Nasogastric IntubationDocument4 pagesNasogastric IntubationDaphnie Mikaela Belarmino LayuganNo ratings yet
- NGT PresentationDocument23 pagesNGT PresentationniyigokNo ratings yet
- Procedure-Nasogastric Tube InsertionDocument22 pagesProcedure-Nasogastric Tube Insertionmohamad dildarNo ratings yet
- NCM 112 - Module (Rle) SemifinalDocument17 pagesNCM 112 - Module (Rle) SemifinalHelen GonzalesNo ratings yet
- Nasogastric Tube InsertionDocument3 pagesNasogastric Tube InsertionLorenza VillarinoNo ratings yet
- Nasogastric Tube Insertion AND Feeding: Mrs. Pramodini R. KhobragadeDocument35 pagesNasogastric Tube Insertion AND Feeding: Mrs. Pramodini R. Khobragadeomar kmr97No ratings yet
- Nasogastric Tube Insertion TechniquesDocument1 pageNasogastric Tube Insertion TechniquesAngelo Enriquez MañiboNo ratings yet
- Nasogastric Feeding TubeDocument7 pagesNasogastric Feeding Tubepatrayati90No ratings yet
- Guide to Endotracheal and Nasogastric Intubation ProceduresDocument9 pagesGuide to Endotracheal and Nasogastric Intubation ProceduresKate AbellaNo ratings yet
- Ccu NotesDocument76 pagesCcu NotesAr PeeNo ratings yet
- Nasogastric TubeDocument5 pagesNasogastric TubeangelaNo ratings yet
- Naspo Gastric Tube Feeding FinalDocument32 pagesNaspo Gastric Tube Feeding FinalNezuko0% (1)
- Nasogastric NG Tube PlacementDocument10 pagesNasogastric NG Tube PlacementA.J PolyNo ratings yet
- Nasogastric Intubation Insertion Procedures & TechniqueDocument1 pageNasogastric Intubation Insertion Procedures & TechniquePaola OrtizNo ratings yet
- Care To The Digestive SystemDocument16 pagesCare To The Digestive SystemSONGA AmriNo ratings yet
- Module 3 Nursing Skills Procedure On GI, Endo-Metab Concept (A)Document18 pagesModule 3 Nursing Skills Procedure On GI, Endo-Metab Concept (A)Nashebah A. BatuganNo ratings yet
- Nasogastric Tubes 1Document3 pagesNasogastric Tubes 1mak40No ratings yet
- NGT Insertion: Group 2 Guerrero, Gumatay, Lim, Lopez, Mallabo, Miñano, Nario, Olores, Paaño, Pajutan, Paz, PerezDocument19 pagesNGT Insertion: Group 2 Guerrero, Gumatay, Lim, Lopez, Mallabo, Miñano, Nario, Olores, Paaño, Pajutan, Paz, PerezHarlyn MagsinoNo ratings yet
- Nasogastric IntubationDocument3 pagesNasogastric IntubationkisffffNo ratings yet
- Nasogastric IntubationDocument6 pagesNasogastric IntubationNadia RivadeneiraNo ratings yet
- Og NGDocument22 pagesOg NGSandya PallapotuNo ratings yet
- Nasogastric Tube InsertionDocument17 pagesNasogastric Tube InsertionMichael Jude MedallaNo ratings yet
- Guidelines for Enteral Feeding TubesDocument19 pagesGuidelines for Enteral Feeding TubesAjeng SuparwiNo ratings yet
- Surgical InstrumentsDocument28 pagesSurgical InstrumentsNama Best100% (1)
- Western Mindanao State University: VisionDocument86 pagesWestern Mindanao State University: VisionHilde RobynNo ratings yet
- Objectives: at The End of The Discussion The Students Will Be Able ToDocument6 pagesObjectives: at The End of The Discussion The Students Will Be Able ToMichael Angelo SeñaNo ratings yet
- As Sig Ment For Remedial ExamDocument8 pagesAs Sig Ment For Remedial ExamBang DeNo ratings yet
- Gastrostomy, Duodenostomy and Jejunostomy Care GuideDocument5 pagesGastrostomy, Duodenostomy and Jejunostomy Care GuideRocco WalksNo ratings yet
- Nasogastric Tube FeedingDocument2 pagesNasogastric Tube FeedingCelline Isabelle ReyesNo ratings yet
- Feeding by Nasogastric TubesDocument3 pagesFeeding by Nasogastric TubesLheidaniel MMM.No ratings yet
- Nasogastric Intubation Technique Step-by-Step GuideDocument4 pagesNasogastric Intubation Technique Step-by-Step GuideLip StickNo ratings yet
- NGT Feeding Discussion InotDocument2 pagesNGT Feeding Discussion InotRhenelyn Delos ReyesNo ratings yet
- NG Tube Lictures 2023Document22 pagesNG Tube Lictures 2023ALi NursingNo ratings yet
- NGT Peritoneal LavageDocument12 pagesNGT Peritoneal LavageJeffrey Dela CruzNo ratings yet
- Nasogastric Tube Placement: Indications, Technique & ComplicationsDocument2 pagesNasogastric Tube Placement: Indications, Technique & Complicationseloiza custodioNo ratings yet
- NASOGASTRIC INSERTION AND FEEDING PROCEDUREDocument5 pagesNASOGASTRIC INSERTION AND FEEDING PROCEDUREXie AraoNo ratings yet
- DONE - NCM 116 RLE Week 7 ROXASDocument11 pagesDONE - NCM 116 RLE Week 7 ROXASBatiao Camille ClaireNo ratings yet
- Nasogastric Tubes Insertion of NotesDocument4 pagesNasogastric Tubes Insertion of NotesJenny WongNo ratings yet
- NasopharyngealairwayDocument16 pagesNasopharyngealairwayChyndi dami 1216No ratings yet
- احمد كريمDocument12 pagesاحمد كريمMr. abbas fahim hamidNo ratings yet
- SuctioningDocument7 pagesSuctioningKat AlaNo ratings yet
- Gastrointestinal Intubation: Nasogastric TubesDocument29 pagesGastrointestinal Intubation: Nasogastric TubesAgastya JanardhanaNo ratings yet
- NG Tube InsertionDocument37 pagesNG Tube InsertionSarah BirechNo ratings yet
- Gastrointestinal Interventional Endoscopy: Advanced TechniquesFrom EverandGastrointestinal Interventional Endoscopy: Advanced TechniquesMihir S. WaghNo ratings yet
- Biliopancreatic Endoscopy: Practical ApplicationFrom EverandBiliopancreatic Endoscopy: Practical ApplicationKwok-Hung LaiNo ratings yet
- Automatic Home Asthma DeviceDocument67 pagesAutomatic Home Asthma DeviceIbsa GetachoNo ratings yet
- Nur 111 - Sas18Document2 pagesNur 111 - Sas18Michelle Jennifer De Castro FagaraganNo ratings yet
- Oxygen Cylinder MSDS General IndustrialDocument4 pagesOxygen Cylinder MSDS General IndustrialarvindsarkarNo ratings yet
- SKH - Myofunctional Therapy and Nasal Breathing Exercises - FADocument2 pagesSKH - Myofunctional Therapy and Nasal Breathing Exercises - FAAmitava MukherjeeNo ratings yet
- Scoring Systems in Anesthesia and PACUDocument16 pagesScoring Systems in Anesthesia and PACUmissyaaaaNo ratings yet
- Mathematical modelling of ventilation mechanics tutorialDocument8 pagesMathematical modelling of ventilation mechanics tutorialHassan FahsNo ratings yet
- High-Flow Nasal Cannula Pada Anak (Literatur Review) : Avalilable OnlineDocument12 pagesHigh-Flow Nasal Cannula Pada Anak (Literatur Review) : Avalilable Onlinejeinzen14No ratings yet
- CPR AssignmentDocument3 pagesCPR AssignmentMUHAMAD FADZLI BIN SUDIN MoeNo ratings yet
- Dioctyl Sulfosuccinate, Sodium SaltDocument4 pagesDioctyl Sulfosuccinate, Sodium SaltWieke SusilawatiNo ratings yet
- Science 9 ODL IDEA WK1 L1 PRINTEDDocument3 pagesScience 9 ODL IDEA WK1 L1 PRINTEDClarice Jenn MaltoNo ratings yet
- Influence of Pranayama On Respiratory Function of Middle Age WomenDocument4 pagesInfluence of Pranayama On Respiratory Function of Middle Age WomenInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- 1359 Eng PDFDocument1 page1359 Eng PDFHaleem Ur Rashid BangashNo ratings yet
- 1,2-Benzisothiazoline-3-One: Human Health EffectsDocument24 pages1,2-Benzisothiazoline-3-One: Human Health EffectsIon VasilescuNo ratings yet
- 7.4 Gas Exchange in Plants and Animals 2Document3 pages7.4 Gas Exchange in Plants and Animals 2yiuzz hcyNo ratings yet
- KOC - SA.007 - Entry Into Confined SpacesDocument19 pagesKOC - SA.007 - Entry Into Confined SpacesMahmoud Abdel DayemNo ratings yet
- Business Plan For Sleep CenterDocument59 pagesBusiness Plan For Sleep Centernajib batoNo ratings yet
- FNH 02Document6 pagesFNH 02karleth angelNo ratings yet
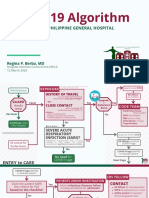
- COVID-19 Algorithm: For The Philippine General HospitalDocument10 pagesCOVID-19 Algorithm: For The Philippine General HospitalJay VeeNo ratings yet
- CPR Evaluation SheetDocument2 pagesCPR Evaluation SheetCatoNo ratings yet
- Laporan Kasus BronkopneumoniaDocument30 pagesLaporan Kasus BronkopneumoniaShifa Ali JannatinNo ratings yet
- rút gọnDocument3 pagesrút gọnUyen VuNo ratings yet
- ALS Ambulance Equipment ChecklistDocument4 pagesALS Ambulance Equipment ChecklistSunil KshetriNo ratings yet
- FELTP Progress Report 2020Document53 pagesFELTP Progress Report 2020ehsanlarikNo ratings yet