You might also like
- Anesthesiology Resident Manual of Procedures: A Step-by-Step GuideFrom EverandAnesthesiology Resident Manual of Procedures: A Step-by-Step GuideNo ratings yet
- General ConceptsDocument18 pagesGeneral ConceptsMoxie MacadoNo ratings yet
- Peripheral Vascular (PVS) Examination OSCE Station GuideDocument4 pagesPeripheral Vascular (PVS) Examination OSCE Station GuideNikita JacobsNo ratings yet
- Lung Ultrasound Made Easy Step-By-Step GuideDocument40 pagesLung Ultrasound Made Easy Step-By-Step GuideJorge PérezNo ratings yet
- Lung Ultrasound Made Easy Step-By-Step GuideDocument48 pagesLung Ultrasound Made Easy Step-By-Step GuideEL SHITA100% (1)
- Appendix A: Doppler Ultrasound and Ankle-Brachial Pressure IndexDocument26 pagesAppendix A: Doppler Ultrasound and Ankle-Brachial Pressure IndexabigailNo ratings yet
- CT For PE Breathing Technique PRESENTATIONDocument17 pagesCT For PE Breathing Technique PRESENTATIONEka JuliantaraNo ratings yet
- Pulse OxymeterDocument9 pagesPulse OxymeterJisha JanardhanNo ratings yet
- Pulse OximetryDocument10 pagesPulse OximetryR.vijay100% (1)
- Pulse Oxymetery:: A Pulse Oximeter Is A Medical Device That Indirectly MonitorsDocument5 pagesPulse Oxymetery:: A Pulse Oximeter Is A Medical Device That Indirectly MonitorsPriyaNo ratings yet
- Respiratory Exam DetailedDocument12 pagesRespiratory Exam DetailedAshiniNo ratings yet
- Chapter 03: Techniques and Equipment For Physical AssessmentDocument6 pagesChapter 03: Techniques and Equipment For Physical AssessmentMay GabiNo ratings yet
- 8 PulseDocument5 pages8 Pulseزياد العنزيNo ratings yet
- A Beginners Guide To UltrasoundDocument12 pagesA Beginners Guide To Ultrasoundrdfj.muganhu1No ratings yet
- Unit 4Document17 pagesUnit 4Krunal ParmarNo ratings yet
- Cranial Nerve Examination OSCE GuideDocument34 pagesCranial Nerve Examination OSCE Guideluq9fifNo ratings yet
- Reflex Measurements: Quick GuideDocument10 pagesReflex Measurements: Quick GuidefilippobNo ratings yet
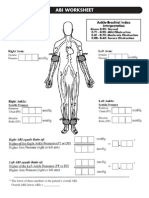
- Ankle-Brachial Index (ABI) PDFDocument4 pagesAnkle-Brachial Index (ABI) PDFHaris PapadopoulosNo ratings yet
- Ankle-Brachial Index-3 PDFDocument9 pagesAnkle-Brachial Index-3 PDFSarah HalanNo ratings yet
- Medical Application of Doppler TechniqueDocument7 pagesMedical Application of Doppler TechniqueCharlotte LambardiNo ratings yet
- Isuog Guias DopplerDocument7 pagesIsuog Guias DopplerrichardquinperNo ratings yet
- Medical ApplicationsDocument15 pagesMedical ApplicationsAakash RNo ratings yet
- Applying and Monitoring Pulse OximeterDocument4 pagesApplying and Monitoring Pulse OximeterPatricia Feb De Los SantosNo ratings yet
- How To Measure Ankle Brachial IndexDocument4 pagesHow To Measure Ankle Brachial Indexzaky0% (1)
- قياس ضغط الدم فى الكلابDocument6 pagesقياس ضغط الدم فى الكلابابراهيم عبداللهNo ratings yet
- Berzuela Lab 2Document9 pagesBerzuela Lab 2Ryan DagsilNo ratings yet
- 5B Assessing Apical Pulse-2Document4 pages5B Assessing Apical Pulse-2Marky RoqueNo ratings yet
- Assessing Peripheral PulseDocument3 pagesAssessing Peripheral Pulsekuroko senpaiNo ratings yet
- Mock Code Blue Teaching Your Role in A Code Blue / WhiteDocument3 pagesMock Code Blue Teaching Your Role in A Code Blue / Whiteapi-581417405No ratings yet
- Vital SignsDocument10 pagesVital SignsMuhammad FahmyNo ratings yet
- Power Point Pulse OximetryDocument11 pagesPower Point Pulse Oximetryanon_47299004No ratings yet
- Principles of Emergency NursingDocument4 pagesPrinciples of Emergency NursingShamera MahabassalNo ratings yet
- Doppler UltrasoundDocument2 pagesDoppler UltrasoundReiruki SawadaNo ratings yet
- Home Products Store Deals Faq & Download Contact Us: Eagleview™ Wireless Linear Probe UltrasoundDocument29 pagesHome Products Store Deals Faq & Download Contact Us: Eagleview™ Wireless Linear Probe UltrasoundJezreel P. GarcíaNo ratings yet
- Vital Signs - C21 - July 2013 - Without QuizDocument28 pagesVital Signs - C21 - July 2013 - Without Quizradwam123No ratings yet
- 9 Tips On How To Make A Good SOAPIEDocument7 pages9 Tips On How To Make A Good SOAPIEMagbanua Airene MarielNo ratings yet
- How To Use An AED - Automatic External DefibrillatorDocument4 pagesHow To Use An AED - Automatic External DefibrillatorMiguel BarreirosNo ratings yet
- Ankle Brachial IndexDocument5 pagesAnkle Brachial IndexFaskanita NadapdapNo ratings yet
- 2013 LVAD Field GuideDocument28 pages2013 LVAD Field Guidejerry3gowenNo ratings yet
- Using A Pulse OximeterDocument3 pagesUsing A Pulse OximeterErika ArceoNo ratings yet
- Pulse Oximetry and The Oxyhemoglobin Dissociation Curve: I. II. Iii. IV. A. B. C. D. V. VI. Vii. A. B. C. D. Viii. IX. XDocument11 pagesPulse Oximetry and The Oxyhemoglobin Dissociation Curve: I. II. Iii. IV. A. B. C. D. V. VI. Vii. A. B. C. D. Viii. IX. XDarryl Betts50% (2)
- SOMNOcheck MicroDocument2 pagesSOMNOcheck MicroEvangelosNo ratings yet
- VI Session - Testing Prior To Program. 1. Auditory System.: There Are Two Parts To A SoundDocument4 pagesVI Session - Testing Prior To Program. 1. Auditory System.: There Are Two Parts To A SoundAhmed HamdyNo ratings yet
- Pulse Ox I Buk FinalDocument25 pagesPulse Ox I Buk Finalabukhari0786No ratings yet
- FREE 2021 ACLS Study Guide - ACLS Made Easy!Document32 pagesFREE 2021 ACLS Study Guide - ACLS Made Easy!Alen ArguellesNo ratings yet
- Pulse OxymetryDocument4 pagesPulse OxymetryErryl Justine AdvinculaNo ratings yet
- Jawahar 1997Document4 pagesJawahar 1997Mohammed RickyNo ratings yet
- Case 6Document1 pageCase 6api-676122689No ratings yet
- Makalah Bahasa InggrisDocument2 pagesMakalah Bahasa InggrisOlga RevalinaNo ratings yet
- What Is A Pulse OximeterDocument2 pagesWhat Is A Pulse OximeterAmey NaikNo ratings yet
- Graphical Representation of Pulsed ArticleDocument6 pagesGraphical Representation of Pulsed ArticleAli RazaNo ratings yet
- Bimbingan ThoraksDocument71 pagesBimbingan ThoraksHedya Nadhrati SururaNo ratings yet
- Abi SheetsDocument2 pagesAbi Sheetszaky soewandi0% (1)
- Blood PressureDocument5 pagesBlood PressureJatinNo ratings yet
- What Is CPR?Document7 pagesWhat Is CPR?Harshal AachrekarNo ratings yet
- Measuring Blood PressureDocument9 pagesMeasuring Blood PressureGuru Raja ChowdaryNo ratings yet
- ME 224 Project: Lie Detector: June 6, 2003Document17 pagesME 224 Project: Lie Detector: June 6, 2003ajayikayodeNo ratings yet
- Indications: PurposeDocument13 pagesIndications: PurposeIRA ODETTE GATUSNo ratings yet
- Ankle Brachial Systolic IndexDocument9 pagesAnkle Brachial Systolic IndexAiman ArifinNo ratings yet
- The Waveform Control ButtonsDocument1 pageThe Waveform Control ButtonsPanagiotis MitsopoulosNo ratings yet
- UltrasoundMasterclass - Arteries - of - The - Legs - Handbook 70Document1 pageUltrasoundMasterclass - Arteries - of - The - Legs - Handbook 70Panagiotis MitsopoulosNo ratings yet
- Four Steps For Recording The Dorsalis Pedis Artery (DPA) PressuresDocument1 pageFour Steps For Recording The Dorsalis Pedis Artery (DPA) PressuresPanagiotis MitsopoulosNo ratings yet
- UltrasoundMasterclass - Arteries - of - The - Legs - Handbook 45Document1 pageUltrasoundMasterclass - Arteries - of - The - Legs - Handbook 45Panagiotis MitsopoulosNo ratings yet
- How To Interpret Audible and Analog WaveformsDocument1 pageHow To Interpret Audible and Analog WaveformsPanagiotis MitsopoulosNo ratings yet
- UltrasoundMasterclass - Arteries - of - The - Legs - Handbook 38Document1 pageUltrasoundMasterclass - Arteries - of - The - Legs - Handbook 38Panagiotis MitsopoulosNo ratings yet
- UltrasoundMasterclass - Arteries - of - The - Legs - Handbook 34Document1 pageUltrasoundMasterclass - Arteries - of - The - Legs - Handbook 34Panagiotis MitsopoulosNo ratings yet
- UltrasoundMasterclass - Arteries - of - The - Legs - Handbook 31Document1 pageUltrasoundMasterclass - Arteries - of - The - Legs - Handbook 31Panagiotis MitsopoulosNo ratings yet