You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5807)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (842)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (346)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Project Human FlagDocument41 pagesProject Human FlagStefan Adrian100% (3)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Teach Me AnatomyDocument17 pagesTeach Me AnatomyMar Kristian Vero Lumen100% (1)
- Cardinal Points in AcupunctureDocument2 pagesCardinal Points in Acupuncturemonicq77100% (1)
- Nasm Study Guide PDF 2016 Nasm CPTDocument54 pagesNasm Study Guide PDF 2016 Nasm CPTAlonzo Mark100% (7)
- Free Software Applications For Authors For Writing.9Document6 pagesFree Software Applications For Authors For Writing.9stone heartNo ratings yet
- Bone LectureDocument50 pagesBone LectureHenry Rodríguez GuzmánNo ratings yet
- Overview of Muscle Tissues: Key ChoicesDocument36 pagesOverview of Muscle Tissues: Key ChoicesJustine Mae AbajoNo ratings yet
- D M M A: R Ichael C UliffeDocument11 pagesD M M A: R Ichael C UliffeJaime Oso ThompsonNo ratings yet
- Principios de Protección ArticularDocument6 pagesPrincipios de Protección ArticularLuis Camilo QuintoNo ratings yet
- The Muscular System The Muscular System: © 2018 Pearson Education, Ltd. 1Document14 pagesThe Muscular System The Muscular System: © 2018 Pearson Education, Ltd. 1lourd nabNo ratings yet
- Seeley's Chapter 6 Skeletal SystemDocument80 pagesSeeley's Chapter 6 Skeletal SystemThea MallariNo ratings yet
- Surgical Approach To The Triangular Fibrocartilage Complex - Marc Garcia EliasDocument7 pagesSurgical Approach To The Triangular Fibrocartilage Complex - Marc Garcia EliasDario AlarconNo ratings yet
- The SkepasDocument24 pagesThe Skepasprince kumarNo ratings yet
- Blood Supply of Lower LimbDocument27 pagesBlood Supply of Lower LimbabdullahNo ratings yet
- Surgery - Dychioco - Musculo Skeletal InjuriesDocument79 pagesSurgery - Dychioco - Musculo Skeletal Injuries3rd yrsNo ratings yet
- Second Semester - Musculoskeletal System: 1 Week Questions (Mcqs/Essay) & AnswersDocument36 pagesSecond Semester - Musculoskeletal System: 1 Week Questions (Mcqs/Essay) & AnswersHashim OmarNo ratings yet
- BCS 1 Dan BCS 2Document5 pagesBCS 1 Dan BCS 2Aisyah SyahidahNo ratings yet
- Crawling Exercise: Dr. Hiral Katakia MPT (Neuro)Document20 pagesCrawling Exercise: Dr. Hiral Katakia MPT (Neuro)Rohan LAl100% (3)
- Shoulder Press Bench PlanDocument44 pagesShoulder Press Bench PlanDiego ChavesNo ratings yet
- Leukotape K 03 Advanced E 12Document58 pagesLeukotape K 03 Advanced E 12Diego TrocheNo ratings yet
- Kartu Hapalan Osteology Anatomy 2018: Nama: .. NIM: .. PembimbingDocument8 pagesKartu Hapalan Osteology Anatomy 2018: Nama: .. NIM: .. PembimbingzannubanabilahNo ratings yet
- Tibio Fibular JointsDocument22 pagesTibio Fibular JointsSamiha HaqNo ratings yet
- 1st Case Musculoskeletal - AuliaDocument25 pages1st Case Musculoskeletal - AuliaAULIA ANGRAININo ratings yet
- MSK CT Protocols Overview, Jan 2018Document26 pagesMSK CT Protocols Overview, Jan 2018grergergr grregrgrebNo ratings yet
- Upper Cross Syndrome Dr. Jeff Luebbe 2-05-12Document9 pagesUpper Cross Syndrome Dr. Jeff Luebbe 2-05-12Simo AsterNo ratings yet
- OS Control Question List.Document83 pagesOS Control Question List.Jericho von NazarethNo ratings yet
- Sample Muscular System WorksheetsDocument8 pagesSample Muscular System WorksheetsAbigailBarrionGutierrezNo ratings yet
- Fibula Wei 2018Document11 pagesFibula Wei 2018Rares CraciunNo ratings yet
- Workout BeggDocument8 pagesWorkout BeggemileNo ratings yet
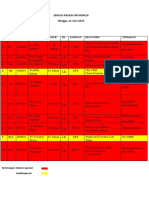
- Sensus Pasien Orthopedi Minggu, 21 JULI 2019: No Bed No - RM Nama Umur JK Jaminan Diagnosis TindakanDocument3 pagesSensus Pasien Orthopedi Minggu, 21 JULI 2019: No Bed No - RM Nama Umur JK Jaminan Diagnosis TindakanWa JulianiNo ratings yet