You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Bringing Down High Blood Pressure-ManteshDocument298 pagesBringing Down High Blood Pressure-Manteshzulmohd1100% (3)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- PE11 - MELC 4 Module 4 - Week7 For Teacher PDFDocument24 pagesPE11 - MELC 4 Module 4 - Week7 For Teacher PDFRommel Cando80% (5)
- Aortic AneurysmDocument61 pagesAortic AneurysmSurya Budikusuma64% (11)
- Biology NMAT Notes AnatomyCirculatory and RespiratoryDocument13 pagesBiology NMAT Notes AnatomyCirculatory and RespiratoryMa. Teresa M. AbainzaNo ratings yet
- Broda Barnes Solved Riddle Heart AttacksDocument47 pagesBroda Barnes Solved Riddle Heart AttacksArsalan Khan100% (1)
- EMPYEMA ReviewDocument95 pagesEMPYEMA ReviewBijay KumarNo ratings yet
- Hypertensive Heart DiseaseDocument33 pagesHypertensive Heart Diseaserini_adriani6817No ratings yet
- Answers To The Cambridge Checkpoint Science 2Document28 pagesAnswers To The Cambridge Checkpoint Science 2Nur Dina ZaulkifleeNo ratings yet
- HascvdDocument92 pagesHascvdbatangas_ynad_29900% (1)
- Arteriovenous Fistula Maturation in Prevalent Hymodialysis PatientsDocument9 pagesArteriovenous Fistula Maturation in Prevalent Hymodialysis PatientsBijay KumarNo ratings yet
- Factors Associated With Early Failure of Arteriovenous FistulaeDocument7 pagesFactors Associated With Early Failure of Arteriovenous FistulaeBijay KumarNo ratings yet
- Moving Beyond The AssumedDocument3 pagesMoving Beyond The AssumedBijay KumarNo ratings yet
- Hemodialysis Vascular Access Construction in The UpperDocument6 pagesHemodialysis Vascular Access Construction in The UpperBijay KumarNo ratings yet
- International Differences in The Location and Use of Arteriovenous Accesses Created For Hemodialysis Results From The Dialysis Outcomes and Practice Patterns Study DOPPSDocument10 pagesInternational Differences in The Location and Use of Arteriovenous Accesses Created For Hemodialysis Results From The Dialysis Outcomes and Practice Patterns Study DOPPSBijay KumarNo ratings yet
- Complications of The Arteriovenous FistulaDocument12 pagesComplications of The Arteriovenous FistulaBijay KumarNo ratings yet
- Evaluation of Arteriovenous Fistulas Made With The Diamond-ShapedDocument4 pagesEvaluation of Arteriovenous Fistulas Made With The Diamond-ShapedBijay KumarNo ratings yet
- Pathophysiology and Classification PDFDocument25 pagesPathophysiology and Classification PDFBijay KumarNo ratings yet
- Murphy Et Al-2016-Pediatric Anesthesia PDFDocument5 pagesMurphy Et Al-2016-Pediatric Anesthesia PDFBijay KumarNo ratings yet
- A New Technique For Microvascular Anastomosis Eversion With 3 Horizontal Mattress SuturesDocument4 pagesA New Technique For Microvascular Anastomosis Eversion With 3 Horizontal Mattress SuturesBijay KumarNo ratings yet
- A New Combined Interrupted-Continuous Anastomosis TechniqueDocument6 pagesA New Combined Interrupted-Continuous Anastomosis TechniqueBijay KumarNo ratings yet
- Surgery For Emphysema PDFDocument2 pagesSurgery For Emphysema PDFBijay KumarNo ratings yet
- Medical Management of Chronic Obstructive PDFDocument15 pagesMedical Management of Chronic Obstructive PDFBijay KumarNo ratings yet
- Heart Dissection Lab Report Guide2Document7 pagesHeart Dissection Lab Report Guide2Dylan FernandezNo ratings yet
- Implication of Location of The Ascending Mental Artery at The Chin Injection PointDocument7 pagesImplication of Location of The Ascending Mental Artery at The Chin Injection Pointmarta.sofiiiaNo ratings yet
- Kamota Mock Examinations 2023 s.6 BiologyDocument18 pagesKamota Mock Examinations 2023 s.6 Biologymungufeni amosNo ratings yet
- Act 5Document10 pagesAct 5Rose CostaNo ratings yet
- Plus One English G7 Revision 1Document28 pagesPlus One English G7 Revision 1Hillary DzudaNo ratings yet
- Answers 8A Food, Glorious Food!Document58 pagesAnswers 8A Food, Glorious Food!David Alan McConnellNo ratings yet
- Compare and Contrast Process in Plants and AnimalsDocument8 pagesCompare and Contrast Process in Plants and AnimalsKimberly EamilaoNo ratings yet
- Learning To Perform Microvascular AnastomosisDocument12 pagesLearning To Perform Microvascular AnastomosisArtiomPaduretNo ratings yet
- CABG (Coronary Artery Bypass Graft)Document2 pagesCABG (Coronary Artery Bypass Graft)ebiiNo ratings yet
- 4th Semi FinalDocument16 pages4th Semi FinalDaypuyart Condez BernardNo ratings yet
- Coke and Great Depression - The Big LieDocument13 pagesCoke and Great Depression - The Big LieN yatesNo ratings yet
- Transport in Animals Revision NotesDocument11 pagesTransport in Animals Revision Notesamr ahmedNo ratings yet
- Heart Dissection PDFDocument2 pagesHeart Dissection PDFharryNo ratings yet
- A&P Exam 2 QuestionsDocument22 pagesA&P Exam 2 QuestionsAbdul QuorishyNo ratings yet
- Prepared By: Group 7Document41 pagesPrepared By: Group 7Ehm Zhy NhelNo ratings yet
- اسؤله اساسيات اولى معهدDocument7 pagesاسؤله اساسيات اولى معهدSalman MohamedNo ratings yet
- Chapter 08 - Transport in HumansDocument84 pagesChapter 08 - Transport in Humanshussaini polackNo ratings yet
- Human Biological Science 2 BIOL122: National Workshop Manual 2019Document78 pagesHuman Biological Science 2 BIOL122: National Workshop Manual 2019Huge Lovely SmileNo ratings yet
- Chapter 10Document29 pagesChapter 10MaskManNo ratings yet
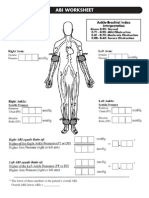
- Abi SheetsDocument2 pagesAbi Sheetszaky soewandi0% (1)
- Health & HygieneDocument5 pagesHealth & Hygieneegy1971100% (2)
- Biology Nce Grade 9 SpecimenDocument24 pagesBiology Nce Grade 9 SpecimenDaishaadil DilNo ratings yet