You might also like
- Pancreatic Enzyme Extract Improves Survival in Murine Pancreatic CancerDocument12 pagesPancreatic Enzyme Extract Improves Survival in Murine Pancreatic CancerRexGoliathNo ratings yet
- Medicine 1Document2 pagesMedicine 1ÇağlaNo ratings yet
- 74 FullDocument3 pages74 FullNoel Saúl Argüello SánchezNo ratings yet
- NPCDocument8 pagesNPCArsy Mira PertiwiNo ratings yet
- Chemotherapy of Canine Hemangiosarcoma With Doxorubicin and CyclophosphamideDocument7 pagesChemotherapy of Canine Hemangiosarcoma With Doxorubicin and CyclophosphamideLeidy CriolloNo ratings yet
- Etm 08 05 1535Document4 pagesEtm 08 05 1535Lumaquin, Reynalyn RuanoNo ratings yet
- Magic TrailDocument10 pagesMagic Trailchootu509No ratings yet
- CCR3-5-1210Document3 pagesCCR3-5-1210NovelNo ratings yet
- NejmoaDocument9 pagesNejmoamangosidNo ratings yet
- Clinical-Liver, Pancreas, and Biliary TractDocument8 pagesClinical-Liver, Pancreas, and Biliary TractKirsten HartmanNo ratings yet
- Adjuvant Systemic Therapies in Breast CancerDocument19 pagesAdjuvant Systemic Therapies in Breast CancerSapp ChaamaraNo ratings yet
- P ('t':'3', 'I':'176969959') D '' Var B Location Settimeout (Function ( If (Typeof Window - Iframe 'Undefined') ( B.href B.href ) ), 15000)Document8 pagesP ('t':'3', 'I':'176969959') D '' Var B Location Settimeout (Function ( If (Typeof Window - Iframe 'Undefined') ( B.href B.href ) ), 15000)Cecep Saeful HudaNo ratings yet
- Fol Firin OxDocument11 pagesFol Firin OxGuilherme SalgadoNo ratings yet
- New England Journal Medicine: The ofDocument11 pagesNew England Journal Medicine: The ofJosé Ignacio Rinaldi CentresNo ratings yet
- Chemotherapy-And Cancer-Related Nausea and Vomiting: Table IDocument12 pagesChemotherapy-And Cancer-Related Nausea and Vomiting: Table IVayu PuthraNo ratings yet
- Lansoprazole For The Prevention of Recurrences of Ulcer Complications From Long-Term Low-Dose Aspirin UseDocument6 pagesLansoprazole For The Prevention of Recurrences of Ulcer Complications From Long-Term Low-Dose Aspirin UseAmalia NandiaNo ratings yet
- Pemphigus VulgarusDocument9 pagesPemphigus Vulgarusmedical studentNo ratings yet
- Ifosfamide in Soft Tissue Sarcoma: Patients and MethodsDocument4 pagesIfosfamide in Soft Tissue Sarcoma: Patients and MethodsRashid SiddiqueNo ratings yet
- JCO 2005 Pink 6809 11Document3 pagesJCO 2005 Pink 6809 11claudiaNo ratings yet
- Pelvic Ewing Sarcoma: A Retrospective Analysis of 241 CasesDocument9 pagesPelvic Ewing Sarcoma: A Retrospective Analysis of 241 CasesHassan AlmasriNo ratings yet
- Retrospective Study of Adverse Events of Chemotherapy in CatsDocument12 pagesRetrospective Study of Adverse Events of Chemotherapy in CatsElvira ViraNo ratings yet
- Khosrowmomtaz 1998Document8 pagesKhosrowmomtaz 1998Mariana JuravleNo ratings yet
- Inappropriate Usage of Intravenous Proton Pump Inhibitors and Associated Factors in A High Complexity Hospital in BrazilDocument7 pagesInappropriate Usage of Intravenous Proton Pump Inhibitors and Associated Factors in A High Complexity Hospital in BrazilJosivaneMarquesNo ratings yet
- Cardiac Toxicity Following High-Dose Cyclophosphamide, Cisplatin, and BCNU (STAMP-I) For Breast CancerDocument6 pagesCardiac Toxicity Following High-Dose Cyclophosphamide, Cisplatin, and BCNU (STAMP-I) For Breast CancerNenad MladenovicNo ratings yet
- 1 PBDocument3 pages1 PBMartynaNo ratings yet
- Advanced Colorectal Cancer: ESMO Clinical Practice Guidelines For TreatmentDocument5 pagesAdvanced Colorectal Cancer: ESMO Clinical Practice Guidelines For TreatmentMohamed OsamaNo ratings yet
- Methylnaltrexone-Associated Bowel Perforation in Postoperative Opioid-Induced Constipation and Ogilvie Syndrome: A Case ReportDocument3 pagesMethylnaltrexone-Associated Bowel Perforation in Postoperative Opioid-Induced Constipation and Ogilvie Syndrome: A Case ReportElizabeth ToapantaNo ratings yet
- Document PDFDocument10 pagesDocument PDFMichael TanNo ratings yet
- Role of Imaging in Clinical Islet TransplantationDocument15 pagesRole of Imaging in Clinical Islet TransplantationR BNo ratings yet
- Spontaneous Regression of Pancreatic Cancer: A Case Report and Literature ReviewDocument5 pagesSpontaneous Regression of Pancreatic Cancer: A Case Report and Literature ReviewHitomi-No ratings yet
- Ibrt 06 I 4 P 232Document2 pagesIbrt 06 I 4 P 232Aditia Nata KusumaNo ratings yet
- Moxifloxaxin For CAPDocument9 pagesMoxifloxaxin For CAPmateri posNo ratings yet
- CAPECITABINEOXALIPLATINODocument8 pagesCAPECITABINEOXALIPLATINOFrancisco BetancourtNo ratings yet
- An Open-Label Pilot Study of Adrenocorticotrophic Hormone in The Treatment of IgA Nephropathy at High Risk of Progression Zand2019Document8 pagesAn Open-Label Pilot Study of Adrenocorticotrophic Hormone in The Treatment of IgA Nephropathy at High Risk of Progression Zand2019Calvin Tanuwijaya Stick BolaNo ratings yet
- Use of Linezolid To Treat MRSP Bacteremia and Discospondylitis in A DogDocument6 pagesUse of Linezolid To Treat MRSP Bacteremia and Discospondylitis in A DogValentina Hincapié GiraldoNo ratings yet
- Case Report On Ulcerative Colitis in 16 Year GirlDocument4 pagesCase Report On Ulcerative Colitis in 16 Year GirlAbdullah KhanNo ratings yet
- 559 FullDocument5 pages559 FullSukhvinder Singh RanaNo ratings yet
- Jurnal UveitisDocument6 pagesJurnal UveitisWidodo WidoNo ratings yet
- Safety and Efficacy of Levofloxacin Versus Rifampicin in Tuberculous Meningitis: An Open-Label Randomized Controlled TrialDocument6 pagesSafety and Efficacy of Levofloxacin Versus Rifampicin in Tuberculous Meningitis: An Open-Label Randomized Controlled TrialSri AgustinaNo ratings yet
- Herbal-Drug Interaction Induced Rhabdomyolysis in A Liposarcoma Patient Receiving TrabectedinDocument5 pagesHerbal-Drug Interaction Induced Rhabdomyolysis in A Liposarcoma Patient Receiving TrabectedinSuci HandayaniNo ratings yet
- Clinical Outcomes of Golimumab As First, Second or Third Anti-TNF Agent in Patients With Moderate-to-Severe Ulcerative ColitisDocument9 pagesClinical Outcomes of Golimumab As First, Second or Third Anti-TNF Agent in Patients With Moderate-to-Severe Ulcerative ColitisDiana GCNo ratings yet
- 1097 0142 28197410 2934 3A4 3C985 3A 3aaid cncr2820340402 3e3.0.co 3B2 U PDFDocument8 pages1097 0142 28197410 2934 3A4 3C985 3A 3aaid cncr2820340402 3e3.0.co 3B2 U PDFLata DeshmukhNo ratings yet
- Fernandez 1989Document2 pagesFernandez 1989Muhammad IqsanNo ratings yet
- Squamous Cell Carcinoma of The PancreasDocument2 pagesSquamous Cell Carcinoma of The Pancreaserick_khristianNo ratings yet
- General Surgery: Ruptured Liver Abscess: A Novel Surgical TechniqueDocument3 pagesGeneral Surgery: Ruptured Liver Abscess: A Novel Surgical TechniqueRahul SinghNo ratings yet
- Alicaforsen For The Treatment of Inflammatory Bowel DiseaseDocument25 pagesAlicaforsen For The Treatment of Inflammatory Bowel Diseaseinfinity TangNo ratings yet
- Anak Jurnal 2Document8 pagesAnak Jurnal 2RamaNo ratings yet
- Mahaseth 2013Document5 pagesMahaseth 2013Paulina Sobarzo VegaNo ratings yet
- J. Kalita., Et Al. 2014Document6 pagesJ. Kalita., Et Al. 2014Ubaida AssalwaNo ratings yet
- Antifungal Step-Down Therapy Based On HospitalDocument8 pagesAntifungal Step-Down Therapy Based On Hospitalvaithy71No ratings yet
- Scar Pigna To 2010Document32 pagesScar Pigna To 2010anon_535071452No ratings yet
- Top Trials in Gastroenterology & HepatologyFrom EverandTop Trials in Gastroenterology & HepatologyRating: 4.5 out of 5 stars4.5/5 (7)
- Nej Mo A 1207756Document11 pagesNej Mo A 1207756Mrs_gumugumuNo ratings yet
- Af13e6df 9c91 4284 A3ae Feb2bacbcba4Document7 pagesAf13e6df 9c91 4284 A3ae Feb2bacbcba4alberto cabelloNo ratings yet
- Management of Perforated Appendicitis in Children: A Decade of Aggressive TreatmentDocument5 pagesManagement of Perforated Appendicitis in Children: A Decade of Aggressive Treatmentapi-308365861No ratings yet
- Phase II Trial of Curcumin in Patients With Advanced Pancreatic Cancer.Document10 pagesPhase II Trial of Curcumin in Patients With Advanced Pancreatic Cancer.João FrancoNo ratings yet
- Interaction Between Warfarin and Tamoxifen A Case ReportDocument3 pagesInteraction Between Warfarin and Tamoxifen A Case ReportBalqis BaslemanNo ratings yet
- Question 1 of 35Document130 pagesQuestion 1 of 35Ahmed SamirNo ratings yet
- Therapy in TuberculosisDocument4 pagesTherapy in TuberculosisSamir SkejicNo ratings yet
- Inherited Abnormalities of CoagulationDocument23 pagesInherited Abnormalities of CoagulationZai Rojas OrtizNo ratings yet
- CT Findings of Chemotherapy-Induced Toxicity What Radiologists Need To Know About The Clinical and Radiologic Manifestations of Chemotherapy ToxicityDocument16 pagesCT Findings of Chemotherapy-Induced Toxicity What Radiologists Need To Know About The Clinical and Radiologic Manifestations of Chemotherapy ToxicityZai Rojas OrtizNo ratings yet
- Targeted Thromboelastographic (TEG) Blood Component and Pharmacologic Hemostatic Therapy in Traumatic and Acquired CoagulopathyDocument17 pagesTargeted Thromboelastographic (TEG) Blood Component and Pharmacologic Hemostatic Therapy in Traumatic and Acquired CoagulopathyZai Rojas OrtizNo ratings yet
- HHS Public Access: Chemotherapy-Induced Peripheral Neuropathy: A Current ReviewDocument17 pagesHHS Public Access: Chemotherapy-Induced Peripheral Neuropathy: A Current ReviewPablo Sebastián SaezNo ratings yet
- Chinese Medicinal Herbs To Treat The Side-Effects of Chemotherapy in Breast Cancer PatientsDocument32 pagesChinese Medicinal Herbs To Treat The Side-Effects of Chemotherapy in Breast Cancer PatientsZai Rojas OrtizNo ratings yet
- A Case of 5-Fluorouracil-Induced Cardiac ArrestDocument6 pagesA Case of 5-Fluorouracil-Induced Cardiac ArrestZai Rojas OrtizNo ratings yet
- Rheumatoid Arthritis Drug StudyDocument2 pagesRheumatoid Arthritis Drug StudyChristaNo ratings yet
- Depression and Diabetes Slides ENGDocument20 pagesDepression and Diabetes Slides ENGMaria Magdalena Dumitru100% (1)
- ICMR GuidelinesType2diabetes2018 0Document82 pagesICMR GuidelinesType2diabetes2018 0VISHWANATH MARSHIVANIKARNo ratings yet
- ShockDocument124 pagesShockRahman Mukti AjiNo ratings yet
- 14.4 Cancer ScreeningDocument2 pages14.4 Cancer Screeningvenkat krishnanNo ratings yet
- Kawasaki Disease Case ReportDocument17 pagesKawasaki Disease Case ReportAlvaro Villarejo PérezNo ratings yet
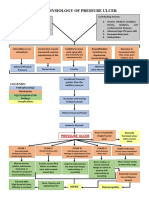
- Pathophysiology of Pressure UlcerDocument1 pagePathophysiology of Pressure UlcerSTORAGE FILENo ratings yet
- Hernia - Surgery PrecisDocument1 pageHernia - Surgery PrecisSherif WagdyNo ratings yet
- Corona Virus (Covid19) : The Grim RealityDocument6 pagesCorona Virus (Covid19) : The Grim RealityGenevieve GayosoNo ratings yet
- Aleukemic LeukemiaDocument3 pagesAleukemic LeukemialilisNo ratings yet
- Kidney DiseasesDocument93 pagesKidney DiseasesDoreen NNo ratings yet
- About Rubella: VaccineDocument5 pagesAbout Rubella: VaccinejudssalangsangNo ratings yet
- Trauma Thoraks PDFDocument86 pagesTrauma Thoraks PDFMiftahurrahmiNo ratings yet
- 3rd Year Bcqs Hhhpathology-2Document38 pages3rd Year Bcqs Hhhpathology-2Hira PanhwerNo ratings yet
- Endocrine NCLEX PN Pract & ANS Questions IIDocument13 pagesEndocrine NCLEX PN Pract & ANS Questions IIYA HONo ratings yet
- Creutzfeldt-Jakob Disease (CJD)Document10 pagesCreutzfeldt-Jakob Disease (CJD)Thicc ManNo ratings yet
- Nutritional Epidemiology: Reference: Nutrition Epidemiology by Walter WilletDocument24 pagesNutritional Epidemiology: Reference: Nutrition Epidemiology by Walter WilletMarelign TilahunNo ratings yet
- Alternative Health & Herbs Remedies 425 Jackson SE, Albany, OR 97321 1-541-791-8400Document159 pagesAlternative Health & Herbs Remedies 425 Jackson SE, Albany, OR 97321 1-541-791-8400Marvin T Verna100% (2)
- Jabeen & TahirDocument12 pagesJabeen & TahirSanaNo ratings yet
- Emerging Infectious DiseasesDocument175 pagesEmerging Infectious Diseasesmani100% (2)
- New Health Care Clinical: Laboratory SrinagarDocument1 pageNew Health Care Clinical: Laboratory SrinagarRajaNo ratings yet
- Drug Name Gemcitabine: Synonym (S) : Common Trade Name (S) : ClassificationDocument8 pagesDrug Name Gemcitabine: Synonym (S) : Common Trade Name (S) : ClassificationOka Robi MuhammadNo ratings yet
- Appendix: Flow Charts and Treatment TablesDocument20 pagesAppendix: Flow Charts and Treatment TablesLeon LellaNo ratings yet
- What Is Heart Bypass SurgeryDocument10 pagesWhat Is Heart Bypass SurgeryVanitha AlagarsamyNo ratings yet
- Proper Fluid Therapy, Vasopressors, and Inotropic - Dr. VidyaDocument40 pagesProper Fluid Therapy, Vasopressors, and Inotropic - Dr. VidyaTinton PristiantoNo ratings yet
- Non-Sickle HB Variants.091611Document44 pagesNon-Sickle HB Variants.091611Sumihar PasaribuNo ratings yet
- Pho Meds ListDocument1 pagePho Meds Listmister emdiNo ratings yet
- THC AspergerDocument168 pagesTHC AspergerMICHAELNo ratings yet
- SPECIMEN COLLECTION and Processing For BACTERIOLOGY PDFDocument19 pagesSPECIMEN COLLECTION and Processing For BACTERIOLOGY PDFLPDF010596No ratings yet
- Assignment 1 Part 1 A1Document10 pagesAssignment 1 Part 1 A1garrenaNo ratings yet