You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5796)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Appendix I JD Service Manual PDFDocument661 pagesAppendix I JD Service Manual PDFJoao Silva0% (1)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Taylor's Handbook of Clinical Nursing SkillsDocument87 pagesTaylor's Handbook of Clinical Nursing SkillsSupremo Manuel M DeluaoNo ratings yet
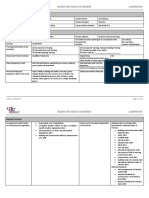
- Safe Work Method Statement: Gypsum Partition/ Column Framing, Cladding& Paneling/Pop PunningDocument6 pagesSafe Work Method Statement: Gypsum Partition/ Column Framing, Cladding& Paneling/Pop PunningSiddharth PNo ratings yet
- Inspection Instruction EN PDFDocument147 pagesInspection Instruction EN PDFMuhammed Shamseer50% (2)
- Job Hazard Analysis Welding Operations: Job Title: Work Place LocationDocument18 pagesJob Hazard Analysis Welding Operations: Job Title: Work Place Locationmuhammad imtiaz100% (1)
- CPCSEA Guidelines PDFDocument121 pagesCPCSEA Guidelines PDFNeha Roy100% (2)
- The World of Disposable Gloves: Compact GuideDocument16 pagesThe World of Disposable Gloves: Compact GuideOliver Patrick StrösserNo ratings yet
- Boustednavalshipyard Safety AssessmentDocument41 pagesBoustednavalshipyard Safety Assessmentikhmal ismayatimNo ratings yet
- MOS-LV Cable Installation, Testing, Splicing & TerminationDocument9 pagesMOS-LV Cable Installation, Testing, Splicing & Termination01095902062ahmedNo ratings yet
- САТ 574 мануал оператора англ PDFDocument208 pagesСАТ 574 мануал оператора англ PDFPavelNo ratings yet
- SikaProof A Method StatementDocument41 pagesSikaProof A Method StatementNUR AIN ROSDINo ratings yet
- 10 1016@j Ajem 2020 10 021Document10 pages10 1016@j Ajem 2020 10 021RianNo ratings yet
- Latsios 2020Document5 pagesLatsios 2020RianNo ratings yet
- Deep Breathing Exercise Education Receiving and Performing Status of Patients Undergoing Abdominal SurgeryDocument4 pagesDeep Breathing Exercise Education Receiving and Performing Status of Patients Undergoing Abdominal SurgeryRianNo ratings yet
- 308 Nadolny OrgDocument30 pages308 Nadolny OrgRianNo ratings yet
- Infection Control & Hospital EpidemiologyDocument9 pagesInfection Control & Hospital EpidemiologyRianNo ratings yet
- CCJM 87a ccc040 FullDocument3 pagesCCJM 87a ccc040 FullRianNo ratings yet
- Jurnal 1Document5 pagesJurnal 1RianNo ratings yet
- 2021 Article 63Document7 pages2021 Article 63RianNo ratings yet
- AnnalsATS 202007-803OCDocument9 pagesAnnalsATS 202007-803OCRianNo ratings yet
- 416 FullDocument6 pages416 FullRianNo ratings yet
- Content ServerDocument18 pagesContent ServerRianNo ratings yet
- Content ServerDocument14 pagesContent ServerRianNo ratings yet
- V2I4 - Sabina Dumitrescu - RJCBTHDocument7 pagesV2I4 - Sabina Dumitrescu - RJCBTHRianNo ratings yet
- Adolescents ' Definitions of Bullying: The Contribution of Age, Gender, and Experience of BullyingDocument17 pagesAdolescents ' Definitions of Bullying: The Contribution of Age, Gender, and Experience of BullyingRianNo ratings yet
- IJESE 2109 Article 5ce3cae248105Document12 pagesIJESE 2109 Article 5ce3cae248105RianNo ratings yet
- Bullying, Depression, and Suicidal Ideation Among Adolescents in The Fujian Province of ChinaDocument6 pagesBullying, Depression, and Suicidal Ideation Among Adolescents in The Fujian Province of ChinaRianNo ratings yet
- Bullying: Remaja SMA Di Kota YogyakartaDocument6 pagesBullying: Remaja SMA Di Kota YogyakartaRianNo ratings yet
- Fullpapers Jphrchda3d2ca5d9afullDocument7 pagesFullpapers Jphrchda3d2ca5d9afullRianNo ratings yet
- Park 2020Document9 pagesPark 2020RianNo ratings yet
- SDS Caustic Soda SolutionDocument24 pagesSDS Caustic Soda SolutionDinu KhanNo ratings yet
- Puranmal Lahoti Government Polytechnic LaturDocument11 pagesPuranmal Lahoti Government Polytechnic Laturshankar biradarNo ratings yet
- HSE DocsDocument30 pagesHSE DocsAbubakr MohamedNo ratings yet
- New GLOVE Standards & RequirementsDocument6 pagesNew GLOVE Standards & RequirementsΚαίτη ΔιαμαντήNo ratings yet
- Safety Data Sheet: Texclad 2Document7 pagesSafety Data Sheet: Texclad 2KuhnNo ratings yet
- BMP 71 Nimh Batteries SdsDocument11 pagesBMP 71 Nimh Batteries SdsPradeep KrishnanNo ratings yet
- Penetration Grade BitumenDocument5 pagesPenetration Grade BitumenAzwanAliNo ratings yet
- 480-EIA Manual of Recommended Safety Practices - IndexDocument4 pages480-EIA Manual of Recommended Safety Practices - Indexkirandevi1981No ratings yet
- Work Method Statement Carpentry: Organisation DetailsDocument22 pagesWork Method Statement Carpentry: Organisation DetailsCathy SmithNo ratings yet
- Supervisor H&S AwarenessDocument31 pagesSupervisor H&S AwarenessAyat TaNo ratings yet
- Castillo ProfileDocument46 pagesCastillo ProfileprabhumanocNo ratings yet
- By: Cleveland Construction: Glasses, Safety Vest, Proper Clothing Depend On Your Work PlaceDocument3 pagesBy: Cleveland Construction: Glasses, Safety Vest, Proper Clothing Depend On Your Work PlaceDaniel ManivoughNo ratings yet
- BBC PaintDocument9 pagesBBC PaintVinith KumarNo ratings yet
- CatalogDocument46 pagesCataloglangtu2011No ratings yet
- XR1245 Manual de Operador PDFDocument82 pagesXR1245 Manual de Operador PDFfercho_50No ratings yet
- MSDS Bagazo de CañaDocument5 pagesMSDS Bagazo de CañaYovany Padilla100% (2)
- EX1900-6 Workshop ManualDocument552 pagesEX1900-6 Workshop ManualShaun GibsonNo ratings yet
- Solvente Mutual ChevronDocument12 pagesSolvente Mutual Chevronjcamacho95No ratings yet
- Genesis Rescue 2016 Spreaders User GuideDocument47 pagesGenesis Rescue 2016 Spreaders User GuideForum PompieriiNo ratings yet