You might also like
- The Menopause Lady: A Menopause Practitioner's Memoir of Life, Love, Breast Cancer, and Her Choice to Return to Estrogen.From EverandThe Menopause Lady: A Menopause Practitioner's Memoir of Life, Love, Breast Cancer, and Her Choice to Return to Estrogen.No ratings yet
- Sign of Hyperandrogenism PDFDocument6 pagesSign of Hyperandrogenism PDFmisbah_mdNo ratings yet
- Genetics of Male InfertilityDocument16 pagesGenetics of Male InfertilityMarcel MusteaNo ratings yet
- Lecture 20 Hormones and Infertility LectureDocument48 pagesLecture 20 Hormones and Infertility LectureJoseph Stans KasiryeNo ratings yet
- Interpretation of The Semen Analysis and Initial Male Factor ManagementDocument10 pagesInterpretation of The Semen Analysis and Initial Male Factor ManagementRosangela Mazariegos CastilloNo ratings yet
- Male Infertility, Diagnosis and Recent ManagementDocument77 pagesMale Infertility, Diagnosis and Recent ManagementDR SHASHWAT JANINo ratings yet
- Leah M. Schenk, MD Infertility Reproductive EndocrinologyDocument2 pagesLeah M. Schenk, MD Infertility Reproductive EndocrinologyLeah M. Schenk MD100% (2)
- IMLE Lecture on Obstetrics and Gynecology AnomaliesDocument69 pagesIMLE Lecture on Obstetrics and Gynecology AnomaliesTarek TarekNo ratings yet
- Female InfertilityDocument4 pagesFemale InfertilityAmar M AradhyaNo ratings yet
- Infertility PBLDocument11 pagesInfertility PBLcgalongNo ratings yet
- Male InfertilityDocument26 pagesMale InfertilitySahil VermaNo ratings yet
- Increase Sperm Count NaturallyDocument5 pagesIncrease Sperm Count Naturallyomomom2710No ratings yet
- Does Endometriosis Cause InfertilityDocument1 pageDoes Endometriosis Cause InfertilityLidia LadeaNo ratings yet
- Infertility CausesDocument3 pagesInfertility Causesapi-3733640No ratings yet
- Female Infertility - Causes and Their Diagnostic Tests - A ReviewDocument18 pagesFemale Infertility - Causes and Their Diagnostic Tests - A Reviewirfan aridNo ratings yet
- Azoospermia Guidelines PDFDocument7 pagesAzoospermia Guidelines PDFafifberlianNo ratings yet
- ESHRE RPL Guideline - 28112017 - FINAL PDFDocument154 pagesESHRE RPL Guideline - 28112017 - FINAL PDFAna MarianaNo ratings yet
- Scrotal Disease - 2Document47 pagesScrotal Disease - 2Hillary BushnellNo ratings yet
- Nursing-Interventions MCN For Infertility MenDocument2 pagesNursing-Interventions MCN For Infertility MenRio DanteNo ratings yet
- Evaluation of The Azoospermic Male: A Committee OpinionDocument6 pagesEvaluation of The Azoospermic Male: A Committee OpinionRossana RoussNo ratings yet
- Causes of Female InfertilityDocument7 pagesCauses of Female InfertilityNatanael SusantoNo ratings yet
- ACOG Perinatal Care Guidelines SummaryDocument4 pagesACOG Perinatal Care Guidelines SummaryMega KahdinaNo ratings yet
- Practical Management of Male InfertilityDocument70 pagesPractical Management of Male InfertilityIosub LicaClaudiu100% (1)
- Seminar On InfertilityDocument17 pagesSeminar On InfertilityN vineethaNo ratings yet
- Ovulation TestingDocument5 pagesOvulation Testingpriya vermaNo ratings yet
- PDE-5 Inhibitors - Drug Class ReviewDocument7 pagesPDE-5 Inhibitors - Drug Class ReviewTkt Sheik AbdullahNo ratings yet
- Medad Andrology Special Note NMT13 PDFDocument70 pagesMedad Andrology Special Note NMT13 PDFSelim TarekNo ratings yet
- Infertility IDocument36 pagesInfertility Idr_asaleh100% (1)
- Amenorrhea WorkupDocument10 pagesAmenorrhea WorkupHaoKeat HoeNo ratings yet
- Cure For InfertilityDocument8 pagesCure For Infertilitykm_ananthNo ratings yet
- Fertility & ART GuideDocument92 pagesFertility & ART GuideSundar NarayananNo ratings yet
- Graves' Disease & PregnancyDocument19 pagesGraves' Disease & Pregnancyrajan kumar100% (1)
- Infertility 1Document2 pagesInfertility 1Mikhaela Andree MarianoNo ratings yet
- Male and Female Infertility GuideDocument35 pagesMale and Female Infertility GuideJalajarani AridassNo ratings yet
- Women'S Health Talk Kozri Lo Lasante Madanm: DR Annabelle D. Marie MO Ministry of Health SeychellesDocument32 pagesWomen'S Health Talk Kozri Lo Lasante Madanm: DR Annabelle D. Marie MO Ministry of Health SeychellesAnna Diana MariaNo ratings yet
- Intrahepatic Cholestasis of Pregnancy: Clinical Obstetrics and Gynecology Volume 63, Number 1, 134-151Document19 pagesIntrahepatic Cholestasis of Pregnancy: Clinical Obstetrics and Gynecology Volume 63, Number 1, 134-151Von BernalNo ratings yet
- Investigation InfertilityDocument44 pagesInvestigation InfertilityDenisNo ratings yet
- Infertility Guide: Causes, Diagnosis and TreatmentDocument44 pagesInfertility Guide: Causes, Diagnosis and TreatmentFemi AustinNo ratings yet
- Precociou S Puberty: BY Vishnupriya Ravimohandoss Year-6 Group-1Document31 pagesPrecociou S Puberty: BY Vishnupriya Ravimohandoss Year-6 Group-1Priya RaviNo ratings yet
- Table 4.1 AFS Classifi Cation System (: The Embryological-Clinical Classifi CationDocument111 pagesTable 4.1 AFS Classifi Cation System (: The Embryological-Clinical Classifi CationArya Syafaromania RachmaNo ratings yet
- Infertility Latest 14.02.2010.Document13 pagesInfertility Latest 14.02.2010.brilliantpaulNo ratings yet
- InfertilityDocument23 pagesInfertilityZahra Alaradi100% (2)
- StratOG Vaginal BreechDocument17 pagesStratOG Vaginal BreechNalin AbeysingheNo ratings yet
- 1st & 2nd Trimester Pregnancy LossDocument48 pages1st & 2nd Trimester Pregnancy LossAbdullah EssaNo ratings yet
- The Use of Aromatase Inhibitors in Infertility and GynecologyDocument9 pagesThe Use of Aromatase Inhibitors in Infertility and Gynecologyalan lowusNo ratings yet
- Fertility: Assessment and Treatment For People With Fertility ProblemsDocument4 pagesFertility: Assessment and Treatment For People With Fertility ProblemsPatrick CoghlanNo ratings yet
- Definition of InfertilityDocument6 pagesDefinition of InfertilityRatiram LilhareNo ratings yet
- HRT Formulary and Treatment Guidance: (Apc Clindoc 010)Document8 pagesHRT Formulary and Treatment Guidance: (Apc Clindoc 010)psdsportsdocNo ratings yet
- Prostate and Seminal VesiclesDocument83 pagesProstate and Seminal Vesiclesgreg_enricoNo ratings yet
- Management of Polycystic Ovary Syndrome in Case ofDocument18 pagesManagement of Polycystic Ovary Syndrome in Case ofMelati PratiwiNo ratings yet
- The Reproductive SystemDocument266 pagesThe Reproductive SystemNatia DemetradzeNo ratings yet
- Nurs 5002 - Case Study 5Document15 pagesNurs 5002 - Case Study 5api-308904543No ratings yet
- A Case Report of Primary Female Infertility Treated With HomoeopathyDocument6 pagesA Case Report of Primary Female Infertility Treated With HomoeopathyVinitha JobyNo ratings yet
- AmenorrheaDocument23 pagesAmenorrheaKarmmanya Razahani PurnamaNo ratings yet
- Intrahepatic Cholestasis of PregnancyDocument19 pagesIntrahepatic Cholestasis of PregnancyAlexander Vasquez TorresNo ratings yet
- Vulvovaginal Health & HygieneDocument131 pagesVulvovaginal Health & HygieneJasmine SardanaNo ratings yet
- Infertility: Reshmi SibyDocument80 pagesInfertility: Reshmi SibySusan ThomasNo ratings yet
- Assessment and Management of Women With Polycystic Ovary Syndrome (PCOS)Document17 pagesAssessment and Management of Women With Polycystic Ovary Syndrome (PCOS)Triratna FauziahNo ratings yet
- IPD Patient History ChecklistDocument2 pagesIPD Patient History ChecklistdrjriNo ratings yet
- Objectives:: Surgery Communications Primer Page 1 of 17Document17 pagesObjectives:: Surgery Communications Primer Page 1 of 17Titoun LettounNo ratings yet
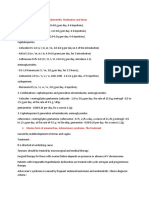
- Treatment of Acute Endometritis. Medication and DosesDocument3 pagesTreatment of Acute Endometritis. Medication and DosesTitoun LettounNo ratings yet
- 25490874Document563 pages25490874Titoun LettounNo ratings yet
- NHMRC Research Achievements - SUMMARY: Funded Research Into Injury Related Research ENDING 2004 TO 2013Document521 pagesNHMRC Research Achievements - SUMMARY: Funded Research Into Injury Related Research ENDING 2004 TO 2013Titoun LettounNo ratings yet
- Breast Cancer Prevention and Early DetectionDocument23 pagesBreast Cancer Prevention and Early DetectionLizha EinsteinNo ratings yet
- Values and Ethics For The 21first CenturyDocument566 pagesValues and Ethics For The 21first CenturyStanislas100% (1)
- What Is Pathophysiology?Document168 pagesWhat Is Pathophysiology?Titoun LettounNo ratings yet
- Intro To Mycology Prelims2Document47 pagesIntro To Mycology Prelims2Annika AbadNo ratings yet
- Multiple MyelomaDocument23 pagesMultiple MyelomaRameshKrishnanNo ratings yet
- Canonum de Ius Virtus Naturae PDFDocument216 pagesCanonum de Ius Virtus Naturae PDFsimon martin ryderNo ratings yet
- Baileys 13th Ed Chapter QuestionsDocument79 pagesBaileys 13th Ed Chapter QuestionsrhymeNo ratings yet
- Journal of Medicinal Chemistry (2011), 54, 7453-7463Document11 pagesJournal of Medicinal Chemistry (2011), 54, 7453-7463James TianNo ratings yet
- The Importance of a Healthy LifestyleDocument2 pagesThe Importance of a Healthy LifestyleAnonymous kF9IXBP100% (1)
- MсKee's V.1 P.1Document376 pagesMсKee's V.1 P.1Jonnie Rose Louise WeeNo ratings yet
- Optic AtrophyDocument16 pagesOptic AtrophyAvesNo ratings yet
- Pi Is 0145212611003705Document7 pagesPi Is 0145212611003705nikunj_patel_43No ratings yet
- Literature Review On BacteriaDocument9 pagesLiterature Review On Bacteriaea83xjp7100% (1)
- HiperbillirubinemiaDocument7 pagesHiperbillirubinemiaBrenda RomeroNo ratings yet
- Cohort Study DesignDocument25 pagesCohort Study DesignAmeerah MantawilNo ratings yet
- MHC MoleculeDocument45 pagesMHC MoleculeShah NAWAZNo ratings yet
- Breast Cancer: Katherine Macgillivray & Melissa PoirierDocument62 pagesBreast Cancer: Katherine Macgillivray & Melissa PoirierJonathan Darell WijayaNo ratings yet
- Assessment and Determination of Optimum Concentration of Streptomycin and Kanamycin As Selective Agents in Peppermint (MenthaDocument6 pagesAssessment and Determination of Optimum Concentration of Streptomycin and Kanamycin As Selective Agents in Peppermint (MenthaMonaia YehiaNo ratings yet
- Natural selection simulation examines adaptation of imaginary organismDocument13 pagesNatural selection simulation examines adaptation of imaginary organismVeyari RamirezNo ratings yet
- EnzymesDocument13 pagesEnzymesManjusha KondepudiNo ratings yet
- Dr. Huma HCV PresentationDocument27 pagesDr. Huma HCV Presentationkaram aliNo ratings yet
- Master Nauli for a Strong Core and DigestionDocument7 pagesMaster Nauli for a Strong Core and DigestionOVVCMOULINo ratings yet
- Biologicals and Biosimilars: An OverviewDocument8 pagesBiologicals and Biosimilars: An OverviewBaru Chandrasekhar RaoNo ratings yet
- Antisocial Personality Disorder by SlidesgoDocument41 pagesAntisocial Personality Disorder by Slidesgosssnehasinha05No ratings yet
- Agilent Bioanalyzer Application CompediumDocument104 pagesAgilent Bioanalyzer Application CompediumShi Jie Pang100% (1)
- Ovine Pulmonary Adenocarcinoma: (Adenomatosis)Document6 pagesOvine Pulmonary Adenocarcinoma: (Adenomatosis)WormInchNo ratings yet
- Review: DevitaDocument469 pagesReview: DevitaRabiya TahseenNo ratings yet
- Tenofovir Disoproxil Fumarate: Therese M. Chapman, Jane K. Mcgavin and Stuart NobleDocument12 pagesTenofovir Disoproxil Fumarate: Therese M. Chapman, Jane K. Mcgavin and Stuart NobleBagusHibridaNo ratings yet
- Cambridge International AS & A Level: Biology 9700/22Document16 pagesCambridge International AS & A Level: Biology 9700/22Hussain AlAliNo ratings yet
- A Review Apocynum VenetumDocument8 pagesA Review Apocynum VenetumAfifah Dwi CahyaniNo ratings yet
- Celiac DiseaseDocument14 pagesCeliac Diseaseapi-355698448100% (1)
- Antidiarrheal DrugsDocument7 pagesAntidiarrheal Drugsmwaithira71682No ratings yet
- Singh 2018Document16 pagesSingh 2018Georgiana BunghiuzNo ratings yet