You might also like
- Nursing Research ProposalDocument36 pagesNursing Research ProposalSithara Jayatunga80% (5)
- Aquifer Case 16Document4 pagesAquifer Case 16Dina KristevaNo ratings yet
- 2 Medrega Cristian Gabriel enDocument1 page2 Medrega Cristian Gabriel enCristian GabrielNo ratings yet
- AAES Guidelines Thyroid PDFDocument73 pagesAAES Guidelines Thyroid PDFDana ChernovNo ratings yet
- Cadchart 2 PDFDocument2 pagesCadchart 2 PDFLouriel NopalNo ratings yet
- Tinnitus PDR Drug Interaction Guide 2009Document2 pagesTinnitus PDR Drug Interaction Guide 2009Avelox FloxNo ratings yet
- FDA Approval GuideDocument38 pagesFDA Approval GuideYuwono WibowoNo ratings yet
- 1992-1997 and 2004 Questions and AnswersDocument56 pages1992-1997 and 2004 Questions and AnswersEmad MerganNo ratings yet
- The Blood-Brain Barrier and Drug Delivery To The CNS - Begley, Bradbury, KreuterDocument247 pagesThe Blood-Brain Barrier and Drug Delivery To The CNS - Begley, Bradbury, KreuterFilip DrzazgaNo ratings yet
- Hyper & Hypothyroidism LectureDocument1 pageHyper & Hypothyroidism LectureJhevilin RMNo ratings yet
- Legal Aspects of Cosmetic Products: Development TeamDocument24 pagesLegal Aspects of Cosmetic Products: Development TeamkashishNo ratings yet
- Presented by Miss. Surita Ghosh Assistant Professor in Pharmaceutics SetgoiDocument37 pagesPresented by Miss. Surita Ghosh Assistant Professor in Pharmaceutics SetgoiSujanNo ratings yet
- Amboss:CardioDocument18 pagesAmboss:CardioNicole Juliette CCNo ratings yet
- Medical Council of Canada Evaluating Examination (MCCEE) Study GuideDocument20 pagesMedical Council of Canada Evaluating Examination (MCCEE) Study GuideMcRee Learning CenterNo ratings yet
- Physiology of PainDocument43 pagesPhysiology of PainNashwan ANo ratings yet
- Ventricular Isovolumetric Contractions: Tiara Calvo Leon, M.DDocument1 pageVentricular Isovolumetric Contractions: Tiara Calvo Leon, M.DSarah KhanNo ratings yet
- Nose To Brain (Physiology of Nose)Document26 pagesNose To Brain (Physiology of Nose)Soma YasaswiNo ratings yet
- Congenital Heart DefectsDocument6 pagesCongenital Heart DefectsJohiarra Madanglog TabigneNo ratings yet
- Back & Spine ConditionsDocument6 pagesBack & Spine ConditionsCarmela Beatriz SuelanNo ratings yet
- Internal Medicine Finals ReviewerDocument8 pagesInternal Medicine Finals ReviewerRojales FrancisNo ratings yet
- Cellulitis: Clinical Review: Be The First To CommentDocument9 pagesCellulitis: Clinical Review: Be The First To CommentAnonymous 1nMTZWmzNo ratings yet
- The Information About EDSDocument3 pagesThe Information About EDSAmber100% (1)
- Polio Virus: Department of Biotechnology Virology BT4168Document19 pagesPolio Virus: Department of Biotechnology Virology BT4168ariffdrNo ratings yet
- Nanomedicine-Based Approaches for the Treatment of DementiaFrom EverandNanomedicine-Based Approaches for the Treatment of DementiaRating: 5 out of 5 stars5/5 (1)
- NBME 11 Answers To All Sections 2Document97 pagesNBME 11 Answers To All Sections 2hussainalmusawiNo ratings yet
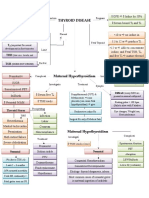
- Thyroid DiseaseDocument1 pageThyroid DiseaseZiyadNo ratings yet
- Lymphatic and Vascular System RehabDocument73 pagesLymphatic and Vascular System RehabWenzy Cruz100% (1)
- 8 BilirubinDocument25 pages8 BilirubinTagreed DerarNo ratings yet
- Basic Environmental Toxicology Problem SetDocument19 pagesBasic Environmental Toxicology Problem SetMimi Labindao100% (1)
- Biochemistry & Genetics Important Concepts Q&as DR Kumar Ponnusamy & Jegathambigai RN, Biochemistry & Genetics, International Medical University (IMU) / AIMST University School of Medicine, MalaysiaDocument60 pagesBiochemistry & Genetics Important Concepts Q&as DR Kumar Ponnusamy & Jegathambigai RN, Biochemistry & Genetics, International Medical University (IMU) / AIMST University School of Medicine, MalaysiaDr Kumar Ponnusamy100% (3)
- LMCC and Osce-Zu Hua PDFDocument270 pagesLMCC and Osce-Zu Hua PDFDaniel F100% (1)
- The Vascular System Doc TulaganDocument10 pagesThe Vascular System Doc Tulagankûrñï såñskrùthîNo ratings yet
- Antibiotics CasesDocument39 pagesAntibiotics CasesnistaneNo ratings yet
- Pharma Week 1-5Document25 pagesPharma Week 1-5Rachelle CambaNo ratings yet
- Bone TumorsDocument29 pagesBone TumorsmatameaNo ratings yet
- Occupational Lung DiseasesDocument75 pagesOccupational Lung DiseasesAnonymous h1XAlApsU100% (1)
- Adrenal and PheochromocytomaDocument86 pagesAdrenal and Pheochromocytomarajan kumar100% (1)
- Sysmex HemostasisDocument11 pagesSysmex HemostasisElyza L. de GuzmanNo ratings yet
- Personal Statement - FinalDocument2 pagesPersonal Statement - Finalapi-383932502No ratings yet
- Sigma Receptors Their Role in Disease and As Therapeutic Targets PDFDocument311 pagesSigma Receptors Their Role in Disease and As Therapeutic Targets PDFJohn Das100% (1)
- Endocrinology-II Past Papers 3rd Year-1Document11 pagesEndocrinology-II Past Papers 3rd Year-1Syed Muhammad HameemNo ratings yet
- Venous DiseaseDocument45 pagesVenous DiseaseNinch Nagac100% (1)
- Thyroid Hormones & Anti Thyroid AgentsDocument3 pagesThyroid Hormones & Anti Thyroid AgentsJaybee SarmientoNo ratings yet
- Cancer and EnvironmentDocument47 pagesCancer and Environmentandra1982No ratings yet
- Medicine Recommended Reading List ANUDocument2 pagesMedicine Recommended Reading List ANUYoussef LatashNo ratings yet
- Bioprocessing in The Pharmaceutical Industry: (An Engineering and Technological Overview)Document39 pagesBioprocessing in The Pharmaceutical Industry: (An Engineering and Technological Overview)ManchowNo ratings yet
- Environmental and Occupational ToxicantsDocument3 pagesEnvironmental and Occupational ToxicantsEhrli CuaresmaNo ratings yet
- Mock Record B-1-2-Well Child VisitsDocument4 pagesMock Record B-1-2-Well Child VisitsaelteeNo ratings yet
- LTF InterpretationDocument3 pagesLTF InterpretationkiethyanNo ratings yet
- The Gonadal Hormones & InhibitorsDocument41 pagesThe Gonadal Hormones & InhibitorsSaddamix AL OmariNo ratings yet
- NMS Surgery Casebook CH 1 Preoperative Care Flashcards - ProProfsDocument3 pagesNMS Surgery Casebook CH 1 Preoperative Care Flashcards - ProProfsWade Bullock0% (1)
- Pages From Grant-Kels - Color Atlas of DermatopathologyDocument5 pagesPages From Grant-Kels - Color Atlas of DermatopathologyamberwinthropNo ratings yet
- Lymphedema: Natthaphong Jirojananukul 4 Year Medical Student Phichit Medical CenterDocument26 pagesLymphedema: Natthaphong Jirojananukul 4 Year Medical Student Phichit Medical CenterPuthiput ChotsutaworakulNo ratings yet
- Practical Lab Manual of Pharmaceutical Organic Chemistry - 2Document117 pagesPractical Lab Manual of Pharmaceutical Organic Chemistry - 2Dhilip MuruganNo ratings yet
- Hematology & Oncology. Anatomy 56Document60 pagesHematology & Oncology. Anatomy 56Heran TeferiNo ratings yet
- 2022 Book CardiovascularCalcificationDocument294 pages2022 Book CardiovascularCalcificationDagoberto MunozNo ratings yet
- The Evolution of Antibiotic ResistanceDocument3 pagesThe Evolution of Antibiotic ResistancedndqdqNo ratings yet
- OsteoporosisDocument11 pagesOsteoporosisAdine Jeminah LimonNo ratings yet
- Aquifer Case 27Document4 pagesAquifer Case 27Dina KristevaNo ratings yet
- K - 8 Blood Brain Barrier (Biokimia)Document31 pagesK - 8 Blood Brain Barrier (Biokimia)Firman YunusNo ratings yet
- Table of Contents: Bacteria: Chapter 1: Gram Positive CocciDocument13 pagesTable of Contents: Bacteria: Chapter 1: Gram Positive CocciAnthony LNo ratings yet
- Trends in Drug ResearchDocument122 pagesTrends in Drug ResearchEvsevios HadjicostasNo ratings yet
- Harrison-Principals of Internal Medicine 20th. Ed. Prt.7-11Document707 pagesHarrison-Principals of Internal Medicine 20th. Ed. Prt.7-11Choi DongYiNo ratings yet
- Revision Guide - Biological Explanations of AggressionDocument6 pagesRevision Guide - Biological Explanations of Aggressionvtina177220No ratings yet
- Transurethral Resection (TUR)Document1 pageTransurethral Resection (TUR)vtina177220No ratings yet
- Cross Tab: Case Processing SummaryDocument4 pagesCross Tab: Case Processing Summaryvtina177220No ratings yet
- Pertumbuhan Dan Perkembangan Pada Masa Remaja: Febe Ardilla Valentina Kaesmetan 102012330Document26 pagesPertumbuhan Dan Perkembangan Pada Masa Remaja: Febe Ardilla Valentina Kaesmetan 102012330vtina177220No ratings yet
- Enlg Argumenative Essay 1Document15 pagesEnlg Argumenative Essay 1aishazariya02No ratings yet
- Cyanobacteria: Cyanobacteria - Wikipedia, The Free EncyclopediaDocument9 pagesCyanobacteria: Cyanobacteria - Wikipedia, The Free EncyclopediaRavindraNo ratings yet
- DENGUE FEVER Test Report Format Example Sample Template Drlogy Lab ReportDocument1 pageDENGUE FEVER Test Report Format Example Sample Template Drlogy Lab ReportBhojraj SinghNo ratings yet
- Rep. Adam Schiff Letter To AmazonDocument3 pagesRep. Adam Schiff Letter To AmazonGeekWireNo ratings yet
- Magnetom Essenza: Established 1.5T Performance. With Tim+DotDocument26 pagesMagnetom Essenza: Established 1.5T Performance. With Tim+DotFrank OforiNo ratings yet
- To Study The Development of Cockroach 1.0Document6 pagesTo Study The Development of Cockroach 1.0Utkarsh MishraNo ratings yet
- My MRIDocument58 pagesMy MRIapi-26159412100% (1)
- Nursing Care Plan For Peds Diabetes InsipidusDocument5 pagesNursing Care Plan For Peds Diabetes Insipidusapi-307733298100% (1)
- Stroke Guidelines 20190724Document40 pagesStroke Guidelines 20190724Виктория МатяшNo ratings yet
- Food SanitationDocument33 pagesFood SanitationOlive FactorizaNo ratings yet
- Prospects For Increaing Commercial Mushroom Production in Malaysia: Challenge and OpportunitiesDocument11 pagesProspects For Increaing Commercial Mushroom Production in Malaysia: Challenge and OpportunitiesHahaNo ratings yet
- Chapter 1 Aloe Vera Face and Body Scrub 2018Document4 pagesChapter 1 Aloe Vera Face and Body Scrub 2018hopeNo ratings yet
- Buah SirsakDocument12 pagesBuah SirsakAHllaqi F SeieiNo ratings yet
- 25 Amazing Benefits and Uses of Jackfruit: Vineetha FruitsDocument10 pages25 Amazing Benefits and Uses of Jackfruit: Vineetha FruitsMohd Idris MohiuddinNo ratings yet
- Significance of The StudyDocument5 pagesSignificance of The StudyMaria Paula Nebria GalichaNo ratings yet
- Hypertension WordDocument8 pagesHypertension WordAllan Alejandro SevillaNo ratings yet
- Middle Cerebral ArteryDocument4 pagesMiddle Cerebral Arterykat9210No ratings yet
- Basic Psychology Lec. Notes FinalDocument134 pagesBasic Psychology Lec. Notes FinalPhilip Mutua100% (1)
- Cerebral Palsy An Information Guide For ParentsDocument36 pagesCerebral Palsy An Information Guide For Parentsraquelbibi100% (1)
- Final Research Paper On Childhood ObesityDocument4 pagesFinal Research Paper On Childhood Obesityafmcpdbnr100% (1)
- Normal Personality Trait and Dark TriadDocument9 pagesNormal Personality Trait and Dark TriadSakina Nusarifa TantriNo ratings yet
- Sample: Patient Safety in Healthcare, Forecast To 2022Document20 pagesSample: Patient Safety in Healthcare, Forecast To 2022Rolando PinchettiNo ratings yet
- HCC Software V1213.70.J1 DescriptionDocument6 pagesHCC Software V1213.70.J1 DescriptionPassFam14No ratings yet
- Serous Otitis MediaDocument21 pagesSerous Otitis Mediagiri00767098No ratings yet
- Step Down RN or Progressive Care Skills ChecklistDocument4 pagesStep Down RN or Progressive Care Skills Checklisthealth careNo ratings yet
- Presentation List Language Disorders in ChildrenDocument3 pagesPresentation List Language Disorders in Childrenramandeep kaurNo ratings yet
- Biology Contents - RPSC FSO by Food TecKnowDocument35 pagesBiology Contents - RPSC FSO by Food TecKnowRahul JainNo ratings yet