Professional Documents
Culture Documents
Management of TMD
Management of TMD
Uploaded by
Wallisson SoaresCopyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
Management of TMD
Management of TMD
Uploaded by
Wallisson SoaresCopyright:
Available Formats
Journal of Oral Rehabilitation
Journal of Oral Rehabilitation 2010 37; 430–451
Review Article
Management of TMD: evidence from systematic reviews and
meta-analyses
T. LIST* & S. AXELSSON† *Department of Stomatognathic Physiology, Faculty of Odontology, Malmö University, Malmö and
†
The Swedish Council on Technology Assessment in Health and Care, Stockholm, Sweden
SUMMARY This systematic review (SR) synthesises control studies, and nine were a mix of RCTs and
recent evidence and assesses the methodological case series. Most SRs had pain and clinical measures
quality of published SRs in the management of as primary outcome variables, while few SRs
temporomandibular disorders (TMD). A systematic reported psychological status, daily activities, or qual-
literature search was conducted in the PubMed, ity of life. There is some evidence that the following
Cochrane Library, and Bandolier databases for 1987 can be effective in alleviating TMD pain: occlusal
to September 2009. Two investigators evaluated the appliances, acupuncture, behavioural therapy, jaw
methodological quality of each identified SR using exercises, postural training, and some pharmacolog-
two measurement tools: the assessment of multiple ical treatments. Evidence for the effect of electro-
systematic reviews (AMSTAR) and level of research physical modalities and surgery is insufficient, and
design scoring. Thirty-eight SRs met inclusion crite- occlusal adjustment seems to have no effect. One
ria and 30 were analysed: 23 qualitative SRs and limitation of most of the reviewed SRs was that the
seven meta-analyses. Ten SRs were related to occlu- considerable variation in methodology between the
sal appliances, occlusal adjustment or bruxism; eight primary studies made definitive conclusions impos-
to physical therapy; seven to pharmacologic treat- sible.
ment; four to TMJ and maxillofacial surgery; and six KEYWORDS: systematic review, randomised clinical
to behavioural therapy and multimodal treatment. trial, evidence-based medicine, treatment, assess-
The median AMSTAR score was 6 (range 2–11). ment
Eighteen of the SRs were based on randomised
clinical trials (RCTs), three were based on case– Accepted for publication 8 March 2010
read about 17–20 original articles – as a daily average
Background
(7).
Population-based studies among adults report that Systematic reviews (SRs) are a cornerstone in evi-
approximately 10–15% have temporomandibular dis- dence-based medicine. An SR is a compilation of all
orders (TMD) pain and 5% a perceived need for published research that addresses a carefully formulated
treatment (1, 2). Several studies have pointed out that question. Research results are collected based upon pre-
persistent and recurrent pain has a potential impact on determined inclusion and exclusion criteria; data are
daily life – mainly in the areas of psychological critically analysed and synthesised so that evidence-
discomfort, physical disability, and functional limita- based conclusions on the benefit or risks of different
tions – which leads to limitations in quality of life (3–6). methods can be drawn, with the final goal to improve
Keeping current on new developments in a medical patient care. An SR may have a qualitative approach if
or dental field is often an imposing task for researchers data from the primary studies are presented descriptively
and clinicians. One researcher estimated that to keep or a quantitative approach if statistical analysis has
abreast of developments in his field, he would need to combined data in a meta-analysis. Of the over 24
ª 2010 Blackwell Publishing Ltd doi: 10.1111/j.1365-2842.2010.02089.x
MANAGEMENT OF TMD 431
instruments that have been developed to assess SR
Inclusion criteria
quality, one recent instrument deserves mention: assess-
ment of multiple systematic reviews (AMSTAR) (8). This Besides the database search criteria listed previously,
tool comprises 11 items and has good face and content the selected articles must:
validity for measuring methodological quality (9). 1 Be an SR
This systematic review of published SRs that survey 2 Focus on the management of TMD treatment
TMD management efficacy adds to these existing Systematic reviews that covered oro-facial pain or
reviews by (i) synthesising recent evidence and (ii) TMD prevention besides TMD treatment effect were
assessing SR methodological quality. included.
Methods Exclusion criteria
1 Dual publication
Procedure
2 Update of the SR by the same author in a later
Both authors selected the articles based on inclusion publication
and exclusion criteria and independently read all titles 3 SR of orthodontic treatment focusing on develop-
and abstracts that were found in multiple searches to ment and not treatment of TMD
identify potentially eligible articles for inclusion. All 4 Systematic reviews of SRs
potentially eligible SRs were then retrieved, and full-
text articles were reviewed to determine whether they
Quality assessment
met inclusion criteria. Disagreement was resolved by
discussion among the investigators. Authors were not Two instruments were used to assess the methodolog-
contacted for missing information. The reviewers were ical quality of the SRs: (i) AMSTAR and (ii) LRD.
experienced oro-facial pain specialist clinicians or Shea et al. developed AMSTAR by evaluating the
methodologists in evidence-based medicine. importance of 37 items commonly used in SR assess-
The investigators independently evaluated the ment and reducing these items to an 11-item instru-
methodological quality of each identified SR using ment that addresses key domains in methodological
AMSTAR and level of research design (LRD) scoring. qualities (8). Assessment of multiple systematic
The following data were extracted: study design, diag- reviews is reported to have good face and content
nosis, number of patients, types of intervention, outcome validity (9).
measures, results, quality score, and author’s conclusion. Assessment of multiple systematic reviews appraises
these key items:
1 Was an á priori design provided?
Database search
2 Was there duplicate study selection and data extrac-
The search encompassed all the articles that were (i) tion?
indexed in PubMed, the Cochrane Library, and Bando- 3 Was a comprehensive literature search provided?
lier, (ii) published in English, Swedish, or German, and 4 Was the status of publication (i.e. grey literature)
(iii) published between 1 January 1987 and 8 September used as an inclusion criterion?
2009. The search strategy was designed to identify SRs 5 Was a list of studies (included and excluded)
that focused on TMD management. The following search provided?
terms were used for PubMed: Craniomandibular disor- 6 Were the characteristics of the included studies
ders ⁄ drug therapy [MeSH] OR Craniomandibular disor- provided?
ders ⁄ surgery [MeSH] OR Craniomandibular 7 Was the scientific quality of the included studies
disorders ⁄ surgery [MeSH] AND ‘‘Review’’ AND Meta- assessed and documented?
analysis [MeSH] AND ‘‘Systematic review’’. For Coch- 8 Was the scientific quality of the included studies
rane Library, the search strategy included the terms used appropriately in formulating conclusions?
craniomandibular disorders and temporomandibular 9 Were the methods used to combine the findings of
joint (TMJ). References in original articles and SRs were studies appropriate?
hand-searched to identify additional SRs. 10 Was the likelihood of publication bias assessed?
ª 2010 Blackwell Publishing Ltd
432 T. LIST & S. AXELSSON
11 Was the conflict of interest stated? Computerised search of databases,
Each of these 11 items was scored as ‘Yes’, ‘No’, reference checking, abstracts:
‘Can’t answer’, or ‘Not applicable’. PubMed: 602 references
Cochrane library: 19 references
The LRD assesses internal validity of the primary Bandolier: 1 reference
studies based on design. The research design levels are Handsearch: 3 references
structured hierarchically according to evidence strength 625 references
(10):
1 Systematic review of randomised clinical trials (RCTs) Abstracts excluded:
2 Randomised clinical trial 587 references
3 Study without randomisation, such as a cohort study,
case–control study
Screening of articles applying
4 A non-controlled study, such as cross-sectional study, inclusion criteria:
case series, case reports 38 references
5 Narrative review or expert opinion
Reliability of quality assessment Abstracts excluded:
8 references
(11–18)
Both authors independently assessed SR quality to
determine inter-test reliability. The inter-reliability of
Articles included for quality
the two authors in assessing the quality of the SRs was assessment:
calculated with kappa-statistics. All articles were dis-
30 references
cussed to verify appraisal process until consensus was (19–47, 65)
(23) reported two SRs
reached. Disagreements on individual item scores were
resolved with discussion. Fig. 1. Flow diagram of references included and excluded in the
systematic review.
Results
tenderness ⁄ pain on palpation, and 10 of the SRs
Thirty-eight SRs were read in full text; 30 of these were included measures of psychological status, daily activ-
included in this SR: 23 were qualitative SRs and seven ities, or quality of life. The median AMSTAR score was 6
were meta-analyses. Eight SRs were excluded after (range 2–11). The LRD scores for the SRs are as follows:
reading because upon closer scrutiny, they did not fulfil
the inclusion criteria: three SRs had been updated in Level I–II 2 SRs
more recent SRs by the same author (11–13), one study Level I-III 1 SR
did not focus on TMD management (14), two SRs Level II 16 SRs
Level II–III 1 SR
focused on development of TMD following orthodontic
Level III 1 SR
intervention (15, 16), and two SRs were SRs of SRs (17, Level II–IV 9 SRs
18) (Fig. 1).
Tables 1–5 list characteristics and assess quality of the
included SRs. Although the most common diagnosis in The SRs were divided into five treatment groups:
the SRs was TMD, more specific TMD diagnoses such as 1 Occlusal appliances, occlusal adjustment, and bruxism
disc displacements and myofascial pain were sometimes 2 Physical treatment [acupuncture, transcutaneous
also reported. Two SRs focused on bruxism. Although it electrical nerve stimulation (TENS), exercise, and
is in the TMD domain, bruxism differs from other TMD mobilisation]
diagnoses: although it may be accompanied by pain, 3 Pharmacologic treatment
bruxism is not related to pain in many cases. The 4 TMJ and maxillofacial surgery
number of patients ranged from 0 to 7173 in the SRs. 5 Behavioural therapy and multimodal treatment
Twenty-nine SRs had pain intensity or pain reduction Ten SRs evaluated occlusal appliances, occlusal
as primary outcome measures, 25 of the SRs reported adjustment, or bruxism (Table 1). Eight of these con-
clinical outcome measures such as jaw movement and cerned TMD treatment (12, 19–26), one the effect of
ª 2010 Blackwell Publishing Ltd
Table 1. Characteristics of systematic reviews (SRs) of occlusal appliances, occlusal adjustment, and orthodontic treatment
Study design, Intervention (I)
Authors, year, diagnosis, and and control (C) Outcome Quality Authors’ (A) conclusions
reference no. of patients groups measures Results score Reviewers’ (R) comments
Santacatterina A SR and I1: Occlusal Pain reduction I2 better than I1 AMSTAR 2 A: A comparison between the two kinds of
1998 (25) Meta-analysis of appliance TMJ click for pain reduction LRD II-IV treatment has demonstrated that the
ª 2010 Blackwell Publishing Ltd
6 RCTs I2: repositioning and TMJ click. repositioning splint is more effective both in the
Disc displacement splint resolution of the articular click and in the
with reduction resolution of the pain (P < 0Æ001).
212 patients R: Methodological weaknesses of primary studies
such as heterogeneous patient material, outcome
measures not clearly defined, and three of the
studies were not RCTs.
Al-Ani MZ Qualitative SR of I1: Occlusal Pain reduction I1 no better than C1 AMSTAR 6 A: There is insufficient evidence either for or
2003 (19) 12 RCTs appliance Jaw motion I1 somewhat better LRD II against the use of stabilisation splint therapy over
Myofascial pain C1: Other treatment than C2 other active interventions for the treatment of
496 patients (biofeedback, jaw I1 no better than C3 temporomandibular myofascial pain. However,
exercises, it appears that stabilisation splint therapy may be
acupuncture) beneficial for reducing pain severity at rest and on
C2: No treatment palpation and depression when compared to no
C3: Placebo treatment.
R: Included studies were small. Patient material
was heterogeneous. Outcome measures varied
between studies. Short-term follow-up.
Exclusion, inclusion, and diagnostic criteria
not clearly defined.
Forssell H Qualitative I1: Occlusal Pain reduction Contradictory AMSTAR 7 A: Occlusal splints yielded equivocal results. Even
2004 (20) SR of 20 RCTs appliance Global results for I1 LRD II for the most studied area, stabilisation splints for
TMD I2: Occlusal improvement compared with myofascial pain, the results do not justify definite
1138 patients adjustment Clinical C1–C3 conclusions about the efficacy of splint therapy.
C1: Other treatment examination I2 no better than Their clinical effectiveness to relieve pain also
(biofeedback, jaw Depression scale C1 or C2 seems modest when compared with treatment
exercises, methods in general. None of the occlusal
acupuncture) adjustment studies provided evidence supporting
C2: No treatment the use of this treatment method.
C3: Placebo R: Included studies small, often not blinded,
heterogeneity concerning outcome measures and
control treatment.
MANAGEMENT OF TMD
433
434
Table 1. (Continued)
Study design, Intervention (I)
Authors, year, diagnosis, and and control (C) Outcome Quality Authors’ (A) conclusions
reference no. of patients groups measures Results score Reviewers’ (R) comments
Türp JC Qualitative I1: Intra-oral Pain reduction I1 better than C2 AMSTAR 6 A: Based on the currently best available evidence,
2004 (21) SR of 9 RCTs appliance Clinical I1 no better than C1 LRD II it appears that most patients with masticatory
T. LIST & S. AXELSSON
Myofascial pain C1: Other treatment examination muscle pain are helped by incorporation of a
482 patients including placebo Depression scale stabilisation splint. A stabilisation splint does not
C2: No treatment appear to yield a better clinical outcome than a
soft splint, a non-occluding palatal splint, physical
therapy, or acupuncture.
R: Well-conducted SR. Limitations: small patient
studies, outcome measures vary between studies,
no long-term results.
Fricton J Qualitative I1: Stabilisation Pain reduction No difference AMSTAR 4 A: Stabilisation splints can reduce TMD pain
2006 (22) SR of 39 RCTs splint between I1 and I2. LRD II compared to placebo splints. Stabilisation splints
TMD I2: Anterior I1 and C2 have are equally effective in reducing pain compared to
patients* positioning and similar effects physical therapy, acupuncture and behavioural
soft splints I2, I1, and C1 have therapy in the short term. The long-term effects of
C1: Placebo similar effects behavioural therapy may be better than splints in
C2: Other treatment reducing symptoms in more severe patients with
psychosocial problems.
R: The article is an overview and separate articles
are under publishing with details regarding
methods and results.
SBU Qualitative I1: Stabilisation Pain reduction I1 better than C3 AMSTAR 6 A: Occlusal appliances gave better pain reduction
2006 (23) SR of 3 SRs and splint Clinical I1 and C2 have LRD I–II than no treatment. Treatment with occlusal
3 RCTs I2: Occlusal examination similar effect appliance had similar effect as other therapies
TMD adjustment Depression scale Results of I1 whereas the effect compared with placebo was
2299 patients C1: Placebo compared with C1 contradictory. No study found occlusal
C2: Other are contradictory adjustment to be effective compared to a control.
treatments I2 and C1 have R: Reviewers and authors are identical persons
C3: No treatment similar effect
ª 2010 Blackwell Publishing Ltd
Table 1. (Continued)
Study design, Intervention (I)
Authors, year, diagnosis, and and control (C) Outcome Quality Authors’ (A) conclusions
reference no. of patients groups measures Results score Reviewers’ (R) comments
Stapelman H Qualitative I1: NTI splint EMG activity Reducing EMG AMSTAR 7 A: NTI-tss devices may be successfully used to
2008 (24) SR of 5 RCTs C1: Flat occlusal Polysomnographic activity: I1 more LRD II manage bruxism and TMDs. To avoid potential
ª 2010 Blackwell Publishing Ltd
TMD splint evaluation effective than C1 unwanted effects, it should be chosen only if a
Bruxism C2: Bleaching tray Pain intensity Improvement in patient will be compliant with follow-up. Two of
Tension-type Jaw opening pain reduction: five studies focused on treatment of TMD.
headache (TTH) Comfort results for I1 Overall, small groups, median of 14 participants
Migraine Analgesic compared with C1 in each group. As adverse events were reported
190 patients consumption are contradictory for I1, and I1 was not more effective than C1,
Treating TTH and only limited indication is warranted.
migraine: I1 more R: Well-conducted SR. Limitations are small
effective than C2 studies. Methodological weaknesses in primary
Five reports of studies such as heterogeneity concerning
complications or outcome measures and diagnostic criteria.
side-effects
reported for I1
Koh H SR and I1: Occlusal Global symptoms No difference AMSTAR 10 A: There is an absence of evidence, from RCTs, that
2009 (26) meta-analysis adjustment Relief of headache between I1 and C1 LRD II occlusal adjustment treats or prevents TMD.
of 6 RCTs C1: Placebo, no Quality of life Occlusal adjustment cannot be recommended for
TMD treatment or management or prevention of TMD.
392 patients reassurance R: Small studies, diagnostic criteria inaccurate.
Outcome measures poorly defined.
Marcedo CR SR and I1: Occlusal splint Sleep variables: e.g. No difference AMSTAR 9 A: There is not sufficient evidence to state that the
2009 (27) meta-analysis I2: Other appliances EMG activity, between I1 and I2 LRD II occlusal splint is effective for treating sleep
of 5 RCTs I3: Other therapies arousal index in the bruxism. Indication of its use is questionable
Bruxism C1: No treatment Report of bruxism meta-analysis of concerning sleep outcomes, but it may be that
63 patients by partner arousal index. there are some benefits concerning tooth wear.
Tooth wear No difference R: Small studies, methodological weaknesses in
between I1 and C1 primary studies
for tooth wear
facets
No difference
between I1 and I3
for TMD pain
MANAGEMENT OF TMD
435
436 T. LIST & S. AXELSSON
occlusal appliances on sleep bruxism (27), and one the
devices. In a case series of patients with severe
A: One study was prospective and reported less
attrition in young children wearing bite plates
R: Small studies, methodological weaknesses in
effect of occlusal appliances on attrition (28). Six SRs
primary studies. The results seem to confirm
attrition, occlusal splints were found to slow
compared with subjects who did not wear
reported that occlusal appliances and other therapies
had similar effect, three that occlusal appliances were
better than no treatment, and four that there was no
AMSTAR, assessment of multiple systematic reviews; LRD, level of research design; NTI, nociceptive trigeminal inhibition; RCT, randomised clinical trial; TMD,
difference between occlusal appliances and non-occlud-
down the rate of tooth wear.
ing splints (placebo). One SR reported stabilisation
Reviewers’ (R) comments
Authors’ (A) conclusions
splints and anterior positioning and soft splints to yield
similar results, while one SR reported anterior posi-
clinical experience.
tioning splints to be more effective than stabilisation
splints. One SR reported contradictory results in a
comparison of nociceptive trigeminal inhibition (NTI)
splints and occlusal appliances. Several complications
and adverse events were documented for the NTI-tss
device. Three SRs reported no difference in outcome
between occlusal adjustments and control treatment.
AMSTAR 6
LRD II-IV
Eight SRs evaluated various physical treatments in
Quality
patients with TMD (Table 2). Of these SRs, six assessed
score
acupuncture (23, 29–32), three jaw exercises (23, 33,
34), two manual therapy (33, 34), and three various
forms of electrical therapy (30, 34). Three SRs reported
compared with C1.
I1 reduces attrition
that acupuncture was better than no treatment, four
SRs that acupuncture and other therapies yielded
similar results, and one SR that acupuncture and
Results
placebo treatment had similar results. Two SRs found
no support for acupuncture treatment.
As for the other types of physical treatment, three
SRs reported that jaw exercises were better than
measures
Outcome
Attrition
controls, and two SRs found postural training to be
better than no treatment. No SR indicated that electro-
physical modalities such as TENS, laser, and ultrasound
were effective in reducing pain.
C1: no treatment
Intervention (I)
and control (C)
Seven SRs evaluated various pharmacological treat-
I1: Occlusal
ments in patients with TMD, atypical facial pain,
appliance
trigeminal neuralgia, and burning mouth syndrome
groups
(23, 35–40) (Table 3). One SR reported anti-epileptic
drugs to be more effective than placebo in patients
with trigeminal neuralgia. In patients with TMD,
2 studies related to
and 1 case series.
pharmacological treatment that was found to be more
SR of 33 studies
bruxism. 1 RCT
no. of patients
diagnosis, and
effective than placebo was analgesics (two SRs),
Intervention
*Number of patients not reported.
Study design,
because of
27 patients
Qualitative
clonazepam or diazepam (three SRs), antidepressants
temporomandibular disorders.
(four SRs), and hyaluronate (one SR). This last SR also
reported hyaluronate and glycocorticoid to produce a
Table 1. (Continued)
similar effect. Three SRs reported amitriptyline to have
a moderate effect in patients with atypical facial pain.
van¢t Spijker A
Authors, year,
Two SRs reported the use of botulinum toxin in
2007 (28)
reference
patients with pain or masseter hypertrophy. One SR
reported positive outcome based upon one RCT,
whereas the other SR found no studies that met its
ª 2010 Blackwell Publishing Ltd
Table 2. Characteristics of systematic reviews (SRs) of physical therapy: acupuncture, TENS, exercise, and mobilisation
Study design, Intervention (I)
Authors, year, diagnosis, and and control (C) Outcome Quality Authors’ (A) conclusions
reference no. of patients groups measures Results score Reviewers’ (R) comments
Ernst E Qualitative I1: Acupuncture Pain Intensity I1 better than C2 AMSTAR 5 A: Although all studies agree with the notion that
1999 (29) SR of 6 RCTs C1: Occlusal Daily activity No difference LRD II acupuncture is effective for TMD, this hypothesis
TMD appliance Global between I1 and C1 requires confirmation through more rigorous
ª 2010 Blackwell Publishing Ltd
205 patients C2: No treatment improvement investigations.
Clinical R: Short follow-up time in two studies. One study
examination reports a 1-year follow-up. No reported side-effects.
SR based on three studies with low quality.
Jedel E Qualitative I1: Biofeedback Self-reported No evidence of an AMSTAR 3 A: The studies were heterogeneous with low quality,
2003 (30) SR of 7 RCTs I2: Acupuncture symptoms effect for any LRD II and therefore it is not possible to draw any
TMD I3: TENS Pain intensity treatment mode conclusions.
379 patients C1: No treatment Clinical R: Limitations in the SR methodology and therefore
C2: Other treatment examination difficult to draw any conclusions
Rosted P Qualitative I1: Acupuncture Pain intensity No difference AMSTRAR 4 A: Acupuncture and conventional treatment were
1998 (31) SR of 15 RCTs C1: Other treatment between I1 and C1 LRD II-IV found to have similar effect. The effect in treating
(7 RCTs on TMD) TMD and facial pain seems real, and acupuncture
Acute toothache could be an alternative to conventional treatment.
TMD R: Non-RCTs were included in the evaluation.
patients* Methodology and results not clearly described.
SBU Qualitative I1: Acupuncture Pain intensity I1 better than C3 AMSTAR 6 A: Acupuncture was found to show better pain
2006 (23) SR of 3 C1: Placebo Daily activities I1 and C2 have LRD I–II reduction than no treatment and similar effect
SRs and 1 RCT acupuncture Global similar effect compared to other treatments. Compared to placebo,
TMD C2: Other treatment improvement I1 and C1 have the results are contradictory.
575 patients C3: No treatment Clinical contradictory R: Reviewers and authors are identical persons
examination results
SBU Qualitative I1: Jaw exercises Pain intensity I1 better than C1 AMSTAR 6 A: The evidence to draw any conclusions regarding
2006 (23) SR of 6 RCTs I2: Pulsed radio Daily activities I1–I4 no different LRD I–II physical treatment for TMD is insufficient because
TMD frequency therapy Clinical from C2 the studies are heterogeneous regarding diagnosis
279 patients I3: Laser examination I5 better than C3 and treatment method.
I4: Pulsed R: Some of the studies showed a difference compared
electromagnetic with controls. Because these findings were not
fields supported by more studies, there is lack of evidence.
I5: Postural Reviewers and authors are identical persons
correction
C1: Minimal
information
C2: Placebo
C3: No treatment
MANAGEMENT OF TMD
437
438
Table 2. (Continued)
Study design, Intervention (I)
Authors, year, diagnosis, and and control (C) Outcome Quality Authors’ (A) conclusions
reference no. of patients groups measures Results score Reviewers’ (R) comments
Fink M Qualitative I1: Acupuncture Pain intensity I1 and C2 have AMSTAR 7 A: The analysed studies on acupuncture in the
2006 (32) SR of 6 RCTs C1: Sham Global similar effects LRD II treatment of TMD confirm acupuncture to be as
TMD acupuncture improvement No difference effective as conservative treatment.
223 patients C2: Other treatment Daily activities between I1 and C1 R: Short follow-up time in three studies. One study
C3: No treatment Clinical reports a 1-year follow-up. No reported side-effects.
T. LIST & S. AXELSSON
examination SR based on three studies with low and one with
Pain thresholds high quality.
McNeely M Qualitative I1: Exercise and Pain reduction No synthesis of AMSTAR 7 A: The results support use of active and passive oral
2006 (33) SR of 12 RCTs manual therapy Jaw mobility results LRD II exercises and exercises to improve posture as
TMD I2: Acupuncture effective interventions to reduce symptoms
480 patients I3: Electrophysical associated with TMD. There is inadequate
modalities (PRFE, information to either support or refute use of
TENS, biofeedback, acupuncture in TMD treatment. There is no evidence
laser) to support use of electrophysical modalities to reduce
C1: Other therapies TMD pain.
C2: Placebo R: Methodological weaknesses of primary studies such
as diagnostic criteria of TMD, outcome measures and
chosen controls limit conclusions in the study.
Medlicott MS Qualitative I1: Exercise Pain intensity No synthesis of AMSTAR 5 A: Active exercise and manual mobilisation may be
2006 (34) SR of 24 RCTs I2: Manual therapy Global results LRD II-IV effective. Postural training may be used in
and 6 uncontrolled I3: Electrotherapy improvement combination with other interventions, as
studies (ultrasound, TENS, Clinical independent effects of postural training are
TMD laser, PRFE) examination unknown. Mid-laser therapy may be more effective
1071 patients I4: Relaxation Jaw mobility than other electrotherapy modalities. Programmes
training and Pressure pain involving relaxation techniques and biofeedback,
education threshold electromyographic training, and proprioceptive
C1: Occlusal splint re-education may be more effective than placebo
C2: Placebo treatment or occlusal splints. Combinations of active
C3: Waiting-list exercise, manual therapy, postural correction, and
relaxation techniques may be effective.
R: Because of the heterogeneous population and to
differences in diagnosis and outcome measures, it not
possible to draw any clear conclusions from this SR.
TENS, transcutaneous electric nerve stimulation; PRFE, pulsed radio frequency energy; AMSTAR, assessment of multiple systematic reviews; LRD, level of research design; RCT,
randomised clinical trials; TMD, temporomandibular disorders.
ª 2010 Blackwell Publishing Ltd
Table 3. Characteristics of systematic reviews (SRs) of pharmacologic treatment
Study design, Intervention (I)
Authors, year, diagnosis, and and control (C) Outcome Quality Authors’ (A) conclusions
reference no. of patients groups measures Results score Reviewers’ (R) comments
ª 2010 Blackwell Publishing Ltd
Sommer C Qualitative I1: Carbamazepin, Pain reduction Trigeminal neuralgia: AMSTAR 4 A: Apart from studies on trigeminal neuralgia,
2002 (35) SR of 27 RCTs baclofen, >50% I1 significantly better LRD II there is little evidence for pharmacotherapy in
TMD, trigeminal lamotrigine than C1 oro-facial pain.
neuralgia, atypical I2: Clonazepam, TMD: moderate R: Some of the studies showed a difference
facial pain Diazepam evidence that I2 and compared with controls. Limitations in the
931 patients I3: Amitriptyline I3 are better than C1 primary studies were small groups,
C1: Placebo Atypical facial pain: a heterogeneous outcome measures, and no
moderate effect of I3 long-term follow-up.
compared with C1
List T Qualitative I1: Analgesics Pain reduction TMD and atypical AMSTAR 7 A: The common use of analgesics in TMD, AFP,
2003 (36) SR of 11 RCTs I2: Antidepressants Global facial pain: few LRD II and BMS is not supported by scientific
TMD, atypical I3: Benzodiazepines improvement studies found better evidence.
facial pain, I4: Miscellaneous Depression scale effect of I1-I4 R: The studies are too heterogeneous to draw
burning mouth (corticosteroids, compared with C1 any conclusions from.
syndrome sodium Burning mouth:
368 patients hyaluronate, I2 = C1
sumatriptan,
cocaine)
C1: Placebo
SBU Qualitative I1: Analgesics Pain reduction TMD and atypical AMSTAR 6 A: Studies on pharmacological treatment of
2006 (23) SR of 1 SR and I2: Antidepressants facial pain: few LRD I–II TMD, atypical facial pain, and burning mouth
13 RCTs I3: Benzodiazepines studies found better syndrome report contradictory results.
TMD, atypical I4: Miscellaneous effect of I1–I4 No conclusions can be drawn as the studies are
facial pain, (corticosteroids, compared with C1 heterogeneous regarding diagnosis and
burning mouth sodium For burning mouth, treatment method.
syndrome hyaluronate, I = C1 R: Reviewers and authors are identical persons
968 patients sumatriptan,
capsaicin,
botulinum toxin)
C1: Placebo
MANAGEMENT OF TMD
439
440
Table 3. (Continued)
Study design, Intervention (I)
Authors, year, diagnosis, and and control (C) Outcome Quality Authors’ (A) conclusions
reference no. of patients groups measures Results score Reviewers’ (R) comments
Shi ZC SR and I1: Hyaluronate Symptoms Long-term effects AMSTAR 11 A: There is insufficient consistent evidence to
2009 (37) meta-analysis I2: Hyaluronate + (e.g. pain, favour I1 compared LRD II support or refute the use of hyaluronate for
of 7 RCTs Arthroscopy ⁄ lavage Clinical to C1 treating patients with TMD.
TMD, rheumatoid C1: Placebo examination I1 had the same R: Methodological weaknesses of primary
arthritis C2: Glycocorticoid Adverse events long-term effects on studies such as diagnostic criteria of TMD and
364 patients C3: Arthroscopy ⁄ lavage symptoms and clinical outcome measures in the study.
T. LIST & S. AXELSSON
signs compared to C2
Comparing I1 to C3,
results were
inconsistent
Al-Muharraqi MA SR and I1: Botulinum toxin Self-reported 167 references were AMSTAR 7 A: No randomised trial on the efficacy of
2009 (38) meta-analysis of C1: Placebo facial retrieved, but none LRD II intra-muscular injections of botulinum toxin
RCTs appearance matched the with bilateral benign masseter hypertrophy
No studies Pain and inclusion criteria. was identified.
included discomfort R: No trend of the effect can be drawn because
Masseter all studies were excluded.
hypertrophy
0 patients
Cascos-Romero J Qualitative I1: Antidepressants Pain I1 better than C1 AMSTAR 4 A: The use of tricyclic antidepressants for the
2009 (39) SR of 1 SR, C1: Placebo LRD I–III treatment of TMD is recommended.
1 RCT and 1 R: Synthesis of results from primary studies are
case–control study missing, and therefore, because of limitations
TMD in the SR, it is difficult to draw any
patients* conclusions.
Ihde S 2007 (40) Qualitative I1: Botulinum toxin Pain reduction I1 better than C1 for AMSTAR 3 A: Botulinum toxin appears relative safe and
SR of 1 RCT and C1 Placebo Jaw opening reducing pain based LRD II-IV effective in treating chronic facial pain
10 case series Functional on one RCT. associated with masticatory hyperactivity.
TMD improvement No synthesis of R: Methodological limitations in the SR.
Bruxism Aesthetic result results. Results only relate to one RCT study.
Masseter Synthesis of results missing so a conclusion of
hypertrophy the effect of Botulinum toxin is difficult to
Oro-mandibular determine
dystonia
402 patients
AMSTAR, assessment of multiple systematic reviews; LRD, level of research design; RCT, randomised clinical trials; TMD, temporomandibular disorders.
*Number of patients not reported.
ª 2010 Blackwell Publishing Ltd
Table 4. Characteristics of systematic reviews (SRs) of the TMJ and maxillofacial surgery
Study design,
Authors, year, diagnosis, and Intervention (I) and Outcome Quality Authors’ (A) conclusions
reference no. of patients control (C) groups measures Results score Reviewers’ (R) comments
ª 2010 Blackwell Publishing Ltd
Reston JT SR and I1: Arthrocentesis Pain reduction Disc displacement AMSTAR 4 A: Surgical treatment appears to provide some
2003 (41) meta-analysis of I2: Arthroscopy Global with reduction: LRD II–IV benefit to patients refractory to non-surgical
30 studies (3 RCTs I3: Disc improvement I2 and I3 (most studies, therapies. The most reliable evidence supports the
and 27 repair ⁄ repositioning Jaw mobility comparable results level IV) effectiveness of arthrocentesis and arthroscopy for
uncontrolled I4: Discectomy Disc displacement patients with disc displacement with reduction.
studies) without reduction: R: Methodological weaknesses of primary studies
Disc displacement Similar results for such as heterogeneous patient material, outcome
with reduction, I1, I2, and I3 measures not clearly defined, and majority of the
Disc displacement studies were not RCTs.
without reduction
1463 patients
Kropmans TJ Qualitative SR of 24 I1: Arthroscopy Pain intensity No synthesis of AMSTAR 2 A: No distinguishing effects on jaw mobility, jaw
1999 (42) studies (6 RCTs I2: Arthrocentesis Jaw function results presented LRD II–IV function, or pain intensity was seen between
and 6 case–control I3: Physical therapy Jaw mobility arthroscopic surgery, arthrocentesis, and physical
and 12 (e.g. exercise, therapy in patients with permanent
uncontrolled massage, TENS) temporomandibular joint disc displacement.
studies) C1: Placebo R: Methodological weaknesses of primary studies
Disc displacement C2: No treatment such as diagnostic criteria of TMD and outcome
without reduction measures in the study. A majority of the studies
4916 patients are LRD level IV, and therefore, it not possible to
draw any clear conclusions from this SR.
Abrahamsson C Qualitative I1: Bilateral sagittal Self-report of Contradictory AMSTAR 8 A: Because of few studies with unambiguous
2007 (44) SR of 3 split and ⁄ or Le Fort symptoms results in signs LRD III results and heterogeneity in study design, the
case–control I osteotomy Clinical and symptoms scientific evidence was insufficient to evaluate the
studies C1: No treatment examination effects that orthognathic surgery had on TMD.
280 patients R: Well-designed SR. Methodological weaknesses
of primary studies such as diagnostic criteria of
TMD and outcome measures in the study.
MANAGEMENT OF TMD
441
442
Table 4. (Continued)
Study design,
T. LIST & S. AXELSSON
Authors, year, diagnosis, and Intervention (I) and Outcome Quality Authors’ (A) conclusions
reference no. of patients control (C) groups measures Results score Reviewers’ (R) comments
Al-Belasy FA Qualitative I1: Arthrocentesis Pain intensity Overall success AMSTAR 2 A: The majority of the reviewed publications were
2007 (43) SR of 19 Studies C1: Not specified Jaw mobility varied between LRD II-IV prospective case series with flawed methodology
(2 RCTs and 6 Clinical 60% -100%. and, despite the impression that arthrocentesis
case–control and examination No comparison may be beneficial for patients with TMJ closed
11 uncontrolled between I1 lock, there have been no good prospective
studies) and C1. randomised clinical trial confirm the efficacy
Anchored disc of the procedure.
phenomenon, R: The overall success rate was high from the
Disc displacement primary studies. The results are difficult to
with or without interpret because of methodological weaknesses
reduction, of primary studies such as diagnostic criteria of
capsulitis ⁄ TMD, outcome measures, missing analysis
synovitis. between Intervention and control treatment in
571 patients the studies. In addition, a majority of the studies
patients received complementary pharmacologic
or conservative treatment besides lavage. The
majority of the studies are LRD level IV, and
therefore, it not possible to draw any clear
conclusions from this SR.
AMSTAR, assessment of multiple systematic reviews; LRD, level of research design; RCT, randomised clinical trials; TMD, temporomandibular disorders.
ª 2010 Blackwell Publishing Ltd
Table 5. Characteristics of systematic reviews (SRs) of behavioural therapy and multimodal treatments
Study design,
Authors, year, diagnosis, and no. Intervention (I) and Outcome Quality Authors’ (A) conclusions
reference of patients control (C) groups measures Results score Reviewers’ (R) comments
Crider AB SR and I1: Electromyographic Pain reduction Pain reduction and AMSTAR 4 A: Although limited in extent, the available
ª 2010 Blackwell Publishing Ltd
1999 (45) meta-analysis of biofeedback Clinical signs of clinical signs: I1 LRD II-IV data support the efficacy of EMG biofeedback
13 RCTs and C1: Active control dysfunction better than treatments for TMD.
un-controlled C2: No treatment or Global assessment C1 and C2 R: Methodological weaknesses of primary
studies placebo studies such as heterogeneous patient
TMD material, outcome measures not clearly
patients* defined, and several studies were not RCTs.
Jedel E Qualitative I1: Biofeedback Self-reported No evidence of an AMSTAR 3 A: The studies were heterogeneous with low
2003 (30) SR of 7 RCTs I2: Acupuncture symptoms effect for any LRD II quality, and therefore, it is not possible to
TMD I3: TENS Pain intensity treatment mode draw any conclusions.
379 patients C1: No treatment Clinical R: Limitations in the SR methodology and
C2: Other treatment examination therefore difficult to draw any conclusions
Crider AB Qualitative I1: Biofeedback Pain intensity I1 was superior to AMSTAR 3 A: Biofeedback training with adjunctive CBT
2005 (46) SR of 6 RCTs training Global C1 in one of two LRD II–III was reported to be an efficacious treatment for
TMD I2: Biofeedback improvement RCTs TMD; both biofeedback training as the sole
449 patients training + CBT Limitation in jaw I2 was significantly intervention and biofeedback-assisted
I3: Biofeedback- function better than relaxation training are probably efficacious
assisted relaxation Depression C2 and I4 treatments.
training Clinical I3 was better R: Small studies, no long-term follow-up.
I4: Alternative examination than C2 Methodological limitations in SR.
treatment I3 was better than
C1: Sham treatment I4 in one of two
C2: No treatment RCTs
SBU (23) Qualitative I1: CBT Pan intensity I1 was better than AMSTAR 6 A: Behavioural treatment such as biofeedback
SR of 2 SRs I2: Biofeedback Daily activities C1 and C3 LRD I–II and CBT have better effect than no treatment.
and 6 RCTs I3: Education Depression I2 was better R: Reviewers and authors are identical persons
TMD I4: Education + home Sleep quality than C2
XX patients instruction I3 was similar to I4
C1: Brief information
C2. No treatment
C3: Conventional
treatment
MANAGEMENT OF TMD
443
444
Table 5. (Continued)
Study design,
Authors, year, diagnosis, and no. Intervention (I) and Outcome Quality Authors’ (A) conclusions
reference of patients control (C) groups measures Results score Reviewers’ (R) comments
McNeely M Qualitative I1: CBT Pain reduction Pain reduction: I1 AMSTAR 7 A: Programmes involving relaxation techniques
T. LIST & S. AXELSSON
2006 (33) SR of 4 RCTs I2: Biofeedback Jaw mobility better than C2 LRD II and biofeedback, electromyographic training,
TMD I3: Relaxation I2 similar effect and proprioceptive re-education may be more
207 patients C1: Occlusal splint to C1 effective than placebo treatment or occlusal
C2: No treatment I2 and I3 similar splints.
effect R: Studies had small numbers of participants
and outcome measures were poorly defined,
so it is difficult to draw any conclusions.
Türp J Qualitative I1: Simple treatment Pain intensity Disc displacement AMSTAR 4 A: Current research suggests that individuals
2007 (47) SR of 11 RCTs I2: Multimodal Graded Chronic without reduction LRD II without major psychological symptoms do not
TMD: treatment Pain Scale with pain: I1 = I2. require more than simple therapy. In contrast,
Disc displacement Analgesic TMD pain, without patients with major psychological
without reduction, consumption major involvement need multimodal,
with pain Psychologic status psychological interdisciplinary therapeutic strategies.
TMD pain, without Pain threshold symptoms: I1 = I2 R: Methodological weaknesses of primary
major TMD pain, with studies such as diagnostic criteria of TMD,
psychological major poor description of how the treatment was
symptoms psychological conducted, and outcome measures in the
TMD pain, with symptoms: study
major I2 better than I1.
psychological
symptoms
895 patients
AMSTAR, assessment of multiple systematic reviews; CBT, cognitive behavioural therapy; LRD, level of research design; RCT, randomised clinical trials; TMD, temporomandibular
disorders.
*Number of patients not reported.
ª 2010 Blackwell Publishing Ltd
MANAGEMENT OF TMD 445
inclusion criteria because of limitations in the quality treatment (two SRs), (ii) better than no treatment
of the studies. when administered in combination with cognitive
Three SRs evaluated surgical treatment of the TMJ in behavioural therapy (CBT) or relaxation (two SRs),
patients with disc displacements (41–43) and one SR and (iii) similar in effect compared with relaxation
orthognathic surgery in patients with TMD (44) training (one SR). Cognitive behavioural therapy was
(Table 4). In patients with disc displacements with reported to be (i) better than conventional treatment
reduction, one SR reported similar treatment effects for (two SRs) and (ii) better than no treatment (one SR).
arthrocentesis, arthroscopy, and discectomy. In patients Education at the clinic and education at the clinic
with disc displacement without reduction, one SR combined with home exercises produced similar results.
reported similar effect for arthrocentesis, arthroscopy, In patients with disc displacement without reduction
and physical therapy. One SR reported overall high and pain and in patients with TMD pain without major
success rate for arthrocentesis but made no comparison psychological symptoms, no difference in outcome was
of arthrocentesis with other interventions. In patients found between simple treatment and multimodal
with TMD pain, one SR reported contradictory results treatment (one SR). But in patients with TMD pain
following orthognathic surgery. But all SRs included in and major psychological symptoms, multimodal treat-
these SRs had low levels of evidence. ment was found to be better than simple treatment.
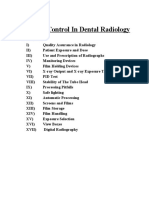
Five SRs evaluated the treatment of various behavio- The overall inter-reliability agreement of the two
ural therapies in patients with TMD (23, 30, 33, 45, 46), authors in assessing the quality of the SRs was 0Æ70 and
and one SR analysed the effect of multimodal and free-marginal kappa 0Æ67. Figure 2 presents percentage
simple treatment in TMD (47) (Table 5). Biofeedback of primary studies cited in one or more of the different
was reported to be (i) better than active control or no SRs for each treatment area.
Occlusal appliance Occlusal adjustment Bruxism
6 SR, 55 studies 4 SR, 12 studies 2 SR, 6 studies
5 4
4 8%
5% 3 2
9%
17% 33%
1
3
43%
18% 1
2 58% 1
17% 67%
2
25%
Acupuncture Physical treatment Pharmacologic treatment
6 SR, 10 studies 4 SR, 26 studies 7 SR, 60 studies
4 4
3 8%
8% 3 13%
5 1 5%
40% 40% 2
12% 2
20% 1
1 62%
4 3 2 72%
10% 0% 10%
TMJ and maxillofacial surgery Behavioral therapy and
4 SR, 54 studies Multimodadal treatment
6 SR, 30 studies
5
3 4
2 7%
4% 7%
15% 1 1 Reference cited number of times
3 36% 2
Fig. 2. Percentage of same primary 17% 3
4
study cited in one or more of the
5
different systematic reviews, for each 1 2
81%
treatment area. 33%
ª 2010 Blackwell Publishing Ltd
446 T. LIST & S. AXELSSON
case series, that is, no control group, which limits the
Discussion
conclusions of the SR. Several leading scientific journals
Systematic reviews are a synthesis and critical assess- have made a united effort to provide guidelines for how
ment of primary studies, or even other SRs, and they a clinical trial should be conducted in the CONSORT
play an important role in evidence-based decision statement (52). These guidelines can be used as a
making. The SR has the benefit that it provides a checklist for avoiding pitfalls in conducting clinical
systematic overview of what has been published on a trials.
specific issue and what current trends are, such as the Our SR found inconsistencies in several SRs con-
effect of various treatment modes in the management cerning diagnosis. Temporomandibular disorders were
of TMD. Because the conclusions in our study are based inconsistently defined in the primary studies but, more
on several SRs published by independent researchers, importantly, also in the SRs reviewed here. Similar
findings are well supported. results were reported for radiographic findings in TMD
Because many researchers and practitioners may not (53). The classification that has been found to provide
have time to read SRs – much less all the primary acceptable reliability and validity and is commonly used
studies on which these SRs are based – a systematic in TMD research is the research diagnostic criteria for
review of these SRs may (i) give a valuable, time-saving temporomandibular disorders (RDC ⁄ TMD) (54, 55).
overview of a specific issue, (ii) provide a pool of The future challenge is to convince researchers to use
references of SRs and of primary studies that have been the diagnostic system with the best evidence – accept-
quality assessed, and (iii) serve as a useful tool for able sensitivity and specificity (56).
giving undergraduate students an understanding of In this SR, a large variety of outcome measures were
how to conduct systematic literature searches and used, and instrument reliability and validity were often
quality assessments of a topic. not described. It is essential that evidence be based on
Studies have indicated that it is difficult to change measures that are important indicators of patient health
competences and knowledge that a dentist learned in and that are not surrogate endpoints. For example, pain
undergraduate dental education (48). It is therefore reduction and daily functioning are more important
important to implement SRs in undergraduate teaching aspects in an evaluation than clicking sounds, deviation
so that students understand evidence-based medicine in mm, or tenderness on palpation. Clinical trials and
(49). SRs must begin meeting international standards, and
The results of the SRs are impacted by the quality of clinical scientists must begin designing and reporting
the primary studies included in the review. However, the such trials. To create a core of common outcome
methodological quality of the SR should not be affected measures in the field of pain, Dworkin et al. and a
by flaws in the primary studies, as long as these flaws are consensus group undertook to put together the
reported, commented on and sufficiently regarded in the Initiative on Methods, Measurements, and Pain Assess-
conclusions. One SR resulted in no included studies but ment in Clinical Trials (IMMPACT) (57). IMMPACT
it was included because it reflected our second aim, to recommendations include the following domains:
assess the methodological quality of SRs (38). pain, physical functioning, emotional functioning,
In AMSTAR, one key item is whether the scientific participant rating of improvement and satisfaction
quality of the included SRs was assessed and docu- with treatment, symptoms and adverse events, and
mented The most commonly used quality assessment participant disposition.
tool used in the SRs was the Jadad score (50). Grades of It is also important that (i) these measures are
Recommendation Assessment, Development and Eval- expressed in clinically relevant terms such as numbers
uation (GRADE) is a recently developed tool for of responders and non-responders to treatment, for
assessing the synthesised evidence for specified out- example, number of patients with >30% pain reduction
come measures. As one of the aims of this study was to and (ii) data are presented in a transparent manner, so
detect trends in the evidence base regarding the overall that mathematical syntheses or meta-analyses of the
effect of different methods for treating TMD, we results may be conducted. In this review, only a few of
decided that introducing GRADE in this context would the SRs had conducted a meta-analysis because of
give too detailed information for this purpose (51). heterogeneity of the original data or methodological
A concern in this SR was that 30% of the SRs included differences such as variability of measures. In future,
ª 2010 Blackwell Publishing Ltd
MANAGEMENT OF TMD 447
the ability to synthesise the results of several primary TMD pain compared to other treatment modalities such
studies would allow more accurate assessment of as physical medicine, behavioural medicine, and acu-
treatment efficacy and treatment effectiveness. This puncture treatment. Overall, documentation on the
approach would allow the continuous update of RCTs long-term pain-relieving effect of occlusal appliances is
in meta-analyses, which would (i) limit the number of limited, as it is for patient compliance in occlusal
qualitative SRs and (ii) allow more accurate, overall appliance treatment. Few SRs reported data on adverse
assessment of treatment result. events related to the use of occlusal appliances. The
major concern with adverse events has been related to
partial non-occluding splints such as the NTI, where the
Quality assessment
design of the splint may contribute to tooth pain and
In this SR, AMSTAR scores ranged from 2 to 11. But it is occlusal changes (24).
important to point out that item scores are not equal in One SR evaluated the use of splints in bruxism,
weight; for example, characteristics of included SRs and which was assessed as number of bruxism episodes per
conflict of interest statement have different weights. hour [electromyographic (EMG) activity] and episodes
With its focus on study design, the LRD was used to with grinding noises. The SR found no significant
supplement AMSTAR in SR quality assessment. Use of differences between occlusal splints, no treatment, and
both instruments was essential to gain perspective on palatinal splints. Small sample size was one explanation
SR quality. for the lack of significance between outcomes which
The number of SRs evaluated in the various treatment the authors of the SR emphasised (27). It should also be
groups ranged from 10 for occlusal splint, occlusal emphasised that some primary studies, particularly
adjustment, and bruxism to 4 for TMJ and maxillofacial those that use polysomnographic registration, are
surgery. In each treatment area, a small number of well- technically very difficult to conduct on large patient
designed primary studies overlapped and were cited in samples. One SR examined tooth attrition related to
several of the SRs that covered that area. But 40–80% of bruxism, and based on two small studies, found that
the primary studies did not overlap between different occlusal appliances retarded wear.
SRs and were only cited once (Fig. 2). Variations No SR found evidence that occlusal adjustments are
between the SRs in aims, inclusion criteria, and time of more or less effective than placebo in the treatment of
data collection may explain this lack of overlap. Despite TMD pain. All SRs were restrictive in recommending
these differences, conclusions drawn in several of the the use of occlusal adjustments for treatment for TMD
SRs for a specific treatment form had similar evidence. pain, especially because this therapy is non-reversible.
Thus, synthesising evidence from several SRs can also be
a tool for validation of this kind of meta-research.
Physical therapy (acupuncture, TENS, exercise, and
A general impression from this study was that
mobilisation)
strength of evidence of an SR was weak if the SR (i)
had a low AMSTAR score (e.g. <5) and (ii) was based Most SRs found evidence that acupuncture is better
upon non-randomised studies. In SRs where AMSTAR than no treatment and comparable to other forms of
scores ranged between 5 and 10, the results were conservative treatment. But because of methodological
similar, regardless of quality. It has been emphasised shortcomings, MacPherson et al. recommended specific
that a clinical trial should follow strict rules; likewise an guidelines to improve the quality of intervention
SR should be conducted in a standardised manner. primary studies; before effectiveness of acupuncture
can be determined more primary studies are needed
(58). Few SRs reported any adverse events or side-
Occlusal appliances, occlusal adjustment, and bruxism
effects from acupuncture treatment. In treatment of
Several of the SRs concluded that management of TMD patients with TMD, side-effects seem to be rare or
with a stabilisation splint worn at night is likely to lead complications only minor (59). MacPherson et al. came
to short-term improvement when compared with no to similar conclusions concerning use of acupuncture in
treatment, but is inconclusive compared with placebo general for pain treatment in a large population group
(non-occluding palatinal splint). In the short term, (60). Major adverse events are very rare, but because
stabilisation splints were equally effective in reducing some have occurred following acupuncture treatment,
ª 2010 Blackwell Publishing Ltd
448 T. LIST & S. AXELSSON
it is strongly recommended that those practicing acu- intensity, and mandibular functioning to the same
puncture have good theoretical knowledge and training degree. Success rates were often high, independent of
in the therapy (61). treatment mode. The effect of maxillofacial surgery on
Next to information, patient education, and occlusal TMD pain is unclear. Many of the RCTs included in the
appliance, jaw exercises are a common form of TMD SRs had low quality scores, and outcome measures were
treatment (62). One SR found active exercise and often coarse, which made data difficult to interpret.
postural training to be effective in treatment of TMD One important aspect in the evaluation of invasive
pain but no evidence for the effectiveness of various TMJ interventions versus conservative treatment is the
electrical modalities. Overall, few primary studies have patient groups. In most TMJ surgery primary studies,
been published and more research is needed to estab- the inclusion criterion for entering the study was
lish the efficacy of the various physical treatment that the patient had been refractory to conserva-
modalities, including acupuncture. tive treatment for 6 months, while the inclusion
criterion for conservative treatment was pain duration
of 6 months. So a comparison between the groups is
Pharmacologic treatment
inconclusive.
Several SRs indicated that analgesics, antidepressants, More well-designed primary studies with proper
diazepam, hyaluronate, and glycocorticoid may be evidence-based standards are needed to identify the
effective in TMD pain. Few primary studies were well patients who are most suited for surgical interventions.
designed with a relevant follow-up time, so the main
conclusion in the SR was that results were heteroge-
Behavioural therapy and multimodal treatment
neous, and no conclusions could be drawn. But it is
important to differentiate between lack of evidence and All SRs of behavioural therapy concluded that this type
evidence for lack of effect. Because of current limitations in of treatment was effective in treating TMD pain. The
knowledge of pharmacologic effects on TMD pain, only treatment modalities included education, biofeedback,
comparisons between similar pain conditions such as relaxation training, stress management, and CBT.
backache or tension-type headache can be made. In Treatment modes were often combined, for example,
several chronic pain conditions, drugs such as analge- biofeedback and relaxation could be compared with
sics, opioids, antidepressants, and anti-epileptics have biofeedback and CBT, making it difficult to determine
been found to be effective in relieving pain (63); these which part of the treatment was most important.
drugs would probably be effective in TMD pain. Several primary studies indicated that behavioural
Important endpoints such as numbers needed to treat therapy was as effective as other forms of conservative
(NNT) and numbers needed to harm (NNH) were rare TMD treatment.
in these primary studies, despite being recommended One SR reported that most patients with TMD
for use in pharmacologic treatment studies because without psychological involvement benefited from
they are easy to understand and provide a clinically simple treatments. Patients with TMD pain and major
relevant measure of the success rate and rate of harm of psychological disturbances were in need of a combined
an intervention (63). therapeutic approach. This emphasises the need for
The SR on pharmacologic treatment reported minor combining the clinical examination with a behavioural
adverse events. Because there is currently no criterion assessment to be able to direct the patient to the proper
standard in the pharmacological treatment of chronic mode of treatment. The RDC ⁄ TMD is a classification
oro-facial pain, the positive effects of drugs must be system that uses a clinical (axis I) and a psychosocial
weighed against possible adverse and toxic effects, and assessment (axis II) to gain a more complete picture of
risk of dependency. the patient; Garofalo and Wesley recommended this
approach – use of a dual axis – in chronic pain
assessment (64).
TMJ and maxillofacial surgery
Evidence-based medicine is defined as the integration
The SRs of surgical treatment of TMD concluded that of best research evidence with clinical expertise and
arthroscopic surgery, arthrocentesis, and physical ther- patient values. In future, we need to expand our
apy affected mandibular movement, reduction in pain understanding of how to:
ª 2010 Blackwell Publishing Ltd
MANAGEMENT OF TMD 449
1 Tailor treatment for the individual patient, so they 2. Macfarlane TV, Glenny AM, Worthington HV. Systematic
benefit from the best treatment for them. review of population-based epidemiological studies of oro-
facial pain. J Dent. 2001;29:451–467.
2 Transfer research findings to the practicing dentist,
3. Dworkin SF, Von Korff M, LeResche L. Multiple pains and
because they are the main caregiver of patients with psychiatric disturbance. An epidemiologic investigation. Arch
TMD. Gen Psychiatry. 1990;47:239–244.
3 Balance our judgment of best research evidence with 4. List T, Dworkin SF. Comparing TMD diagnoses and clinical
clinical expertise in the choice of treatment. findings at Swedish and US TMD centers using research
4 Gain more information about patient preferences diagnostic criteria for temporomandibular disorders. J Orofac
Pain. 1996;10:240–253.
and values and what impact this has on treatment
5. John MT, Reissmann DR, Schierz O, Wassell RW. Oral health-
outcome. related quality of life in patients with temporomandibular
disorders. J Orofac Pain. 2007;21:46–54.
6. Turp JC, Motschall E, Schindler HJ, Heydecke G. In patients
Conclusions with temporomandibular disorders, do particular interven-
tions influence oral health-related quality of life? A qualita-
There is some evidence that occlusal appliances,
tive systematic review of the literature. Clin Oral Implants
acupuncture, behavioural therapy, jaw exercises, pos- Res. 2007;18(Suppl 3):127–137.
tural training, and some pharmacological treatments 7. Davidoff F, Haynes B, Sackett D, Smith R. Evidence based
can be effective in alleviating pain in patients with medicine. BMJ. 1995;310:1085–1086.
TMD. Evidence is insufficient for the effect of electro- 8. Shea BJ, Grimshaw JM, Wells GA, Boers M, Andersson N,
Hamel C et al. Development of AMSTAR: a measurement tool
physical modalities and surgery. Occlusal adjustment
to assess the methodological quality of systematic reviews.
seems to have no effect according to the available
BMC Med Res Methodol. 2007;7:10.
evidence. One limitation of most of the SRs reviewed 9. Shea BJ, Hamel C, Wells GA, Bouter LM, Kristjansson E,
was that the considerable variation in methodology Grimshaw J et al. AMSTAR is a reliable and valid measure-
between the primary studies made definitive conclu- ment tool to assess the methodological quality of systematic
sions impossible. reviews. J Clin Epidemiol. 2009;62:1013–1020.
10. Antes G. [Evidence-based medicine]. Internist (Berl).
1998;39:899–908.
Acknowledgments 11. Forssell H, Kalso E, Koskela P, Vehmanen R, Puukka P,
Alanen P. Occlusal treatments in temporomandibular disor-
To the participants of the 2009 Colloquium on Oral ders: a qualitative systematic review of randomized controlled
Rehabilitation in Sienna, who provided valuable feed- trials. Pain. 1999;83:549–560.
back on the manuscript. 12. Koh H, Robinson PG. Occlusal adjustment for treating and
preventing temporomandibular joint disorders. J Oral Reha-
bil. 2004;31:287–292.
Declaration of interests 13. Al-Ani Z, Gray RJ, Davies SJ, Sloan P, Glenny AM. Stabiliza-
tion splint therapy for the treatment of temporomandibular
Dr Axelsson is a staff member and a project director at myofascial pain: a systematic review. J Dent Educ.
the Swedish Council on Technology Assessment in 2005;69:1242–1250.
14. Ismail AI, Bader JD. Evidence-based dentistry in clinical
Health Care (SBU).
practice. J Am Dent Assoc. 2004;135:78–83.
15. Mohlin B, Axelsson S, Paulin G, Pietila T, Bondemark L,
Authors’ contributions Brattstrom V et al. TMD in relation to malocclusion and
orthodontic treatment. Angle Orthod. 2007;77:542–
Dr List conceived the project, developed the protocol, 548.
conducted searches, and prepared the manuscript. Both 16. Kim MR, Graber TM, Viana MA. Orthodontics and temporo-
mandibular disorder: a meta-analysis. Am J Orthod Dentofa-
authors undertook data collection and extraction. Dr
cial Orthop. 2002;121:438–446.
Axelsson contributed to manuscript preparation. 17. Rinchuse DJ, McMinn JT. Summary of evidence-based
systematic reviews of temporomandibular disorders. Am J
Orthod Dentofacial Orthop. 2006;130:715–720.
References 18. Bessa-Nogueira RV, Vasconcelos BC, Niederman R. The
1. Drangsholt M. Temporomandibular pain. In: Crombie IK, methodological quality of systematic reviews comparing
Croft PR, Linton SJ, LeResche L, Von Korff M, eds. Epidemi- temporomandibular joint disorder surgical and non-surgical
ology of pain. Seattle (WA): IASP Press; 1999:203–233. treatment. BMC Oral Health. 2008;8:27.
ª 2010 Blackwell Publishing Ltd
450 T. LIST & S. AXELSSON
19. Al-Ani MZ, Davies SJ, Gray RJ, Sloan P, Glenny AM. 34. Medlicott MS, Harris SR. A systematic review of the effec-
Stabilisation splint therapy for temporomandibular pain tiveness of exercise, manual therapy, electrotherapy, relaxa-
dysfunction syndrome. Cochrane Database Syst Rev. 2004;1: tion training, and biofeedback in the management of
CD002778. temporomandibular disorder. Phys Ther. 2006;86:955–973.
20. Forssell H, Kalso E. Application of principles of evidence-based 35. Sommer C. [Pharmacotherapy of orofacial pain]. Schmerz.
medicine to occlusal treatment for temporomandibular disor- 2002;16:381–388.
ders: are there lessons to be learned? J Orofac Pain. 36. List T, Axelsson S, Leijon G. Pharmacologic interventions in
2004;18:9–22; discussion 23–32. the treatment of temporomandibular disorders, atypical facial
21. Turp JC, Komine F, Hugger A. Efficacy of stabilization splints pain, and burning mouth syndrome. A qualitative systematic
for the management of patients with masticatory muscle pain: review. J Orofac Pain. 2003;17:301–310.
a qualitative systematic review. Clin Oral Investig. 2004;8: 37. Shi Z, Guo C, Awad M. Hyaluronate for temporomandibular
179–195. joint disorders. Cochrane Database Syst Rev. 2003;1:
22. Fricton J. Current evidence providing clarity in management CD002970.
of temporomandibular disorders: summary of a systematic 38. Al-Muharraqi MA, Fedorowicz Z, Al Bareeq J, Al Bareeq R,
review of randomized clinical trials for intra-oral appliances Nasser M. Botulinum toxin for masseter hypertrophy. Coch-
and occlusal therapies. J Evid Based Dent Pract. 2006;6:48–52. rane Database Syst Rev. 2009;1:CD007510.
23. SBU. Methods of treating chronic pain. In: Axelsson S, Boivie J, 39. Cascos-Romero J, Vazquez-Delgado E, Vazquez-Rodriguez E,
Eckerlund I, Gerdle B, Johansson E, Kristiansson M, List T, Gay-Escoda C. The use of tricyclic antidepressants in the
Lundberg B, Mannheimer C, Marke¢ L-Å, Olsson G, Segerdahl treatment of temporomandibular joint disorders: systematic
M, Sjöström B, Söderlund A, Willman A, eds. SBU-report no review of the literature of the last 20 years. Med Oral Patol
177:1+2. Stockholm: The Swedish Council on Technology Oral Cir Bucal. 2009;14:E3–E7.
Assessment in Health and Care (SBU); 2006:299–410, 437–443. 40. Ihde SK, Konstantinovic VS. The therapeutic use of botu-
24. Stapelmann H, Turp JC. The NTI-tss device for the therapy of linum toxin in cervical and maxillofacial conditions: an
bruxism, temporomandibular disorders, and headache – where evidence-based review. Oral Surg Oral Med Oral Pathol Oral
do we stand? A qualitative systematic review of the literature. Radiol Endod. 2007;104:e1–e11.
BMC Oral Health. 2008;8:22. 41. Reston JT, Turkelson CM. Meta-analysis of surgical treatments
25. Santacatterina A, Paoli M, Peretta R, Bambace A, Beltrame A. for temporomandibular articular disorders: a reply to the
A comparison between horizontal splint and repositioning discussants. J Oral Maxillofac Surg. 2003;61:737–738.
splint in the treatment of ‘disc dislocation with reduction’. 42. Kropmans TJ, Dijkstra PU, Stegenga B, de Bont LG. Ther-
Literature meta-analysis. J Oral Rehabil. 1998;25:81–88. apeutic outcome assessment in permanent temporomandib-
26. Koh H, Robinson PG. Occlusal adjustment for treating and ular joint disc displacement. J Oral Rehabil. 1999;26:
preventing temporomandibular joint disorders. Cochrane 357–363.
Database Syst Rev. 2003;1:CD003812. 43. Al-Belasy FA, Dolwick MF. Arthrocentesis for the treatment of
27. Macedo CR, Silva AB, Machado MA, Saconato H, Prado GF. temporomandibular joint closed lock: a review article. Int J
Occlusal splints for treating sleep bruxism (tooth grinding). Oral Maxillofac Surg. 2007;36:773–782.
Cochrane Database Syst Rev. 2007;4:CD005514. 44. Abrahamsson C, Ekberg E, Henrikson T, Bondemark L.
28. van ‘tSpijker A, Kreulen CM, Creugers NH. Attrition, occlu- Alterations of temporomandibular disorders before and after
sion, (dys)function, and intervention: a systematic review. orthognathic surgery: a systematic review. Angle Orthod.
Clin Oral Implants Res. 2007;18(Suppl 3):117–126. 2007;77:729–734.
29. Ernst E, White AR. Acupuncture as a treatment for tempo- 45. Crider AB, Glaros AG. A meta-analysis of EMG biofeedback
romandibular joint dysfunction: a systematic review of ran- treatment of temporomandibular disorders. J Orofac Pain.
domized trials. Arch Otolaryngol Head Neck Surg. 1999;13:29–37.
1999;125:269–272. 46. Crider A, Glaros AG, Gevirtz RN. Efficacy of biofeedback-
30. Jedel E, Carlsson J. Biofeedback, acupuncture and transcuta- based treatments for temporomandibular disorders. Appl
neous electric nerve stimulation in the management of Psychophysiol Biofeedback. 2005;30:333–345.
temporomandibular disorders: a systematic review. Phys Ther 47. Turp JC, Jokstad A, Motschall E, Schindler HJ, Windecker-
Rev. 2003;8:217–223. Getaz I, Ettlin DA. Is there a superiority of multimodal as
31. Rosted P. The use of acupuncture in dentistry: a review of the opposed to simple therapy in patients with temporomandib-
scientific validity of published papers. Oral Dis. 1998;4: ular disorders? A qualitative systematic review of the litera-
100–104. ture. Clin Oral Implants Res. 2007;18(Suppl 3):138–150.
32. Fink M, Rosted P, Bernateck M, Stiesch-Scholz M, Karst M. 48. Greenhalgh T, Robert G, Macfarlane F, Bate P, Kyriakidou
Acupuncture in the treatment of painful dysfunction of the O. Diffusion of innovations in service organizations: system-
temporomandibular joint – a review of the literature. Forsch atic review and recommendations. Milbank Q. 2004;82:
Komplementmed. 2006;13:109–115. 581–629.
33. McNeely ML, Armijo Olivo S, Magee DJ. A systematic review 49. Sackett D, Straus S, Richardson WS, Rosenberg W, Haynes R.
of the effectiveness of physical therapy interventions for Evidence-based medicine. How to practice and teach EBM.
temporomandibular disorders. Phys Ther. 2006;86:710–725. Edinburgh: Churchill Livingstone; 2000.
ª 2010 Blackwell Publishing Ltd
MANAGEMENT OF TMD 451
50. Jadad AR, Moore RA, Carroll D, Jenkinson C, Reynolds DJ, 58. MacPherson H, White A, Cummings M, Jobst KA, Rose K,
Gavaghan DJ et al. Assessing the quality of reports of Niemtzow RC. Standards for Reporting Interventions in
randomized clinical trials: is blinding necessary? Control Clin Controlled Trials of Acupuncture: the STRICTA recommen-
Trials. 1996;17:1–12. dations. J Altern Complement Med. 2002;8:85–89.
51. Atkins D, Best D, Briss PA, Eccles M, Falck-Ytter Y, Flottorp S 59. List T, Helkimo M. Adverse events of acupuncture and
et al. Grading quality of evidence and strength of recommen- occlusal splint therapy in the treatment of craniomandibular
dations. BMJ. 2004;328:1490. disorders. Cranio. 1992;10:318–324; discussion 324–6.
52. Moher D, Schulz KF, Altman D. The CONSORT statement: 60. MacPherson H, Thomas K, Walters S, Fitter M. A prospective
revised recommendations for improving the quality of reports survey of adverse events and treatment reactions following
of parallel-group randomized trials. JAMA. 2001;285: 34,000 consultations with professional acupuncturists. Acu-
1987–1991. punct Med. 2001;19:93–102.
53. Koh KJ, List T, Petersson A, Rohlin M. Relationship between 61. Ernst E, White A. Life-threatening adverse reactions
clinical and magnetic resonance imaging diagnoses and after acupuncture? A systematic review. Pain. 1997;71:123–
findings in degenerative and inflammatory temporomandib- 126.
ular joint diseases: a systematic literature review. J Orofac 62. Tegelberg A, List T, Wahlund K, Wenneberg B. Temporo-
Pain. 2009;23:123–139. mandibular disorders in children and adolescents: a survey of
54. Dworkin SF, LeResche L. Research diagnostic criteria for dentists’ attitudes, routine and experience. Swed Dent J.
temporomandibular disorders: review, criteria, examinations 2001;25:119–127.
and specifications, critique. J Craniomandib Disord. 1992; 63. McQuay H, Moore A. An evidence-based resource for pain
6:301–355. relief. Oxford: Oxford University Press; 1998.
55. Schiffman E, Truelove E, Ohrbach R, Anderson GC, John MT, 64. Garofalo J, Wesley A. Research diagnostic criteria for tempo-
List T, Look J. The research diagnostic criteria for tempor- romandibular disorders: reflection pf the physical-psycholog-
omandibular disorders. I: overview and methodology for ical interface. ASP Bull. 1997;3:4–16.
assessment of validity. J Orofacial Pain. 2010;24:7–24. 65. Jedel E, Carlsson J. Biofeedback, acupuncture and transcuta-
56. Whiting P, Rutjes AW, Reitsma JB, Bossuyt PM, Kleijnen J. neous electric nerve stimulation in the management of
The development of QUADAS: a tool for the quality assess- temporomandibular disorders. A systematic review. J Orofac
ment of studies of diagnostic accuracy included in systematic Pain. 2003;8:217–223.
reviews. BMC Med Res Methodol. 2003;3:25.
57. Dworkin RH, Turk DC, Farrar JT, Haythornthwaite JA, Jensen Correspondence: Thomas List, DDS, Odont. dr, Department of
MP, Katz NP et al. Core outcome measures for chronic pain Stomatognathic Physiology, Faculty of Odontology, Malmö Univer-
clinical trials: IMMPACT recommendations. Pain. 2005;113: sity, SE-205 06 Malmö, Sweden. E-mail: Thomas.list@mah.se
9–19.
ª 2010 Blackwell Publishing Ltd
You might also like
- Essentials of Dental Medicine Text in CRDocument14 pagesEssentials of Dental Medicine Text in CRIvan Galic0% (1)
- DriftodonticsDocument2 pagesDriftodonticssweetie0% (1)
- Tong 2017Document12 pagesTong 2017Dina AnisawatiNo ratings yet
- Rheumatology 2009 Langhorst 1155 9Document5 pagesRheumatology 2009 Langhorst 1155 9AleCsss123No ratings yet
- Class II Functional Orthopaedic Treatment - A Systematic Review of Systematic ReviewsDocument19 pagesClass II Functional Orthopaedic Treatment - A Systematic Review of Systematic ReviewsMonica JohanaNo ratings yet
- Systematic Review-Stuttering Treatment ResearchDocument22 pagesSystematic Review-Stuttering Treatment Researchmajid mirzaeeNo ratings yet
- NG 2007Document19 pagesNG 2007NunoGonçalvesNo ratings yet
- A Systematic Review of Treatments For Mild Traumatic Brain InjuryDocument3 pagesA Systematic Review of Treatments For Mild Traumatic Brain InjurySergio Machado NeurocientistaNo ratings yet
- Z Al-Roubaie - 2020Document12 pagesZ Al-Roubaie - 2020Kossay ZaouiNo ratings yet
- Part 17 PDFDocument6 pagesPart 17 PDFKarolina PolskaNo ratings yet
- Ramsey 2014Document12 pagesRamsey 2014rohanaNo ratings yet
- A Step-By-Step Guide To The SystematicDocument5 pagesA Step-By-Step Guide To The SystematicWiwien HendrawanNo ratings yet
- LI, Meixuan Et Al. (2019)Document6 pagesLI, Meixuan Et Al. (2019)Rafael ConcursoNo ratings yet
- Effectiveness of Adjunctive Interventions For Accelerating Orthodontic Tooth Movement: A Systematic Review of Systematic ReviewsDocument19 pagesEffectiveness of Adjunctive Interventions For Accelerating Orthodontic Tooth Movement: A Systematic Review of Systematic ReviewsfghdhmdkhNo ratings yet
- Incidencia de La Reabsorcion Espontanea de HNPDocument8 pagesIncidencia de La Reabsorcion Espontanea de HNPNicolas ParejaNo ratings yet
- Occupational Therapy For Rheumatoid Arthritis: A Systematic ReviewDocument14 pagesOccupational Therapy For Rheumatoid Arthritis: A Systematic ReviewispasNo ratings yet
- Systematic Reviews and Meta-Analyses in The Orthopedic Literature: Assessment of The Current State of Quality and Proposal of A New Rating StrategyDocument7 pagesSystematic Reviews and Meta-Analyses in The Orthopedic Literature: Assessment of The Current State of Quality and Proposal of A New Rating StrategyasclepiuspdfsNo ratings yet
- Prognostic Factors in Non-Surgically Treated Sciatica: A Systematic ReviewDocument11 pagesPrognostic Factors in Non-Surgically Treated Sciatica: A Systematic ReviewDhiaul IzzahNo ratings yet
- Difference Between Literature Review and MethodologyDocument6 pagesDifference Between Literature Review and MethodologyhfuwwbvkgNo ratings yet
- Hepp, Niedtfeld, Schulze (Accepted Draft) - Experimental Paradigms in Personality Disorder Research - PDTRTDocument33 pagesHepp, Niedtfeld, Schulze (Accepted Draft) - Experimental Paradigms in Personality Disorder Research - PDTRTTelor GorengNo ratings yet
- Reviewon QualityassessmentDocument13 pagesReviewon QualityassessmentnewsPewNo ratings yet
- Principles of Drug Literature Evaluation For Observational Study DesignsDocument13 pagesPrinciples of Drug Literature Evaluation For Observational Study Designs李姵瑩No ratings yet
- Effectiveness of The Open Bite Treatment in Growing Children and Adolescents. A Systematic ReviewDocument14 pagesEffectiveness of The Open Bite Treatment in Growing Children and Adolescents. A Systematic Reviewhasan.abomohamedNo ratings yet
- Quality Assessment of Systematic Reviews On Alveolar Socket Preservation.Document9 pagesQuality Assessment of Systematic Reviews On Alveolar Socket Preservation.andreita_loppNo ratings yet
- Development of A Quantitative Scoring Method For Strobe ChecklistDocument13 pagesDevelopment of A Quantitative Scoring Method For Strobe Checklistgopi mistryNo ratings yet
- 1 s2.0 S0897189716300234 MainDocument7 pages1 s2.0 S0897189716300234 MainVenice s SantosNo ratings yet
- Literature Research: Aims and Design of Systematic Reviews : HCW de Vet, AP Verhagen, I Logghe and RWJG OsteloDocument4 pagesLiterature Research: Aims and Design of Systematic Reviews : HCW de Vet, AP Verhagen, I Logghe and RWJG OsteloNina Ricci AraracapNo ratings yet
- Artigo ResistTraining Reduce Hypertension MetaanalysisDocument5 pagesArtigo ResistTraining Reduce Hypertension MetaanalysisRafaela AssunçãoNo ratings yet
- Prognosis of Six-Month Functioning After Moderate To Severe Traumatic Brain Injury: A Systematic Review of Prospective Cohort StudiesDocument12 pagesPrognosis of Six-Month Functioning After Moderate To Severe Traumatic Brain Injury: A Systematic Review of Prospective Cohort StudiesYan Sheng HoNo ratings yet
- PIIS0007091221001422Document9 pagesPIIS0007091221001422ArolNo ratings yet
- Palliative CareDocument7 pagesPalliative CaremiguelplenoNo ratings yet
- Jeehp 10 12Document7 pagesJeehp 10 12Fabio da CostaNo ratings yet
- Methodological Quality of Systematic Reviews of Animal Studies - A Survey of Reviews of Basic ResearchDocument6 pagesMethodological Quality of Systematic Reviews of Animal Studies - A Survey of Reviews of Basic Researchgabriela_mariangela5929No ratings yet
- ارزیابی مقالات کارآزمایی بالینی دارای گروه کنترل تصادفی شده مجله دانشکده دندانپزشکی دانشگاه علوم پزشکی مشهد منتشره از سال 2831 الی2814Document10 pagesارزیابی مقالات کارآزمایی بالینی دارای گروه کنترل تصادفی شده مجله دانشکده دندانپزشکی دانشگاه علوم پزشکی مشهد منتشره از سال 2831 الی2814Majid KarimiNo ratings yet
- Augmentation Therapies For Treatment-Resistant Depression: Systematic Review and Meta-AnalysisDocument10 pagesAugmentation Therapies For Treatment-Resistant Depression: Systematic Review and Meta-AnalysisjonascarvNo ratings yet
- Clavicle ORIFDocument8 pagesClavicle ORIFsefhilla putriNo ratings yet
- Guidelines On Presenting at Journal ClubDocument6 pagesGuidelines On Presenting at Journal ClubreewenNo ratings yet
- Clinical Reasoning in Medicine: A Concept Analysis: Shahram Yazdani, MD Maryam Hoseini Abardeh, MSCDocument9 pagesClinical Reasoning in Medicine: A Concept Analysis: Shahram Yazdani, MD Maryam Hoseini Abardeh, MSCPascalina Monts'onyaneNo ratings yet
- R01ev ApendicDocument10 pagesR01ev ApendicJimena Rocio MancillaNo ratings yet
- Bluephase G4 - De, En, FR, It, Es, PTDocument7 pagesBluephase G4 - De, En, FR, It, Es, PTAngela Quintero CalderonNo ratings yet
- Systematic Reviews and Meta-And Pooled AnalysesDocument11 pagesSystematic Reviews and Meta-And Pooled AnalysesVictor abramonteNo ratings yet
- Therapeutic Exercise and Orthopedic Manual Therapy For Impingement Syndrome: A Systematic ReviewDocument7 pagesTherapeutic Exercise and Orthopedic Manual Therapy For Impingement Syndrome: A Systematic ReviewkhushmitNo ratings yet
- MINORS Criteria For Non-Randomized StudiesDocument5 pagesMINORS Criteria For Non-Randomized StudiesRamiro Manzano NúñezNo ratings yet
- Systematic Literature Review Vs Meta AnalysisDocument9 pagesSystematic Literature Review Vs Meta Analysisafdtsebxc100% (1)
- Chiropractic & Osteopathy: On The Reliability and Validity of Manual Muscle Testing: A Literature ReviewDocument23 pagesChiropractic & Osteopathy: On The Reliability and Validity of Manual Muscle Testing: A Literature ReviewEdgardo BivimasNo ratings yet
- A Survey of Prevalence of Narrative and Systematic-2017Document7 pagesA Survey of Prevalence of Narrative and Systematic-2017Zezinho zéNo ratings yet
- Prevalence of Myofascial Trigger Points in Spinal Disorders: A Systematic Review and Meta-AnalysisDocument22 pagesPrevalence of Myofascial Trigger Points in Spinal Disorders: A Systematic Review and Meta-AnalysisGabriel Gaspar Bike FitNo ratings yet
- Gagnier2012 - Investigating CHDocument15 pagesGagnier2012 - Investigating CHrestu pangestutiNo ratings yet
- RC0602 Prolotherapy FinalDocument42 pagesRC0602 Prolotherapy Finalesma bekirogluNo ratings yet
- NIH Public Access: Author ManuscriptDocument16 pagesNIH Public Access: Author ManuscriptMarvin BundoNo ratings yet
- Effectiveness of An Osteopathic Treatment On TheDocument2 pagesEffectiveness of An Osteopathic Treatment On ThedhirenNo ratings yet
- Systematic Reviews and Met A Analysis Scientific Rationale and InterpretationDocument9 pagesSystematic Reviews and Met A Analysis Scientific Rationale and InterpretationIbn JesseNo ratings yet
- Evidence-Based Dentistry. How To Design A Research? A Literature ReviewDocument7 pagesEvidence-Based Dentistry. How To Design A Research? A Literature ReviewNadya ANo ratings yet
- Peterson 2008Document10 pagesPeterson 2008Fatamorgana AbdullahNo ratings yet
- Are We Improving? Update and Critical Appraisal of The Reporting of Decision Process and Quality Measures in Trials Evaluating Patient Decision AidsDocument6 pagesAre We Improving? Update and Critical Appraisal of The Reporting of Decision Process and Quality Measures in Trials Evaluating Patient Decision AidsThu ThảoNo ratings yet
- Rodriguez 2017Document10 pagesRodriguez 2017oni yanuarNo ratings yet
- Literature Review On Rheumatoid ArthritisDocument6 pagesLiterature Review On Rheumatoid Arthritispib0b1nisyj2100% (1)
- Jurnal EnglishDocument6 pagesJurnal EnglishMuhammad HazmiNo ratings yet
- Periodontal Health During Orthodontic Treatment With Clear Aligners and Fixed AppliancesDocument21 pagesPeriodontal Health During Orthodontic Treatment With Clear Aligners and Fixed AppliancesabocoliNo ratings yet
- Tailieuxanh cc3803 0597Document8 pagesTailieuxanh cc3803 0597Cu ChíNo ratings yet
- 2014 - Methods, Diagnostic Criteria, Cutoff Points, and Prevalence of Sarcopenia Among Older PeopleDocument12 pages2014 - Methods, Diagnostic Criteria, Cutoff Points, and Prevalence of Sarcopenia Among Older PeopleAlex LimaNo ratings yet
- Analysis of Clinical Trials Using SAS: A Practical Guide, Second EditionFrom EverandAnalysis of Clinical Trials Using SAS: A Practical Guide, Second EditionNo ratings yet
- Surgery ElevatorsDocument9 pagesSurgery ElevatorsmegamarwaNo ratings yet
- Oral Med Handbook 2020 2021Document75 pagesOral Med Handbook 2020 2021chandru104No ratings yet
- Facial Starter Guide: By, Sand and John SparrowDocument11 pagesFacial Starter Guide: By, Sand and John SparrowpkwatchbuzzNo ratings yet
- Fonetica Resumen Primer ParcialDocument11 pagesFonetica Resumen Primer Parcialemilse RodríguezNo ratings yet
- Askar 2018Document5 pagesAskar 2018Pau Robles FdzNo ratings yet
- 1 Super Bond CBblackbookletDocument52 pages1 Super Bond CBblackbookletHRNo ratings yet
- Malocclusion: Dr. Sanam Tauheed Assistant ProfessorDocument40 pagesMalocclusion: Dr. Sanam Tauheed Assistant ProfessorayeshaNo ratings yet
- Dental Occlusion Ties A Rapid Safe and Non-InvasivDocument6 pagesDental Occlusion Ties A Rapid Safe and Non-InvasivFernando CasanovaNo ratings yet
- TUTORIAL IN ENGLISH Blok 12Document7 pagesTUTORIAL IN ENGLISH Blok 12Ifata RDNo ratings yet
- Dental Update 20-03-2021Document3 pagesDental Update 20-03-2021Hari PriyaNo ratings yet
- Comperasion of Healing ProcessDocument6 pagesComperasion of Healing ProcessMitha Ratu amandaNo ratings yet
- Dental Hygiene Remediation Coursework For Graduates of UnaccreditedDocument7 pagesDental Hygiene Remediation Coursework For Graduates of Unaccreditedbotav1nakak3100% (2)
- Dental Assistants in OrthodonticsDocument2 pagesDental Assistants in Orthodonticsmaryam fatimaNo ratings yet
- ReportDocument2 pagesReportChris AdoraNo ratings yet
- Intrusion ArchesDocument7 pagesIntrusion ArchesHARITHA H.PNo ratings yet
- A Case Study About Cleft Lip and Cleft PalateDocument12 pagesA Case Study About Cleft Lip and Cleft PalateLerma PagcaliwanganNo ratings yet
- Penetration Depth of Irrigants Into Root Dentine After Sonic, Ultrasonic and Photoacoustic ActivationDocument8 pagesPenetration Depth of Irrigants Into Root Dentine After Sonic, Ultrasonic and Photoacoustic ActivationAndras KuthiNo ratings yet
- Case Report Endo Perio Lesions-A Synergistic ApproachDocument5 pagesCase Report Endo Perio Lesions-A Synergistic ApproachRyanka Dizayani PutraNo ratings yet
- Mandibular Buccal Bifurcation Cyst: Case Report and Literature ReviewDocument5 pagesMandibular Buccal Bifurcation Cyst: Case Report and Literature Reviewboooow92No ratings yet
- Why Does Inferior Alveolar Nerve Block Fail - A ReviewDocument15 pagesWhy Does Inferior Alveolar Nerve Block Fail - A ReviewSetu KatyalNo ratings yet
- Dental Instruments 6th Edition Boyd Test BankDocument4 pagesDental Instruments 6th Edition Boyd Test Bankteresawatsonezryabigfk100% (15)
- Infection Control in Dental X-Ray RoomDocument13 pagesInfection Control in Dental X-Ray RoomAlaa MoradNo ratings yet
- Starcke 1975Document5 pagesStarcke 1975Spardha ShrivastavaNo ratings yet
- Maxillofacial Injuries (3) / Orthodontic Courses by Indian Dental AcademyDocument9 pagesMaxillofacial Injuries (3) / Orthodontic Courses by Indian Dental Academyindian dental academyNo ratings yet
- Imes-Icore Technologieprospekt EN 2013Document45 pagesImes-Icore Technologieprospekt EN 2013Liviu BirtNo ratings yet
- Asymmetry in Orthodontics QaDocument3 pagesAsymmetry in Orthodontics Qadrzana78No ratings yet
- Enamel and DentinDocument64 pagesEnamel and DentinasdababuNo ratings yet
- Efficacy of Airpolishing Devices Without Removal of Implantsupported Fullarch ProsthesesDocument11 pagesEfficacy of Airpolishing Devices Without Removal of Implantsupported Fullarch ProsthesesDiego Saavedra MoralesNo ratings yet