You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Sean Griffin - Tinker Belles and Evil QueensDocument317 pagesSean Griffin - Tinker Belles and Evil QueensLizzy Chin100% (2)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The New Faces of ChristianityDocument265 pagesThe New Faces of ChristianityValéria100% (5)
- Weitzman Research ProposalDocument8 pagesWeitzman Research ProposalAlex WeitzmanNo ratings yet
- (WARNER, Michael) Fear of A Queer Planet - IntroductionDocument16 pages(WARNER, Michael) Fear of A Queer Planet - IntroductionMolly MillionsNo ratings yet
- NIH Public Access: Author ManuscriptDocument20 pagesNIH Public Access: Author ManuscriptSarif CassanovaNo ratings yet
- BouhnikDocument9 pagesBouhnikSarif CassanovaNo ratings yet
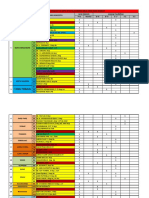
- Rekap Anggota DPD Ipai Sulawesi Selatan Dan Barat: Tana TorajaDocument3 pagesRekap Anggota DPD Ipai Sulawesi Selatan Dan Barat: Tana TorajaSarif CassanovaNo ratings yet
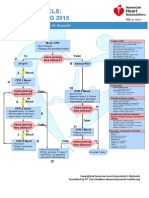
- Algoritma ACLS Bhs IndonesiaDocument6 pagesAlgoritma ACLS Bhs IndonesiaSarif CassanovaNo ratings yet
- Management of Foreskin ConditionsDocument26 pagesManagement of Foreskin ConditionsSarif CassanovaNo ratings yet
- Test Bank For Psychology in Modules Eleventh Edition DownloadDocument28 pagesTest Bank For Psychology in Modules Eleventh Edition Downloadkennethmataqfsdwnxcot100% (25)
- Divorce StatisticsDocument15 pagesDivorce StatisticsEq BrownNo ratings yet
- Social Science Research PaperDocument3 pagesSocial Science Research PaperJe RelloraNo ratings yet
- Celluloid Comrades - Representations of Male Homosexuality in Contemporary Chinese CinemasDocument269 pagesCelluloid Comrades - Representations of Male Homosexuality in Contemporary Chinese CinemasElena Kuzmina100% (3)
- 5 12 16Document32 pages5 12 16ConnorNo ratings yet
- Module 14 and 15Document6 pagesModule 14 and 15Rica Mae BotorNo ratings yet
- Making Excellence Inclusive:: Higher Education's LGBTQ ContextsDocument24 pagesMaking Excellence Inclusive:: Higher Education's LGBTQ ContextsinquepennNo ratings yet
- The Treatment of Homosexuality - Some Historical Contemporary An SCOTT RICHARDS PDFDocument18 pagesThe Treatment of Homosexuality - Some Historical Contemporary An SCOTT RICHARDS PDFAcetiNo ratings yet
- The Politics of Identity: AppiahDocument9 pagesThe Politics of Identity: AppiahjgswanNo ratings yet
- UTSDocument2 pagesUTSMikaela LozanoNo ratings yet
- Gender and Society Prelim ExamDocument5 pagesGender and Society Prelim ExamLes Jara LJNo ratings yet
- Sexual Orientation Scale 2020Document10 pagesSexual Orientation Scale 2020MaqboolNo ratings yet
- Kelompok 8 - Chapter 9 (Gender)Document15 pagesKelompok 8 - Chapter 9 (Gender)pinkan.rafa23No ratings yet
- (Histories and Addresses of Philosophical Societies) Raja Halwani, Carol V. A. Quinn, Andy Wible - Queer Philosophy_ Presentations of the Society for Lesbian and Gay Philosophy, 1998-2008-Rodopi (2012.pdfDocument414 pages(Histories and Addresses of Philosophical Societies) Raja Halwani, Carol V. A. Quinn, Andy Wible - Queer Philosophy_ Presentations of the Society for Lesbian and Gay Philosophy, 1998-2008-Rodopi (2012.pdfJoseph RuedaNo ratings yet
- Persuasive Speech Preparation OutlineDocument5 pagesPersuasive Speech Preparation OutlineVũ TâmNo ratings yet
- Unit 3 Masculinities: StructureDocument10 pagesUnit 3 Masculinities: StructureHarry AryanNo ratings yet
- Out of The ShadowsDocument90 pagesOut of The ShadowsCenter for American ProgressNo ratings yet
- BRIEF: The Kinsey Institute ExposedDocument29 pagesBRIEF: The Kinsey Institute ExposedJudith Reisman, Ph.D.100% (1)
- PRELIM Learning KitDocument6 pagesPRELIM Learning KitRegina Joy JabonNo ratings yet
- Homosexuality vs. HeterosexualityDocument3 pagesHomosexuality vs. Heterosexualityteganemmalia4643100% (1)
- The Top Ten Harms of Same-Sex "Marriage": Immediate EffectsDocument13 pagesThe Top Ten Harms of Same-Sex "Marriage": Immediate EffectsyohoyonNo ratings yet
- Interview Dale O'LearyDocument3 pagesInterview Dale O'LearyAnonymous 1XIYOVXv6100% (2)
- Types of Family, Health EducationDocument17 pagesTypes of Family, Health EducationNessa Layos MorilloNo ratings yet
- Right To Privacy and Sec. 377Document17 pagesRight To Privacy and Sec. 377Saif100% (1)
- William L. Petersen, "Can ApΣenokoitai Be Translated by ‘Homosexuals'? (I Cor. 6.9; I Tim. 1.10) ."Document6 pagesWilliam L. Petersen, "Can ApΣenokoitai Be Translated by ‘Homosexuals'? (I Cor. 6.9; I Tim. 1.10) ."JonathanNo ratings yet
- Lesbians, Gays, Bisexuals and TransgenderDocument9 pagesLesbians, Gays, Bisexuals and Transgenderlance steven huescaNo ratings yet