You might also like
- The Crash CartDocument39 pagesThe Crash Cartpramod kumawat100% (1)
- Nfpa Codes PDFDocument12 pagesNfpa Codes PDFphe zenNo ratings yet
- VALS System: Presented By: Atul Agarwal Balu K Thomas Dhiraj BhabhulgaonkarDocument18 pagesVALS System: Presented By: Atul Agarwal Balu K Thomas Dhiraj BhabhulgaonkarBalu K Thomas100% (1)
- ASCIA Guidelines Acute Management Anaphylaxis 2019Document8 pagesASCIA Guidelines Acute Management Anaphylaxis 2019Asadulla KhanNo ratings yet
- Drug StudyDocument7 pagesDrug StudyJoy Jarin100% (1)
- ER Intubation GuideDocument79 pagesER Intubation Guidezulham effendyNo ratings yet
- Allison - Dp-8000 - Manual de Servicio - Pag-390Document390 pagesAllison - Dp-8000 - Manual de Servicio - Pag-390Manuales De Maquinaria Jersoncat100% (1)
- NCM 118B Emergency MedicationsDocument110 pagesNCM 118B Emergency MedicationsJan Crizza Dale R. FrancoNo ratings yet
- ASCIA Guidelines Acute Management Anaphylaxis 2017 Updated PDFDocument8 pagesASCIA Guidelines Acute Management Anaphylaxis 2017 Updated PDFAyu WahyuniNo ratings yet
- Crash Cart Drugs: A Review of Medications Used in Cardiac ArrestDocument23 pagesCrash Cart Drugs: A Review of Medications Used in Cardiac ArrestKristiina MakinenNo ratings yet
- Nitric Acid - Nitrous Acid - Nitrogen Oxides - Ullman's EncyclopediaDocument49 pagesNitric Acid - Nitrous Acid - Nitrogen Oxides - Ullman's Encyclopediapoly6icsNo ratings yet
- AnaphylaxisDocument39 pagesAnaphylaxisLydia Novalista100% (1)
- EpinephrineDocument3 pagesEpinephrinealexjerimiahNo ratings yet
- Highh Mast LightingDocument6 pagesHighh Mast LightingAsghar KhanNo ratings yet
- InvoiceDocument2 pagesInvoiceamalNo ratings yet
- 1978 Damage - To Rock Tunnels From Earthquake ShakingDocument18 pages1978 Damage - To Rock Tunnels From Earthquake Shakingofelix505100% (1)
- High Alert MedicationsDocument17 pagesHigh Alert MedicationsJoanna Marie Datahan EstomoNo ratings yet
- Epinephrine Drug StudyDocument2 pagesEpinephrine Drug StudyAbigail De Leon80% (5)
- Anaphylactic Shock LectureDocument32 pagesAnaphylactic Shock LectureIchal 'petta' Malebbi100% (1)
- ASCIA Acute Management of Anaphylaxis Guidelines 2015Document4 pagesASCIA Acute Management of Anaphylaxis Guidelines 2015tom8989No ratings yet
- Lupus Eritematosus Sistemik Poliarteritis Nodosa Polimialgia Reumatik Reaksi Anafilaktik Demam Reumatik Artritis ReumatoidDocument43 pagesLupus Eritematosus Sistemik Poliarteritis Nodosa Polimialgia Reumatik Reaksi Anafilaktik Demam Reumatik Artritis ReumatoidKasdianto BantunNo ratings yet
- Anaphylaxis Wallchart 2018Document1 pageAnaphylaxis Wallchart 2018simranNo ratings yet
- AnaphylaxisDocument22 pagesAnaphylaxischitra gayenNo ratings yet
- Paediatric Clinical GuidelinesDocument7 pagesPaediatric Clinical GuidelinesAndriNo ratings yet
- EMERGENCY TREATMENT OF ANAPHYLACTIC REACTIONSDocument40 pagesEMERGENCY TREATMENT OF ANAPHYLACTIC REACTIONS'ranu HerjunaNo ratings yet
- Management of Anaphylactic Shock: DR Veerendra K H Asst Prof, Dept of MedicineDocument31 pagesManagement of Anaphylactic Shock: DR Veerendra K H Asst Prof, Dept of MedicineveerendrakhNo ratings yet
- Supportive Care Essentials in Clinical ToxicologyDocument4 pagesSupportive Care Essentials in Clinical ToxicologyFeroze FathimaNo ratings yet
- ASCIA Guidelines Acute Management Anaphylaxis Dec2016Document5 pagesASCIA Guidelines Acute Management Anaphylaxis Dec2016kkkssbbNo ratings yet
- 12.0 Emergency Protocol Allergic ReactionsDocument9 pages12.0 Emergency Protocol Allergic ReactionsConstantin BudinNo ratings yet
- VF PediDocument6 pagesVF PedixiphoideusNo ratings yet
- Treating Dental EmergenciesDocument15 pagesTreating Dental Emergenciesminaxi123No ratings yet
- Anaphylaxis Acute Management ABCDEDocument8 pagesAnaphylaxis Acute Management ABCDESSNo ratings yet
- CNEP Guide to Code Blue ResponseDocument93 pagesCNEP Guide to Code Blue ResponsedindaNo ratings yet
- Management of Medical Emergencies GuideDocument2 pagesManagement of Medical Emergencies Guidekojeda1No ratings yet
- Emergency GuidelinesDocument11 pagesEmergency GuidelineswinstonappsNo ratings yet
- Anaphylaxis: By: O. Ahmadi, MD. Professor Assistant of Esfahan Medical School, Emergency Department of Al-Zahra HospitalDocument39 pagesAnaphylaxis: By: O. Ahmadi, MD. Professor Assistant of Esfahan Medical School, Emergency Department of Al-Zahra HospitalBudi SetyanugrahaNo ratings yet
- Syok Anafilaksis 1Document4 pagesSyok Anafilaksis 1Mariatun Zahro NasutionNo ratings yet
- Anaesthetic EmergenciesDocument11 pagesAnaesthetic EmergenciesSivasankaryNo ratings yet
- Anaphylaxis: How To Recognize, Treat, and Prevent Potentially Fatal AttacksDocument8 pagesAnaphylaxis: How To Recognize, Treat, and Prevent Potentially Fatal AttacksИван Марковић ИскеNo ratings yet
- Pediatric Protokol EmergencyDocument19 pagesPediatric Protokol EmergencyChristian RobbyNo ratings yet
- A (ACLS) - 2015: Dvanced Cardiac Life SupportDocument52 pagesA (ACLS) - 2015: Dvanced Cardiac Life SupportNajmussaqibNo ratings yet
- Current Clinical Strategies: Handbook of AnesthesiologyDocument180 pagesCurrent Clinical Strategies: Handbook of AnesthesiologydramaganaNo ratings yet
- ANAPHYLAXISDocument21 pagesANAPHYLAXISMicah TuringanNo ratings yet
- Penatalaksanaan Reaksi AnafilaktikDocument4 pagesPenatalaksanaan Reaksi AnafilaktikAnnisa RusfianaNo ratings yet
- Hersheychapter 1Document17 pagesHersheychapter 1poddata100% (1)
- Presenter - Dr. Ashray - VDocument33 pagesPresenter - Dr. Ashray - VKhushbu JainNo ratings yet
- Acute Management of Anaphylaxis: Adrenaline (Epinephrine) Is The First Line Treatment For AnaphylaxisDocument8 pagesAcute Management of Anaphylaxis: Adrenaline (Epinephrine) Is The First Line Treatment For AnaphylaxissigmapomalNo ratings yet
- Drugs AjDocument19 pagesDrugs AjPugazhenthi CNo ratings yet
- ASCIA HP Guidelines Acute Management Anaphylaxis 2020Document8 pagesASCIA HP Guidelines Acute Management Anaphylaxis 2020Munshi KamrulNo ratings yet
- Anaphylaxis: Initial Management in Non-Hospital Settings: Edition", Pages 14 To 18 (Anaphylaxis Section Only)Document4 pagesAnaphylaxis: Initial Management in Non-Hospital Settings: Edition", Pages 14 To 18 (Anaphylaxis Section Only)Fera MulidarNo ratings yet
- Protocol For Treatment of Anaphylactic ReactionsDocument1 pageProtocol For Treatment of Anaphylactic ReactionsbuenaNo ratings yet
- Refractory Anaphylaxis, Treatment Algorithm.2021Document3 pagesRefractory Anaphylaxis, Treatment Algorithm.2021Patricia AndradeNo ratings yet
- AtropinDocument9 pagesAtropinarfitaaaaNo ratings yet
- Azithromycin 500mg Tab (Zithromax)Document6 pagesAzithromycin 500mg Tab (Zithromax)Mayownski TejeroNo ratings yet
- Snakebite Management Guide For Healthcare Providers in Malaysia 2011Document8 pagesSnakebite Management Guide For Healthcare Providers in Malaysia 2011fifa_0304535100% (1)
- PocketCard Contrast ReactionsDocument2 pagesPocketCard Contrast ReactionsThomasNo ratings yet
- Final Assignment of ShockDocument21 pagesFinal Assignment of Shocknyandap tanyuNo ratings yet
- Pediatric Medical Emergencies Rev Oct 2016Document27 pagesPediatric Medical Emergencies Rev Oct 2016ElvisNo ratings yet
- Anaphylaxis - Emergency Treatment - UpToDateDocument49 pagesAnaphylaxis - Emergency Treatment - UpToDatealinaNo ratings yet
- Clinical Management JEDocument15 pagesClinical Management JEegalivanNo ratings yet
- Neonatal Seizures: Learning ObjectivesDocument6 pagesNeonatal Seizures: Learning ObjectivesSatya Prakash TiwariNo ratings yet
- Emergency Pediatric AidsDocument29 pagesEmergency Pediatric AidsRana SalemNo ratings yet
- Seven Ps For RSI BOARDDocument2 pagesSeven Ps For RSI BOARDJames BrownNo ratings yet
- PICU Anaesthetic Drugs GuideDocument6 pagesPICU Anaesthetic Drugs GuideAmar Mahesh KalluNo ratings yet
- Early Childhood Teachers Psychological Well Being Exploring Potential Predictors of Depression Stress and Emotional ExhaustionDocument18 pagesEarly Childhood Teachers Psychological Well Being Exploring Potential Predictors of Depression Stress and Emotional ExhaustionAhmed QlhamdNo ratings yet
- School- Utilization- Urban Children-Mental Health ProblemsقديمDocument18 pagesSchool- Utilization- Urban Children-Mental Health ProblemsقديمAhmed QlhamdNo ratings yet
- Teacher Autonomy Support Reduces Adolescent Anxiety and DepressionDocument9 pagesTeacher Autonomy Support Reduces Adolescent Anxiety and DepressionAhmed QlhamdNo ratings yet
- Endocrine Midterm 21: Anatomy & EmbryologyDocument1 pageEndocrine Midterm 21: Anatomy & EmbryologyAhmed QlhamdNo ratings yet
- Plaintiff's Original Petition: Uber Ridesharing DefendantDocument8 pagesPlaintiff's Original Petition: Uber Ridesharing DefendantWigingtonRumleyDunnBlairLLPNo ratings yet
- Cloze Test For The Upcoming SSC ExamsDocument9 pagesCloze Test For The Upcoming SSC ExamsAbhisek MishraNo ratings yet
- Power Solutions GuideDocument60 pagesPower Solutions Guidetheodoiq100% (1)
- Department of Civil Engineering, Semester 7th: Different Types of BridgesDocument39 pagesDepartment of Civil Engineering, Semester 7th: Different Types of BridgesSiddhartha SahaNo ratings yet
- Services Marketing Chapter-9Document15 pagesServices Marketing Chapter-9Orko AhmedNo ratings yet
- Example of An Essay CAEDocument3 pagesExample of An Essay CAEJon ArriaranNo ratings yet
- Join in SQLDocument9 pagesJoin in SQLSugeenaNo ratings yet
- Annul. Press. Bleed Off Proced.Document3 pagesAnnul. Press. Bleed Off Proced.eng7mohamed7hashimNo ratings yet
- Magnetic Particle TestDocument4 pagesMagnetic Particle TestHarry Doble100% (1)
- AI Story WritermnfyaDocument2 pagesAI Story Writermnfyafrenchrugby98No ratings yet
- Quiz II - Company MissionDocument4 pagesQuiz II - Company MissionSuraj SapkotaNo ratings yet
- Petron Corporate PresentationDocument46 pagesPetron Corporate Presentationsivuonline0% (1)
- Aoc ts185 LCD MonitorDocument56 pagesAoc ts185 LCD MonitoraldinaenNo ratings yet
- 10 Days 7 NightsDocument5 pages10 Days 7 NightsSisca SetiawatyNo ratings yet
- Empowerment Technologies Week 1-2 - Final Term: Prepared By: Mr. Jake Indico Edited By: Ms. Shaira G. RaquilDocument5 pagesEmpowerment Technologies Week 1-2 - Final Term: Prepared By: Mr. Jake Indico Edited By: Ms. Shaira G. RaquilJustine Evasco RubiaNo ratings yet
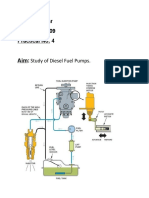
- Study of Diesel Fuel Pumps ComponentsDocument6 pagesStudy of Diesel Fuel Pumps ComponentsPro GamerssNo ratings yet
- Akd 736103113213Document1 pageAkd 736103113213May'Axel RomaricNo ratings yet
- Assignment 2 QP MPMC - ITDocument1 pageAssignment 2 QP MPMC - ITProjectsNo ratings yet
- Haslinda Mohd Anuar Senior Lecturer School of Law ColgisDocument24 pagesHaslinda Mohd Anuar Senior Lecturer School of Law ColgisSHAHEERANo ratings yet
- Fundamentals of Metal Matrix CompositesDocument19 pagesFundamentals of Metal Matrix CompositesAstriaNo ratings yet
- SA-10/20 User ManualDocument31 pagesSA-10/20 User ManualJorgeLuis Anaya NúñezNo ratings yet
- Remote Environment: - Concern The Nature and Direction of Economy in Which A Firm Operates - Types of FactorsDocument27 pagesRemote Environment: - Concern The Nature and Direction of Economy in Which A Firm Operates - Types of FactorsmikiyingNo ratings yet
- Group 3 - Brand Architecture Assignment IDocument9 pagesGroup 3 - Brand Architecture Assignment IShijin SreekumarNo ratings yet