Professional Documents
Culture Documents
Review: The International Hypoglycaemia Study Group
Uploaded by
ChindyOriginal Title
Copyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
Review: The International Hypoglycaemia Study Group
Uploaded by
ChindyCopyright:
Available Formats
Review
Hypoglycaemia, cardiovascular disease, and mortality in
diabetes: epidemiology, pathogenesis, and management
The International Hypoglycaemia Study Group*
Hypoglycaemia has long been recognised as a dangerous side-effect of treatment of diabetes with insulin or insulin Lancet Diabetes Endocrinol 2019
secretagogues. With its potential to disrupt cerebral function, hypoglycaemia can have a major effect on peoples’ lives. Published Online
Study findings have suggested that hypoglycaemia is associated with an increased risk of cardiovascular events and March 26, 2019
http://dx.doi.org/10.1016/
mortality. Different mechanisms by which hypoglycaemia might provoke cardiovascular events have been identified
S2213-8587(18)30315-2
in experimental studies, and in clinical studies cardiac arrhythmias have been reported to be induced by hypoglycaemia,
*Members listed at end of
with one report describing sudden death during a severe episode. Emerging evidence suggests that the association Review
between hypoglycaemia and cardiovascular events and mortality is likely to be multifactorial. The association is Correspondence to:
probably partly caused by confounding, with hypoglycaemia occurring more frequently in people with comorbidities Prof Simon R Heller, Academic
who are also more likely to die than those without. However, people with type 1 or type 2 diabetes also seem at risk of Unit of Diabetes, Endocrinology
hypoglycaemia-induced cardiovascular effects. This risk should be recognised by clinicians when agreeing glycaemic and Metabolism, Department of
Oncology & Metabolism,
goals with patients and choosing appropriate glucose-lowering therapies. University of Sheffield, Sheffield
S10 2RX, UK
Introduction s.heller@sheffield.ac.uk
Hypoglycaemia in people with diabetes has been defined UK from 1979, hypoglycaemia was reported to cause 4%
by an American Diabetes Association (ADA) working of deaths of all people with diabetes younger than
group as all episodes of an abnormally low plasma glucose 50 years.4 This report might have underestimated the
concentration that expose the individual to potential number of deaths from hypoglycaemia, because deaths
harm.1 It is associated with several negative life from myocardial infarction and other causes that could
consequences, ranging from disruption of daily activities have resulted from hypoglycaemia-induced cardiac
to psychosocial problems for both patients and their arrhythmias were included as separate categories. More
family members. Moreover, the possibility that recent studies have recorded a higher prevalence of
hypoglycaemia might directly increase mortality has been deaths directly due to hypoglycaemia, with more than 8%
recognised since the discovery of insulin. Fatal brain reported in people with type 1 diabetes younger than
injury from profound neuroglycopenia is quite rare, but 56 years in a Norwegian study.5 Although this finding
following the early termination of the Action to Control might reflect greater precision in identifying the cause of
Cardiovascular Risk in Diabetes (ACCORD) trial because death, an alternative explanation is that it represents an
of increased mortality in participants treated intensively,2 increased frequency of hypoglycaemia and associated
there has been a major interest in the association between mortality.
hypoglycaemia and fatal cardiovascular events.
The increased mortality in the ACCORD trial provoked Epidemiology
considerable controversy with respect to its underlying The results of the UK Prospective Diabetes Study
cause. Negative cardiovascular consequences of hypo (UKPDS), published in 1998, confirmed that intensive
glycaemia might explain why intensive glycaemic control glycaemic control could reduce microvascular disease in
has generally not lowered the risk of cardiovascular events patients with newly diagnosed type 2 diabetes. It also
in clinical trials. Alternatively, the association might be resulted in an observational analysis suggesting that a
explained by confounding, with hypoglycaemic episodes more intensive approach had the potential to prevent
identifying vulnerable individuals with comorbidities that macrovascular events.6 Indeed, extended follow-up for the
render them prone to adverse outcomes and who are 10 years after the trial ended showed significant reductions
therefore more likely to have experienced hypoglycaemia in rates of myocardial infarction and cardiovascular
during treatment. In this Review, we explore the mortality.7 Three randomised clinical trials subsequently
epidemiology of hypoglycaemia and cardiovascular tested the hypothesis, comparing the effect of more
disease, identify potential mechanisms, explain the versus less intensive glycaemic control among individuals
competing hypotheses, consider what additional research with established type 2 diabetes at increased cardiovascular
is required, and suggest how the issue might be risk, but all three trials did not show significant reductions
approached in clinical practice. in cardiovascular events or mortality.2,8,9 In fact, mortality
in one of these trials, ACCORD, actually increased.2
Hypoglycaemia and mortality Although there are other potential causes of increased
That hypoglycaemia could be fatal was recognised soon mortality such as weight gain, use of certain medications,
after the discovery of insulin during animal experiments, or even chance alone, it is noteworthy that compared with
and early clinical use soon led to reports of deaths in the ADVANCE (Action in Diabetes and Vascular Disease:
people with diabetes.3 In an epidemiological study in the Preterax and Diamicron MR Controlled Evaluation) trial,9
www.thelancet.com/diabetes-endocrinology Published online March 26, 2019 http://dx.doi.org/10.1016/S2213-8587(18)30315-2 1
Review
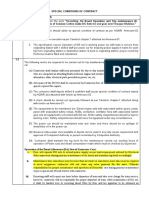
Severe No severe Hazard ratio compared with those who did not. This increased risk
hypoglycaemia hypoglycaemia (95% CI) seems to be shared by people with type 1 and type 2
(n=231) (n=10 909)
diabetes,23 although the magnitude of the risks varies with
Major macrovascular events 33 (11·5%) 1114 (10·2%) 3·53 (2·41–5·17) diabetes type, background cardiovascular risk, presence of
Major microvascular events 24 (10.4%) 1107 (10·1%) 2·19 (1·40–3·45) comorbidities, severity of hypoglycaemia, temporality of
Death from any cause 45 (19·5%) 986 (9·0%) 3·27 (2·29–4·65) hypoglycaemia to the event, length of follow-up, and level
Cardiovascular disease 22 (9·5%) 520 (4·8%) 3·79 (2·36–6·08)
of adjustment for potential confounders. The association
Non-cardiovascular disease 23 (10·0%) 466 (4·3%) 2·80 (1·64–4·79)
is not confined to hypoglycaemia induced by insulin—a
0·1 1·0 10·0 similar association has been reported for hypoglycaemia
induced by sulfonylureas.30 Additional post-hoc analyses
Figure 1: Association of severe hypoglycaemia with the risk of an adverse clinical outcome or death in other trials with cardiovascular outcomes have also
The hazard ratio represents the risk of an adverse clinical outcome or death among patients reporting severe
hypoglycaemia compared with those not reporting severe hypoglycaemia. The centres of the squares are placed at
raised the likely contribution of confounding as an
the point estimates and the horizontal lines represent the corresponding 95% CIs. The area of each square is explanation for the association.11,12
proportional to the inverse of the variance of each estimate. Reproduced from Zoungas et al,10 by permission of the The observational nature of many of the analyses and
Massachusetts Medical Society. the inability to capture all hypoglycaemic episodes
(particularly milder or asymptomatic episodes that might
which showed no increase in mortality, the frequency of contribute to cardiovascular events), have made it
severe hypoglycaemia in ACCORD was four to five times difficult to confirm or refute causality, particularly in
higher. The Veteran’s Affairs Diabetes Trial (VADT), relation to cardiovascular events. Nevertheless, results
which was done over the same period, was underpowered from some studies have shown an association between
to measure the effect of hypoglycaemia on mortality.8 cardiovascular events (particularly myocardial infarction)
However, all three studies showed a significant association and hypoglycaemia;24 the evidence seems less consistent
between severe hypoglycaemia and mortality. In VADT for the association between hypoglycaemia and stroke.31
and ADVANCE, severe hypoglycaemia predicted later Therefore, this Review mainly focuses on studies that
mortality (ie, downstream of the hypoglycaemic episode); report links between mortality and severe hypoglycaemia.
in ADVANCE, the median time from severe In most studies, severe hypoglycaemia is defined as
hypoglycaemia to death was 1·05 years. The difference in episodes that require the assistance of another person to
diabetes duration between these later studies and UKPDS recover. However, where reliable studies reporting
might be relevant to their different outcomes since the cardiovascular events were available, these were included.
UKPDS studied those newly diagnosed, whereas the The debate might also be framed by asking whether
three more recent trials recruited patients with established hypoglycaemia should be considered a risk factor for
diabetes, many of whom were at increased cardiovascular cardiovascular disease or merely a risk marker. Chronic
risk. hyperglycaemia leads to increased rates of cardiovascular
Whether the association in these later trials is causal or disease and is considered a risk factor. If intensive
because of confounding remains uncertain. It has been management increases the rate of severe hypoglycaemic
argued that confounding might explain the association episodes in people because they are frail with
between hypoglycaemia and mortality—ie, that comorbidities, they are more likely to die; therefore,
comorbidities (such as renal or liver disease, malignancy, hypoglycaemia would be considered a risk marker of
weight loss, or cognitive impairment) confer an increased mortality. Alternatively, if hypoglycaemia, particularly
risk of hypoglycaemia and of cardiovascular events and repeated episodes and not necessarily severe, activate
mortality. Zoungas and colleagues10 attributed at least physiological responses that accelerate cardiovascular
some of the association between mortality and severe disease, hypoglycaemia could be a regarded as a risk
hypoglycaemia in ADVANCE to confounding (figure 1). factor.
This conclusion was based on the increased hazard ratio A definitive trial to prove causality in which severe
of non-cardiovascular events in participants who hypoglycaemia is deliberately induced in one group and
experienced severe hypoglycaemia compared with those not the other, and mortality compared in both, is clearly
who did not; it was reasoned that events associated with not possible for ethical and practical reasons. However,
respiratory or gastrointestinal diseases were most the conclusion that a causal association exists between
unlikely to have been caused by hypoglycaemia. hypoglycaemia and cardiovascular events is supported by
These concerns have resulted in additional cohort two systematic reviews, which used the statistical
studies (both clinical trial and epidemiological) in people technique of bias analysis in meta-analyses of large
with diabetes (table). Collectively, these studies have numbers of participants in observational studies.32,33 The
included tens of thousands of patients with type 1 or type 2 authors of these reviews concluded that comorbid severe
diabetes from different regions of the world and different illness alone could not explain the association, because
health-care settings. These studies have shown a roughly the prevalence of comorbidity would have had to be far
1·5–6-times increased risk of cardiovascular events and higher than it was to account for the association.
mortality among participants who had hypoglycaemia Furthermore, Yeh and colleagues33 reported a
2 www.thelancet.com/diabetes-endocrinology Published online March 26, 2019 http://dx.doi.org/10.1016/S2213-8587(18)30315-2
Review
Publication year Severity of Diabetes type Sample size Follow-up Effect size (adjusted; 95% CI)
hypoglycaemia
Clinical trial cohorts
DEVOTE 311 2018 Severe Type 2 7637 Median 2·0 years CVD HR 1·38 (0·96–1·96); all-cause death HR 2·51
(1·79–3·50)
EXAMINE12 2017 Severe Type 2 5380 Median 1·5 years CVD HR 2·42 (1·27–4·60); CVD post-severe hypoglycaemia
HR 1·60 (0·80–3·20)
ORIGIN13 2013 Severe Type 2 12 537 Median 6·2 years CVD HR 1·58 (1·24–2·02); CV death HR 1·71 (1·27–2·30);
all-cause death HR 1·74 (1·39–2·19); arrhythmic death
HR 1·77 (1·17–2·67)
ORIGIN13 2013 Non-severe Type 2 12 537 Median 6·2 years No association
VADT8 2011 Severe Type 2 1791 Median 5·6 years CVD HR 1·88 (1·03–3·43)
ADVANCE10 2010 Severe Type 2 11 140 Median 5·0 years CVD HR 3·53 (2·41–5·17); CV death HR 3·79 (2·36–6·08);
all-cause death HR 3·27 (2·29–4·65)
ACCORD 14 2010 Severe Type 2 10 194 Mean 3·5 years All-cause death HR (intensive glucose control group) 1·41
(1·03–1·93); all-cause death HR (standard glucose control
group) 2·30 (1·46–3·65)
Epidemiological cohorts
ARIC15 2018 Severe Type 2 1209 Median 15·3 years CHD HR 2·02 (1·27–3·20); CV death HR 1·64 (1·15–2·34);
all-cause death HR 1·73 (1·38–2·17)
Taiwan database16 2016 Severe Type 1 4361 5 years* CVD HR 2·74 (1·96–3·85)
Japanese database17 2016 Severe Type 2 58 223 Mean 2·3 years CVD HR 3·39 (1·25–9·18)
US Academic Primary Care 2016 Not defined Type 1 and 2 9173 Mean 5·2 years CHD HR 2·15 (1·24–3·74) without previous CAD; CHD
Network18 HR 3·01 (1·15–7·91) in patients at high vascular risk; CHD
HR 4·62 (1·65–12·9) in patients aged ≥65 years
Vincent Type 2 Diabetes 2016 Severe Type 2 906 Median 10·4 years All-cause death HR 2·64 (1·39–5·02); CV death HR 6·34
Registry (South Korea)19 (2·02–19·87)
Dutch and Danish cohorts20 2016 Severe Type 1 482 (Dutch); 6·5 years (Dutch); No association for all-cause death or CV death
269 (Danish) 12 years (Danish)
Joint Asia Diabetes Registry21 2016 Mild Type 2 18 589 Mean 3·9 years CVD HR 1·16 (0·94–1·43); all-cause death HR 1·03
(0·78–1·36)
CREDIT study22 2016 Severe Type 2, insulin 2999 4·0 years* CV death HR 1·10 (0·34–3·57); all-cause death HR 1·22
treated (0·59–2·53)
UK GP database23 2015 Severe Type 1 3260 Median 5·0 years CVD secondary care HR 1·10 (0·40–3·01); CVD HR 1·92
(1·31–2·79)
UK GP database23 2015 Severe Type 2, insulin 10 422 Median 4·8 years CVD secondary care HR 1·70 (1·09–2·64); CVD HR 1·50
treated (1·19–1·88)
Edinburgh Type 2 Diabetes 2014 Severe Type 2 1066 Mean 4·0 years CVD HR 1·60 (1·13–2·26)
Study24
Swedish Diabetes Register25 2014 Severe Type 1 1839 5 years* All-cause death HR 1·25 (1·02–1·53)
German primary are 2013 Severe Type 2 25 712 Mean 2·0 years CVD HR 2·11 (1·06–4·20)
database26
Taiwan database27 2013 Severe Type 2 2500 10 years* CVD HR 2·26 (1·93–2·65); CHD HR 1·63 (1·28–2·08);
stroke HR 1·64 (1·29–2·07)
Taiwan database27 2013 Mild Type 2 2500 10 years* CVD HR 2·21 (1·98–2·47)
US Veterans Network28 2012 Severe Type 2 1522 Median 3·9 years CVD HR 2·00 (1·63–2·44)
Medicare database29 2011 Severe Type 2 860 845 Mean 1 year CVD HR 1·79 (1·69–1·89)
CVD=cardiovascular disease. HR=hazard ratio. CV=cardiovascular. CHD=coronary heart disease. CAD=coronary artery disease. *Type of descriptive statistic not stated.
Table: Studies linking hypoglycaemia to cardiovascular events and mortality
dose-response relation (ie, severe hypoglycaemia showed A study from 2018 lends support to the hypothesis that
a stronger association than less severe episodes). hypoglycaemia might oppose the benefits of strict
The authors also highlighted the many plausible glycaemic control, and that hypoglycaemia is indeed a
pathophysiological mechanisms that might contribute to risk factor for cardiovascular disease and mortality.34 The
increased cardiovascular events. researchers used meta-regression analysis to investigate
www.thelancet.com/diabetes-endocrinology Published online March 26, 2019 http://dx.doi.org/10.1016/S2213-8587(18)30315-2 3
Review
the relation between reduction of HbA1c and the risk (so-called dead-in-bed syndrome). Mortality data are
of major adverse cardiovascular events in trials of limited to children and adolescents on contemporary
medication that did not increase hypoglycaemia. The insulin therapy, but mortality in this population compared
results showed that lowering HbA1c in these trials with the age-matched background population is
conferred a significant risk reduction for major adverse significantly higher.5,44,45 Under-reporting of diabetes-
cardiovascular events, whereas no such association was related death is less likely to occur in children and
seen in trials involving traditional therapy (the side- adolescents because of the lower rates of comorbid
effects of which include hypoglycaemia). disease compared with adults. Most reports describe a
two to four times increase in standardised mortality in
Hypoglycaemia and cardiovascular disease in children and adolescents with type 1 diabetes; diabetic
specific populations ketoacidosis is the most frequently described cause of
Older people and people with comorbidities death, but hypoglycaemia and dead-in-bed syndrome
Many clinical practice guidelines recommend avoiding also feature in most surveys.44,46 Death associated with
strict glycaemic control in older people (eg, people older hypoglycaemia in children and adolescents might follow
than 75 years) with diabetes, and frail individuals with a seizure, or be the result of an accident or drowning,
comorbidities and end-stage chronic illness. Benefits of and might not invoke a cardiovascular cause.
strict control in these populations have not been shown
and potential harm is increased, largely related to Cardiovascular effects of hypoglycaemia
hypoglycaemia. Despite these recommendations, over There is accumulating evidence that hypoglycaemia can
treatment is common in such patients, particularly with cause cardiac dysfunction and sudden death. This
insulin or sulfonylureas.35 As expected, this overtreatment evidence includes case reports of various cardiac
increases the risk of hypoglycaemia associated with arrhythmias induced by hypoglycaemia and studies
increasing age per se, a high burden of comorbidities, reporting abnormal cardiac repolarisation. Most of the
diminished cognitive ability, and diminished renal clinical studies have been in either people without
function.36 Paradoxically, poorer glycaemic control is also diabetes or people with type 1 diabetes; relatively few
associated with hypoglycaemia in this population.37 studies have involved patients with type 2 diabetes.
Findings from observational studies have identified an Hypoglycaemia activates the sympathoadrenal system
association between hypoglycaemia and mortality in older causing profuse secretion of catecholamines that exert
people,38,39 but its association with cardiovascular disease profound haemodynamic and haemorrheological effects
has not been properly assessed and has to be extrapolated (figure 2). Sympathetic stimulation causes a rapid
from studies in populations younger than 75 years old. increase in heart rate, myocardial contractility and cardiac
output, and central systolic pressure falls secondary to
Pregnancy increased elasticity of large vessels.48,49 Plasma potassium
The overall incidence of acute myocardial infarction is rapidly declines,50 inducing electrophysiological and
increased in pregnancy by three to five times, particularly electro
cardiographic changes, which might provoke
in women with pre-existing diabetes, and the risk of abnormal cardiac conduction and repolarisation.51
mortality is high in patients with diabetes and myocardial Furthermore, acute changes occur in blood coagulability,
infarction.40 An interaction between hypoglycaemia and cell adhesion, endothelial dysfunction, and inflammatory
ischaemic heart disease during pregnancy has not been markers in response to hypoglycaemia. These effects
reported to our knowledge, but severe hypoglycaemia is have the potential to compromise endothelial function,
very frequent in pregnant women with diabetes treated blood flow, and tissue perfusion, risking intravascular
with insulin, particularly in the first trimester.41 In one coagulation and thrombosis.52
study of 972 pregnant women with type 1 diabetes, two of Antecedent hypoglycaemia blunts the autonomic
four maternal deaths that occurred were attributed to responses to cardiac stress for several hours in people
hypoglycaemia-induced dead-in-bed syndrome.42 This without diabetes53 and this transient impairment of auto
association cannot be used as an argument against nomic cardiac reflexes could affect cardiac vulnerability
intensive glycaemic management during pregnancy, to a subsequent stress. The haemorrheological and
because of its very clear benefits in terms of fetal outcomes, inflammatory responses to hypoglycaemia persist for
but does argue for greater attention to be paid to achieving several days in patients with type 2 diabetes.54 Functional
normoglycemia without excess hypoglycaemia.43 abnormalities that persist long after restoration of
normoglycaemia could create an intravascular milieu that
Children and adolescents is conducive to a thrombotic event.55 Paradoxically, greater
Data regarding the cardiovascular consequences of hypoglycaemia-associated cardiovascular mortality was
hypoglycaemia in children and adolescents with diabetes reported in patients on standard therapy who maintained
are sparse. Although speculative, the most likely effect of higher HbA1c concentrations than in those treated
hypoglycaemia on the cardiovascular system in those intensively in the ACCORD Trial.14 It is unclear whether
younger than 18 years is sudden unexpected death in bed frequent exposure to hypoglycaemia increases the risk of a
4 www.thelancet.com/diabetes-endocrinology Published online March 26, 2019 http://dx.doi.org/10.1016/S2213-8587(18)30315-2
Review
↑CRP ↑VEGF ↑IL-6
Inflammation
↑Macrophage activation
Blood coagulation
Hypoglycaemia Endothelial dysfunction
abnormalities
Sympathoadrenal response
↑Vasodilatation
↑Epinephrine
↑Platelet activation
↑Factor VIII Rhythm abnormalities Haemodynamic changes
Heart rate variability ↑Heart workload
↑Contractility
↑Output
Figure 2: Pathophysiological cardiovascular consequences of hypoglycaemia
Adapted from Desouza et al,47 by permission of the American Diabetes Association. CRP=C-reactive protein. VEGF=vascular endothelial growth factor. IL-6=interleukin 6.
cardiovascular event, or whether it might even have a Acute hypoglycaemia also evokes a pro-inflammatory
protective effect through a diminished sympathoadrenal response that might contribute to endothelial dysfunction
response due to repeated hypoglycaemia. and be pro-atherogenic. In individuals with and without
In people with type 2 diabetes, many of whom have diabetes, hypoglycaemia leads to increases in cluster
premature cardiovascular disease, the transient haemo of differentiation 40 (CD40) expression on monocytes
dynamic changes associated with hypoglycaemia might and plasma soluble CD40 ligand concentrations, as well as
provoke acute cardiovascular events such as myocardial increases in intercellular adhesion molecule 1, vascular
ischaemia and infarction, cardiac failure, and cardiac cell adhesion protein 1, E-selectin, vascular endothelial
arrhythmias. Anecdotal cases have been described of acute growth factor, and the cytokines interleukin (IL)-6, IL-8,
cardiovascular events being precipitated by hypoglycaemia, and tumour necrosis factor α. This pro-inflammatory
and ischaemic electrocardiogram changes have been response might worsen the chronic inflammation and
reported, with and without the development of angina.56 endothelial dysfunction that is common in diabetes.
Certainly, endothelial dysfunction with impaired nitric
Potential mechanisms oxide-mediated vasodilation is evident during hypo
The body responds to the systemic challenge of glycaemia and exacerbated after two episodes of
hypoglycaemia by initiating a counterregulatory defence hypoglycaemia.58 Repeated hypoglycaemia in type 1
response that involves multiple stress pathways and diabetes is also associated with flow-mediated endothelial
activation of the sympathetic nervous system. Insulin- dysfunction and increased intima-media thickness.61
induced hypoglycaemia is a profound systemic stress, However, this response might be modified by recurrent
which has substantial haemodynamic, pro-inflammatory, exposure to hypoglycaemia, where studies in non-diabetic
and pro-atherothrombotic effects, as well as increasing rodents show blunting of both the inflammatory response
the potential for cardiac arrhythmias. and sympathoadrenal responses to hypoglycaemia.62
Hypoglycaemia also stimulates an increase in plasma Ratter and colleagues63 have shown that, in people
aldosterone via activation of the renin–angiotensin without diabetes and in people with type 1 diabetes,
system, which through activation of the mineralocorticoid hypoglycaemia promoted mobilisation of specific
receptor might exacerbate endothelial dysfunction.57 leucocyte subsets from the marginal pool and induced
Increased cardiac workload during acute hypoglycaemia is pro-inflammatory changes in immune cells with
accompanied by changes in vascular haemorrheology, exaggerated cytokine responses to microbial stimulation.
with increased platelet activation, diminished fibrinolytic However, although hypoglycaemia can activate multiple
balance, and elevated haemostasis.58 However, recurrent pathways that potentially lead to endothelial dysfunction,
hypoglycaemia leads to a suppression of the sympatho a similar response to acute hypoglycaemia in terms of
adrenal response to hypoglycaemia59 and reduced inflammatory cytokine and selectin release is seen with
β-adrenergic sensitivity.60 Thus, the haemodynamic effects acute exercise in people without diabetes with and
of hypoglycaemia might be paradoxically less profound in without coronary artery disease,64 and exercise is generally
individuals at the greatest risk of severe hypoglycaemia. considered to be cardioprotective.
www.thelancet.com/diabetes-endocrinology Published online March 26, 2019 http://dx.doi.org/10.1016/S2213-8587(18)30315-2 5
Review
300 Day 1 Day 2
severe hypoglycaemia.66 These observations suggest that
the ability of the host’s defences to cope with the stress of
250 hypoglycaemia is impaired by pre-existing diabetes and
that the inflammatory response to hypoglycaemia might
Glucose concentration (mg/dL)
200 be amplified by rebound hyperglycaemia on recovery.
Clinical episodes of hypoglycaemia have been reported
150 to cause atrial fibrillation, multiple ventricular ectopics,
and ventricular tachycardia. A pivotal report by Tattersall
100 and Gill67 in 1991 presented strong circumstantial evidence
70 that hypoglycaemia was implicated in the sudden overnight
50
30
death of young people with type 1 diabetes. This mode
10 of death, described as the dead-in-bed syndrome, has since
0
08:00 12:00 16:00
20:00 00:00 04:00 08:00 been reported in a series of epidemiological studies, with a
Time paper from 2011 calculating a ten-times increase in sudden
Patient actions (as recovered from CGM and insulin pump): death in young people with type 1 diabetes compared with
5
Units
5
3·0
1·4
1·4
1·0
0·
Correction boluses
Exercise the non-diabetic population,68 and the circumstances of the
Meal or food death make an arrhythmia a likely agonal event.
An example of sudden death occurring during profound
Figure 3: Continuous glucose monitoring trace showing sudden death during hypoglycaemia
The graph shows glucose concentrations captured by a CGM system for the evening before and the morning of a hypoglycaemia was captured in a case of a young man
patient’s death. The patient’s measured and entered calibrations are represented by the four circles. Timing of the (age 23 years) with type 1 diabetes, in which the continuous
patient’s meals, exercise, and correction insulin boluses are represented by the bars along the bottom of the graph. glucose monitoring (CGM) trace demonstrated the low
Reproduced from Tanenberg et al,69 by permission of the American Association of Clinical Endocrinologists.
glucose concentration at the time of death (figure 3). With
CGM=continuous glucose monitoring.
no other cause found at autopsy in an apparently otherwise
healthy individual, the cause of death seemed to have
been a cardiac arrhythmia.69 Experimentally-induced
hypoglycaemia in people with type 1 and type 2 diabetes70,71
has shown that hypoglycaemia results in pro-arrhyth
mogenic cardiac repolarisation with prolongation of the
QT interval corrected for heart rate (figure 4). It has been
hypothesised that people with underlying polymorphisms
of the ion channels, which contribute to the cardiac
conduction system, might be particularly vulnerable.72
Other experimental and observational studies have shown
abnormalities of cardiac repolari sation along with
profound bradycardia in some susceptible individuals
with type 1 diabetes,73 but what confers susceptibility or
triggers the fatal event is unknown.
Profound hypoglycaemia (glucose <1·0 mmol/L) in
QTc 456 ms QTc 610 ms rodent models leads to QT prolongation, ventricular
HR 66 bpm HR 61 bpm ectopy, and high-degree heart block dependent on
5·0 mM 2·5 mM duration and severity of hypoglycaemia.74 Interestingly,
mortality in this rodent model of profound hypoglycaemia
Figure 4: Abnormal cardiac repolarisation during experimental hypoglycaemia was exacerbated by diabetes, but for the most part reversed
Typical QT measurement with a screen cursor placement during euglycaemia (left), showing a clearly defined
T wave, and hypoglycaemia (right), showing prolonged repolarisation and a prominent U wave. Reproduced from
by preceding exposure to recurrent hypoglycaemia and
Marques et al,70 by permission of John Wiley & Sons. HR=heart rate. QTc=corrected QT. potassium replacement; intra-cerebroventricular glucose
infusion or β-adrenergic blockade reduced severe hypo
It is important to recognise that hypoglycaemia in both glycaemia-induced arrhythmias and overall mortality.66
type 1 and type 2 diabetes occurs on the background of Hypoglycaemia-induced arrhythmias are also a potential
chronic exposure to high glucose concentrations, and the contributor to the increased cardiac mortality seen in the
treatment (or overtreatment) of hypoglycaemia often ACCORD trial.2 Studies in an ambulatory setting
results in rebound hyperglycaemia. This increased combining Holter monitoring and continuous interstitial
glucose variability might induce an additional inflam glucose measurement have documented relative increases
matory stimulus. Rebound hyperglycaemia following in the frequencies of bradycardia and atrial ectopic activity
hypoglycaemia has a greater effect in impairing during hypoglycaemia.75 In a detailed study of the
endothelial function and activating thrombosis than does arrhythmic effects of hypoglycaemia in people with type 2
hypoglycaemia alone.65 Pre-existing diabetes also worsens diabetes undertaken with a hypoglycaemic clamp, Chow
cardiac outcomes in a rodent model of exposure to very and colleagues76 showed that an initial vagal withdrawal
6 www.thelancet.com/diabetes-endocrinology Published online March 26, 2019 http://dx.doi.org/10.1016/S2213-8587(18)30315-2
Review
during hypoglycaemia resulted in an increase in heart rate, include situational characteristics (eg, in a public setting
but with more prolonged hypoglycaemia, vagal reactivation as opposed to occurring when alone), social implications
then resulted in relative bradycardia, consistent with (eg, in front of friends or colleagues), and emotional
earlier observations.77 By contrast, people without diabetes consequences (level of fearfulness or perceived danger) of
had a persistent increase in heart rate during the episode. Changes that patients or relatives have made
hypoglycaemia in the study, implying continued vagal in diabetes management behaviours and routine in
withdrawal. Chow and colleagues also noted that people response to an episode of hypoglycaemia should also be
with type 2 diabetes had a higher heart rate, lower heart carefully assessed.
rate variability at baseline, and greater changes in the The rare but well recognised dead-in-bed syndrome
duration and heterogeneity of repolarisation abnormalities presents a special problem and an ethical dilemma for
during hypoglycaemia. Why people with type 2 diabetes health-care practitioners regarding patient and family
respond differently to hypoglycaemia in this context is not education about hypoglycaemia. To our knowledge, no
known, but hypoglycaemia has been shown to reduce studies have specifically explored the potential effect of
baroreflex sensitivity, shift the blood pressure thresholds mortality secondary to hypoglycaemia on the family
for baroreflex activation, and reduce the range of R-R of those affected. However, many patients and their
interval responses.78 Thus, pre-existing abnormalities in families are concerned that severe hypoglycaemia overnight
autonomic function might contribute to an increased might be fatal, particularly if they have witnessed a
propensity to cardiac arrhythmias. hypoglycaemic seizure.85 Although there has been no
apparent research on the psychological effects on patients’
Clinical approaches families, there is anecdotal evidence that most clinicians do
Psychological issues not raise the issue of fatal cardiac arrhythmias caused by
The negative consequences of hypoglycaemia, ranging hypoglycaemia in discussions with patients and family
from unpleasant symptoms to potentially dangerous members. Although nocturnal hypoglycaemia is common,
situations, often cause patients and family members to fatal episodes are very rare. Thus, presenting it as a possible
develop fear of hypoglycaemia. Numerous studies have outcome might produce unwarranted high levels of anxiety.
documented the detrimental effect of fear of hypo Further research is required to understand the risk factors
glycaemia on quality of life across different countries and and mechanisms associated with fatal nocturnal hypo
cultures.79,80 Overall, high levels of fear of hypoglycaemia glycaemia, which would help to guide the development of
are most commonly associated with a history of episodes appropriate patient education and recommendations.
of severe hypoglycaemia, especially episodes resulting in
cognitive disorientation, social embarrassment, loss of Basic clinical approaches
consciousness, accidents, and physical injury. People Clinicians prescribing insulin and sulfonylureas must
with impaired awareness of hypoglycaemia, who are at prepare patients for hypoglycaemia that might occur when
higher risk of severe hypoglycaemia, often have these medications are used. In a busy practice setting,
substantial fear of hypoglycaemia, although about a third such patients should be referred to diabetes education for
of them paradoxically have low scores on the fear-of- comprehensive instruction on recognising, anticipating,
hypoglycaemia scales.81 Parents of children with type 1 and treating hypoglycaemia. Learning to identify people
diabetes are particularly vulnerable to high levels of fear with impaired awareness of hypoglycaemia is an important
of hypoglycaemia, including anxiety related to nocturnal clinical skill for all practitioners. They might consider
episodes of hypoglycaemia, which is a major source of using the questionnaires developed by the ADA Hypo
emotional stress.82,83 glycaemia Working Group1 to ensure a systematic
Fear of hypoglycaemia might also have important assessment is done at each visit. Clinician and patient
implications for diabetes management and control. Some educational materials have also been developed by the
patients might cope with their fear and try to mitigate the International Hypoglycaemia Study Group86 to enhance
threat of hypoglycaemia by maintaining their blood understanding of this complication of diabetes treatment.
glucose levels in a higher range, leading to additional time Advances in diabetes care have provided new approaches
spent in hyperglycaemia. Several studies have shown that that reduce the risk of hypoglycaemia in patients with
high levels of fear of hypoglycaemia are associated with diabetes.87 Insulin-requiring patients with both types of
poorer metabolic control, including more frequent diabetes might find that they have less hypoglycaemia if
hyperglycaemic blood glucose readings and higher HbA1c they use a long-acting basal insulin, such as insulin
levels.84 Although patients might be reluctant to report degludec, which has been shown to reduce rates of severe
episodes of severe hypoglycaemia to their health-care hypoglycaemia in both type 1 and type 2 diabetes compared
practitioners, it is crucial to assess these episodes in with insulin glargine U100.88–90 Individuals with type 1
clinical settings. In addition to assessing factors such as diabetes at increased hypoglycaemic risk might benefit
causes, frequency, and severity, it is important to ask from an insulin pump70 and the addition of real-time
patients and family members about aspects of the episode CGM to an existing insulin regimen has also been shown
likely to be associated with psychological effects. These to reduce hypoglycaemia.92 Use of a threshold-suspend
www.thelancet.com/diabetes-endocrinology Published online March 26, 2019 http://dx.doi.org/10.1016/S2213-8587(18)30315-2 7
Review
pump93 or a hybrid closed-loop pump94 can lower rates of cardiovascular disease risk. In the ADVANCE study, only
hypoglycaemia in patients with type 1 diabetes without plasma levels of IL-6, but not those of C-reactive protein
jeopardising glycaemic control. Patients with impaired or fibrinogen, were independently associated with cardio
awareness of hypo glycaemia and repeated episodes of vascular events or death in patients with type 2 diabetes.97
severe hypoglycaemia, despite ongoing efforts to avoid it, In the Edinburgh Type 2 Diabetes Study, there was no
might be eligible for islet transplantation, when available.95 evidence that increased levels of inflammatory factors
affected the relation between severe hypoglycaemia and
Reducing hypoglycaemia in patients at high cardiovascular complications in people with type 2
cardiovascular risk diabetes.86 It is also unclear how long, pro-inflammatory
The ADA standards of care recommend that glycaemic conditions and reduced endothelial function persist after
targets are changed in patients who have clinically resolution of hypoglycaemia.
significant hypoglycaemia or impaired awareness of Hyperglycaemia-induced modifications of the
hypoglycaemia.96 For patients on insulin or sulfonylureas, epigenome have been suggested to account for the
there should be a stronger emphasis on cardiovascular phenomenon of glycaemic memory—ie, the observation
comorbidities, with glucose targets shifted upwards and that vascular damage caused by previous chronic
HbA1c targets increased to 55 mmol/mol (7·5%) if hyperglycaemia persists despite good current glycaemic
necessary to help vulnerable patients avoid hypoglycaemia. control.98 Epigenetic factors might also contribute to the
In patients with type 2 diabetes, reduction in effects of hypoglycaemia on the cardiovascular system.
hypoglycaemia risk might be accomplished by switching State-of-the-art imaging techniques, including PET,
to a regimen that does not include insulin or a functional MRI, and magnetic resonance spectroscopy,
sulfonylurea, which might also allow the benefits of a are needed to visualise with greater precision how
lower HbA1c to be achieved.96 hypoglycaemia affects cardiac and cerebral perfusion and
Although the use of new technologies including the uptake and metabolism of nutrients in these organs.99
pumps, CGM, and insulin analogues, might reduce the It is also important to establish whether the effects of
incidence of hypoglycaemia, there is no evidence that recurrent episodes of hypoglycaemia are cumulative or
this translates into lower cardiovascular disease risk or diminutive. In healthy people, exposure to two consecutive
improved survival in people with diabetes, perhaps hypoglycaemic episodes has been shown to result in
because of the short duration of the trials and the low greater impairment of endothelial function than one
baseline cardiovascular risk of study participants. The episode, although this was not the case for the elevation of
study that has come closest to finding such an effect was pro-inflammatory cytokines.100 By contrast, it has been
the DEVOTE trial (Trial Comparing Cardiovascular reported that the acute inflammatory responses to
Safety of Insulin Degludec Versus Insulin Glargine in hypoglycaemia were blunted in patients with type 1
Subjects With Type 2 Diabetes at High Risk of diabetes and impaired awareness of hypoglycaemia,
Cardiovascular Events).90 In the trial, which was done in possibly because of the reduced counterregulatory
patients with type 2 diabetes at increased risk of hormone response.63 In rats, recurrent hypoglycaemia
cardiovascular disease, the use of insulin degludec protects against hypoglycaemia-induced death or neuronal
(compared with insulin glargine U100) reduced the damage,101,102 rather than amplifying the risk for these
incidence of severe hypoglycaemia by 40%, as well as a events. Conversely, an exaggerated counterregulatory
non-significant 9% reduced incidence of cardiovascular hormone response, particularly of epinephrine and
events. cortisol, could explain why patients with poor glycaemic
control might be at an increased risk when they experience
Future directions a hypoglycaemic event.14
Although the acute and potentially harmful responses to Experimental research on severe hypoglycaemia has
non-severe controlled hypoglycaemia have been studied mainly been done in rat models. Such experiments cannot
in detail, knowledge of the effects of severe or long-lasting be undertaken in human beings for ethical reasons, and
(eg, nocturnal) hypoglycaemia is scarce. It is possible that replication should be sought in larger animal models with
the documented responses to non-severe hypoglycaemia cardiovascular function that better resembles human
might be exaggerated and some effects might only occur physiology.103
during severe hypoglycaemia. Furthermore, knowledge Little is known about differences in the vulnerability to
about the duration of potential adverse responses is the potentially deleterious cardiovascular effects of
absent. This issue is important since a very transient pro- iatrogenic hypoglycaemia, or the underlying mechanisms,
coagulant inflammatory response is less likely to enhance between various patient subgroups. For example, it is
the risk of cardiovascular morbidity than a more prolonged unlikely that hypoglycaemia exerts the same effect, or the
one. It is also unclear whether or not exposure to repeated same cardiovascular response, in young people with type 1
moderate hypoglycaemia has a cumulative effect. diabetes who are otherwise healthy as in older people with
A better understanding of modulating factors is needed type 2 diabetes and advanced atherosclerosis. Susceptibility
to explain the relation between hypoglycaemia and to cardiac arrhythmias during hypoglycaemia seems to be
8 www.thelancet.com/diabetes-endocrinology Published online March 26, 2019 http://dx.doi.org/10.1016/S2213-8587(18)30315-2
Review
Search strategy and selection criteria with increased cardiovascular risks in populations treated
We identified references for this Review through searches of with medication that do not cause hypoglycaemia as a
PubMed for articles published in English from Jan 1, 1971, to side-effect. Thus, iatrogenic hypoglycaemia seems to be a
Dec 31, 2018, using the terms “hypoglycaemia”, “fear of risk factor for death in people with diabetes. However,
hypoglycaemia”, “pregnancy”, “cardiovascular mortality”, there remains the prospective evidence that strict
“cardiovascular disease”, “low glucose”, “myocardial glycaemic control applied early in the course of both
infarction”, “stroke”, “insulin treatment”, and “intensive type 1 and type 2 diabetes reduces mortality, despite an
insulin therapy”, in combination with the term “diabetes”. increase in hypoglycaemia risk. Collectively, these
Relevant articles were also identified through searches of the findings emphasise the importance of carefully balancing
authors’ personal files, Google Scholar, and the Springer the potential benefits and potential harms, and
Online Archives Collection, as well as from reference lists of individualising glycaemic goals in people with diabetes
identified articles. Articles were initially selected for inclusion treated with insulin or an insulin secretagogue.
on the basis of the opinion of the contributing authors, with
Contributors
each section covered by two or three authors with particular SAA, BC, and YL read and contributed to successive drafts. BMF
expertise. The chosen references were also reviewed by the contributed to literature review and sections on cardiovascular effects of
wider group when reading successive drafts. hypoglycaemia and read and contributed to successive drafts. SRH took
responsibility for the overall manuscript, contributed to the literature
review, wrote first drafts of sections on mortality and cardiovascular
disease, and combined all contributions into the first and subsequent
confined to a few individuals,104 but what determines this drafts. RJM contributed to the literature review, wrote the first draft
of the section on potential mechanisms and read and contributed to
susceptibility and how those at risk can be identified is successive drafts. KK contributed to the literature review, wrote the first
unknown. Identifying people who are at increased risk of draft of the epidemiology section, prepared the table and read and
arrhythmias during hypoglycaemia is obviously important contributed to successive drafts. PA contributed to the literature review,
with respect to balancing benefits of glycaemic control wrote the first draft of the pregnancy section and read and contributed
to successive drafts. PEC contributed to literature review and sections on
optimisation against the risks of hypoglycaemia. Further mortality and cardiovascular disease, epidemiology and the conclusion
more, establishing that these effects are present in and read and contributed to successive drafts. LG-F contributed to the
individuals without comorbidities would help to establish literature review, wrote the first draft of the section dealing with
that hypoglycaemia is a risk factor rather than simply a psychological issues and the section on clinical approaches and read and
contributed to successive drafts. ERS participated in writing the first
risk marker. draft and read and contributed to successive drafts. BEdG wrote the first
The existing gaps in the evidence discussed in this draft of the future directions section and read and contributed to
Review are the focus of the comprehensive IMI-funded successive drafts. TJ contributed to the literature review, wrote the first
research project Hypoglycaemia redefining solutions for draft of the paediatric section and read and contributed to successive
drafts. SZ contributed to the literature review, wrote the first draft of the
better lives (Hypo-RESOLVE), which is addressing a epidemiology section and table and read and contributed to successive For more on Hypo-RESOLVE, see
number of areas related to diabetic hypoglycaemia. These https://hypo-resolve.eu
drafts. LAL contributed to data interpretation and critical review and
include enlarging the evidence base underpinning a input into successive drafts. UP-B contributed to the first draft of the
future directions section and read and contributed to successive drafts.
universally accepted classification of hypoglycaemia,
understanding the consequences of hypoglycaemia with The International Hypoglycaemia Study Group
UK Stephanie A Amiel (Division of Diabetes and Nutritional Sciences,
particular focus on cardiovascular disease, and
King’s College London, London); Brian M Frier (Queen’s Medical
measuring hypoglycaemic events more accurately during Research Institute, University of Edinburgh, Edinburgh); Simon R Heller
clinical trials with the advent of continuous glucose (University of Sheffield and Sheffield Teaching Hospitals NHS
monitoring technology. Foundation Trust, Sheffield); Rory J McCrimmon (Division of Molecular
& Clinical Medicine, School of Medicine, University of Dundee, Dundee);
Kamlesh Khunti (University of Leicester, Leicester). Colombia Pablo
Conclusions Aschner (Javeriana University School of Medicine, San Ignacio University
It has been known that hypoglycaemia can be fatal since Hospital, and Colombian Diabetes Association, Bogota). USA
the introduction of insulin therapy nearly a century ago. Belinda Childs (Great Plains Diabetes, Wichita, KS); Philip E Cryer
(Washington University in St Louis, St Louis, MO);
Numerous reports exist of an association between Linda Gonder-Frederick (Department of Psychiatry and Neurobehavioral
hypoglycaemia and cardiovascular events or death, with Sciences, and Behavioral Medicine Center, University of Virginia Health
statistical evidence that the association is not entirely System, Charlottesville, VA); Elizabeth R Seaquist (Division of
attributable to confounding by comorbidities. In this Endocrinology and Diabetes, Department of Medicine, University of
Minnesota, Minneapolis, MN). Netherlands Bastiaan E de Galan
Review, we have discussed the many mechanisms by (Department of Internal Medicine, Radboud University Nijmegen Medical
which hypoglycaemia might increase the risk of Centre, Nijmegen). Australia Timothy Jones (School of Paediatrics and
cardiovascular disease and mortality and oppose the Child Health, Telethon Institute for Child Health Research, University
potential benefits of strict glycaemic control. Lower of Western Australia, and Department of Endocrinology and Diabetes,
Princess Margaret Hospital for Children, Perth, WA); Sophia Zoungas
HbA1c levels are associated with an increased frequency (School of Public Health and Preventive Medicine, Monash University,
of severe hypoglycaemia and with increased mortality Melbourne, VIC). Canada Lawrence A Leiter (Division of Endocrinology
and cardiovascular events in people with diabetes.105 and Metabolism, St Michael’s Hospital, and University of Toronto,
Importantly, low HbA1c levels do not seem to be associated Toronto, ON). China Yingying Luo (Endocrinology and Metabolism
www.thelancet.com/diabetes-endocrinology Published online March 26, 2019 http://dx.doi.org/10.1016/S2213-8587(18)30315-2 9
Review
Department, Peking University People’s Hospital, Beijing). Denmark 9 Patel A, MacMahon S, Chalmers J, et al. Intensive blood glucose
Ulrik Pedersen-Bjergaard (Department of Clinical Medicine, University control and vascular outcomes in patients with type 2 diabetes.
of Copenhagen, and Department of Endocrinology & Nephrology, N Engl J Med 2008; 358: 2560–72.
Nordsjællands Hospital, Hillerød). 10 Zoungas S, Patel A, Chalmers J, et al. Severe hypoglycemia and
risks of vascular events and death. N Engl J Med 2010; 363: 1410–18.
Declaration of interests
11 Pieber TR, Marso SP, McGuire DK, et al. DEVOTE 3: temporal
BMF has served as a consultant or speaker for Novo Nordisk, Lilly, relationships between severe hypoglycaemia, cardiovascular
Boehringer Ingelheim, Roche, Abbott, and MSD. SRH has served as outcomes and mortality. Diabetologia 2018; 61: 58–65.
a consultant or speaker from Lilly, Novo Nordisk, Takeda, Boeringher 12 Heller SR, Bergenstal RM, White WB, et al. Relationship of glycated
Ingelheim, Mannkind, Sanofi, Zealand Pharma and UN-EEG. RJM has haemoglobin and reported hypoglycaemia to cardiovascular
served as a consultant or speaker for Novo Nordisk, Sanofi, Eli Lilly and outcomes in patients with type 2 diabetes and recent acute coronary
has received research grant support from Novo Nordisk and the Helmsley syndrome events: the EXAMINE trial. Diabetes Obes Metab 2017;
Trust. KK has served as a consultant or speaker for AstraZeneca, 19: 664–71.
Boehringer Ingelheim, Janssen, Lilly, MSD, Novartis, Novo Nordisk, 13 Mellbin LG, Rydén L, Riddle MC, et al. Does hypoglycaemia
and Sanofi and has received research grant support from AstraZeneca, increase the risk of cardiovascular events? A report from the
Boehringer Ingelheim, Lilly, Novartis, Novo Nordisk, Roche, and Sanofi. ORIGIN trial. Eur Heart J 2013; 34: 3137–44.
PA has served on scientific advisory boards, served as a speaker, or both 14 Bonds DE, Miller ME, Bergenstal RM, et al. The association
for AstraZeneca, Boehringer Ingelheim/Lilly, Bristol-Myers Squibb, between symptomatic, severe hypoglycaemia and mortality in type 2
GlaxoSmithKline, Janssen, Merck Sharp & Dohme (MSD), Novartis, diabetes: retrospective epidemiological analysis of the ACCORD
and Sanofi. BC has served as a consultant or speaker for Xeris study. BMJ 2010; 340: b4909.
Pharmaceuticals. PEC has served as a consultant or speaker to Novo 15 Lee AK, Warren B, Lee CJ, et al. The association of severe
Nordisk. LG-F has served as a consultant or speaker for Abbott Diabetes hypoglycemia with incident cardiovascular events and mortality in
adults with type 2 diabetes. Diabetes Care 2018; 41: 104–11.
Care, AstraZeneca, Dexcom, Johnson and Johnson, and Merck and
received research funding from Abbott Diabetes Care. LG-F distributes 16 Lu CL, Shen HN, Hu SC, Wang JD, Li CY. A population-based study
of all-cause mortality and cardiovascular disease in association with
and licences for the Hypoglycemia Fear Survey through HFS-Global LLC
prior history of hypoglycemia among patients with type 1 diabetes.
in agreement with the University of Virginia Licensing and Ventures
Diabetes Care 2016; 39: 1571–78.
Group. ERS has served as a consultant or speaker for Sanofi, Lilly, Zucara,
17 Goto A, Goto M, Terauchi Y, Yamaguchi N, Noda M.
MannKind, NovoNordisk, and WebMD and has received research funding
Association between severe hypoglycemia and cardiovascular
from Lilly. BEdG has served on scientific advisory boards for Novo disease risk in Japanese patients with type 2 diabetes.
Nordisk and received research grant support from AstraZeneca and J Am Heart Assoc 2016; 5: e002875.
Sanofi. TJ has served as a consultant or speaker for Novo Nordisk, Lilly, 18 Leong A, Berkowitz SA, Triant VA, et al. Hypoglycemia in diabetes
Medtronic, and Sanofi. SZ has served as a consultant or speaker for mellitus as a coronary artery disease risk factor in patients at
AstraZeneca, Novo Nordisk, and MSD Australia. LAL has acted as a elevated vascular risk. J Clin Endocrinol Metab 2016; 101: 659–68.
consultant or speaker for AstraZeneca, Boehringer Ingelheim, Eli Lilly, 19 Cha SA, Yun JS, Lim TS, et al. Severe hypoglycemia and
Janssen, Merck, Novo Nordisk, Sanofi, and Servier and has received cardiovascular or all-cause mortality in patients with type 2 diabetes.
research grant support from AstraZeneca, Boehringer Ingelheim, Eli Lilly, Diabetes Metab J 2016; 40: 202–10.
GlaxoSmithKline, Janssen, Novo Nordisk, and Sanofi. UP-B has served as 20 Sejling AS, Schouwenberg B, Faerch LH, Thorsteinsson B,
a consultant or speaker for AstraZeneca, Bristol-Myers Squibb, Novo de Galan BE, Pedersen-Bjergaard U. Association between
Nordisk, Sanofi-Aventis, UN-EEG and has received research grant support hypoglycaemia and impaired hypoglycaemia awareness and
from Novo Nordisk. SAA and YL declare no competing interests. mortality in people with type 1 diabetes mellitus. Diabet Med 2016;
33: 77–83.
Acknowledgments 21 Luk AO, Ho TS, Lau ES, et al. Association of self-reported recurrent
The International Hypoglycaemia Study Group (IHSG) is supported mild hypoglycemia with incident cardiovascular disease and
through an unrestricted educational grant from Novo Nordisk, awarded all-cause mortality in patients with type 2 diabetes: prospective
to the University of Sheffield (Sheffield, UK) on behalf of the members of analysis of the Joint Asia Diabetes Evaluation Registry.
the IHSG. The rationale for the formation of IHSG is that hypoglycaemia Medicine (Baltimore) 2016; 95: e5183.
is an under-recognised problem that deserves greater awareness and 22 Freemantle N, Danchin N, Calvi-Gries F, Vincent M, Home PD.
focus across the health-care community. The group’s ultimate goal is to Relationship of glycaemic control and hypoglycaemic episodes to
improve the lives of patients with diabetes. Novo Nordisk representatives 4-year cardiovascular outcomes in people with type 2 diabetes
had no role in the design or content of the Review, were unaware of its starting insulin. Diabetes Obes Metab 2016; 18: 152–58.
content, and had no right to approve or disapprove the final content. 23 Khunti K, Davies M, Majeed A, Thorsted BL, Wolden ML, Paul SK.
Hypoglycemia and risk of cardiovascular disease and all-cause
References mortality in insulin-treated people with type 1 and type 2 diabetes:
1 Seaquist ER, Anderson J, Childs B, et al. Hypoglycemia and diabetes: a cohort study. Diabetes Care 2015; 38: 316–22.
a report of a workgroup of the American Diabetes Association and
24 Bedenis R, Price AH, Robertson CM, et al. Association between
the Endocrine Society. Diabetes Care 2013; 36: 1384–95.
severe hypoglycemia, adverse macrovascular events, and
2 Gerstein HC, Miller ME, Byington RP, et al. Effects of intensive inflammation in the Edinburgh Type 2 Diabetes Study.
glucose lowering in type 2 diabetes. N Engl J Med 2008; 358: 2545–59. Diabetes Care 2014; 37: 3301–08.
3 Bliss M. The discovery of insulin. Chicago: University of Chicago 25 Lung TW, Petrie D, Herman WH, et al. Severe hypoglycemia and
Press, 1982. mortality after cardiovascular events for type 1 diabetic patients in
4 Tunbridge WMG. Factors contributing to deaths of diabetics under Sweden. Diabetes Care 2014; 37: 2974–81.
fifty years of age. Lancet 1981; 318: 569–72. 26 Rathmann W, Kostev K, Gruenberger JB, Dworak M, Bader G,
5 Gagnum V, Stene LC, Jenssen TG, et al. Causes of death in Giani G. Treatment persistence, hypoglycaemia and clinical
childhood-onset type 1 diabetes: long-term follow-up. Diabet Med outcomes in type 2 diabetes patients with dipeptidyl peptidase-4
2017; 34: 56–63. inhibitors and sulphonylureas: a primary care database analysis.
6 Stratton IM, Adler AI, Neil HA, et al. Association of glycaemia with Diabetes Obes Metab 2013; 15: 55–61.
macrovascular and microvascular complications of type 2 diabetes 27 Hsu PF, Sung SH, Cheng HM, et al. Association of clinical
(UKPDS 35): prospective observational study. BMJ 2000; 321: 405–12. symptomatic hypoglycemia with cardiovascular events and total
7 Holman RR, Paul SK, Bethel MA, Matthews DR, Neil HA. 10-year mortality in type 2 diabetes: a nationwide population-based study.
follow-up of intensive glucose control in type 2 diabetes. Diabetes Care 2013; 36: 894–900.
N Engl J Med 2008; 359: 1577–89. 28 Zhao Y, Campbell CR, Fonseca V, Shi L. Impact of hypoglycemia
8 Duckworth W, Abraira C, Moritz T, et al. Glucose control and associated with antihyperglycemic medications on vascular risks in
vascular complications in veterans with type 2 diabetes. veterans with type 2 diabetes. Diabetes Care 2012; 35: 1126–32.
N Engl J Med 2009; 360: 129–39.
10 www.thelancet.com/diabetes-endocrinology Published online March 26, 2019 http://dx.doi.org/10.1016/S2213-8587(18)30315-2
Review
29 Johnston SS, Conner C, Aagren M, Smith DM, Bouchard J, Brett J. 52 Wright RJ, Newby DE, Stirling D, Ludlam CA, Macdonald IA,
Evidence linking hypoglycemic events to an increased risk of acute Frier BM. Effects of acute insulin-induced hypoglycemia on indices
cardiovascular events in patients with type 2 diabetes. of inflammation: putative mechanism for aggravating vascular
Diabetes Care 2011; 34: 1164–70. disease in diabetes. Diabetes Care 2010; 33: 1591–97.
30 Nunes AP, Iglay K, Radican L, et al. Hypoglycaemia seriousness 53 Adler GK, Bonyhay I, Failing H, Waring E, Dotson S, Freeman R.
and weight gain as determinants of cardiovascular disease Antecedent hypoglycemia impairs autonomic cardiovascular
outcomes among sulfonylurea users. Diabetes Obes Metab 2017; function: implications for rigorous glycemic control. Diabetes 2009;
19: 1425–35. 58: 360–66.
31 Smith L, Chakraborty D, Bhattacharya P, Sarmah D, Koch S, 54 Chow E, Iqbal A, Walkinshaw E, Phoenix F, Macdonald IA,
Dave KR. Exposure to hypoglycemia and risk of stroke. Storey RF, Ajjan R, Heller SR. Prolonged prothrombotic effects of
Ann N Y Acad Sci 2018; 1431: 25–34. antecedent hypoglycemia in individuals with type 2 diabetes.
32 Goto A, Arah OA, Goto M, Terauchi Y, Noda M. Diabetes Care 2018; 41: 2625–33.
Severe hypoglycaemia and cardiovascular disease: systematic review 55 Wright RJ, Frier BM. Vascular disease and diabetes: is hypoglycaemia
and meta-analysis with bias analysis. BMJ 2013; 347: f4533. an aggravating factor? Diabetes Metab Res Rev 2008; 24: 353–63.
33 Yeh JS, Sung SH, Huang HM, et al. Hypoglycemia and risk of 56 Desouza C, Salazar H, Cheong B, Murgo J, Fonseca V.
vascular events and mortality: a systematic review and Association of hypoglycemia and cardiac ischemia: a study based on
meta-analysis. Acta Diabetol 2016; 53: 377–92. continuous monitoring. Diabetes Care 2003; 26: 1485–89.
34 Huang CJ, Wang WT, Sung SH, et al. Blood glucose reduction by 57 Adler GK, Bonyhay I, Curren V, Waring E, Freeman R.
diabetic drugs with minimal hypoglycaemia risk for cardiovascular Hypoglycaemia increases aldosterone in a dose-dependent fashion.
outcomes: evidence from meta-regression analysis of randomized Diabet Med 2010; 27: 1250–55.
controlled trials. Diabetes Obes Metab 2018; 20: 2131–39. 58 Gogitidze Joy N, Hedrington MS, Briscoe VJ, Tate DB, Ertl AC,
35 Müller N, Khunti K, Kuss O, et al. Is there evidence of potential Davis SN. Effects of acute hypoglycemia on inflammatory and
overtreatment of glycaemia in elderly people with type 2 diabetes? pro-atherothrombotic biomarkers in individuals with type 1 diabetes
Data from the GUIDANCE study. Acta Diabetol 2017; 54: 209–14. and healthy individuals. Diabetes Care 2010; 33: 1529–35.
36 de Decker L, Hanon O, Boureau AS, et al. Association between 59 Beall C, Ashford ML, McCrimmon RJ. The physiology and
hypoglycemia and the burden of comorbidities in hospitalized pathophysiology of the neural control of the counterregulatory
vulnerable older diabetic patients: a cross-sectional, response. Am J Physiol Regul Integr Comp Physiol 2012; 302: R215–23.
population-based study. Diabetes Ther 2017; 8: 1405–13. 60 Fritsche A, Stumvoll M, Grüb M, et al. Effect of hypoglycemia on
37 Heald AH, Anderson SG, Cortes GJ, et al. Hypoglycaemia in the beta-adrenergic sensitivity in normal and type 1 diabetic subjects.
over 75s: understanding the predisposing factors in type 2 diabetes Diabetes Care 1998; 21: 1505–10.
(T2DM). Prim Care Diabetes 2018; 12: 133–38. 61 Giménez M, Gilabert R, Monteagudo J, et al. Repeated episodes of
38 Huang ES, Laiteerapong N, Liu JY, John PM, Moffet HH, Karter AJ. hypoglycemia as a potential aggravating factor for preclinical
Rates of complications and mortality in older patients with diabetes atherosclerosis in subjects with type 1 diabetes. Diabetes Care 2011;
mellitus: the Diabetes and Aging Study. JAMA Intern Med 2014; 34: 198–203.
174: 251–58. 62 McNeilly AD, Gallagher JR, Dinkova-Kostova AT, et al.
39 Chi MJ, Liang CK, Lee WJ, Peng LN, Chou MY, Chen LK. Nrf2-mediated neuroprotection against recurrent hypoglycemia is
Association of new-onset diabetes mellitus in older people insufficient to prevent cognitive impairment in a rodent model of
and mortality in Taiwan: a 10-year nationwide population-based type 1 diabetes. Diabetes 2016; 65: 3151–60.
study. J Nutr Health Aging 2017; 21: 227–32. 63 Ratter JM, Rooijackers HM, Tack CJ, et al. Proinflammatory effects
40 Jones TB, Savasan ZA, Johnson Q, Bahado-Singh R. Management of hypoglycemia in humans with or without diabetes. Diabetes 2017;
of pregnant patients with diabetes with ischemic heart disease. 66: 1052–61.
Clin Lab Med 2013; 33: 243–56. 64 Cwikiel J, Seljeflot I, Berge E, Njerve IU, Ulsaker H, Arnesen H,
41 Kimmerle R, Heinemann L, Delecki A, Berger M. Severe Flaa A. Effect of strenuous exercise on mediators of inflammation
hypoglycemia; incidence and predisposing factors in 85 in patients with coronary artery disease. Cytokine 2018; 105: 17–22.
pregnancies of type 1 diabetic women. Diabetes Care 1992; 65 Ceriello A, Novials A, Ortega E, et al. Hyperglycemia following
15: 1034–37. recovery from hypoglycemia worsens endothelial damage and
42 Leinonen PJ, Hiilesmaa VK, Kaaja RJ, Teramo KA. thrombosis activation in type 1 diabetes and in healthy controls.
Maternal mortality in type 1 diabetes. Diabetes Care 2001; Nutr Metab Cardiovasc Dis 2014; 24: 116–23.
24: 1501–02. 66 Reno CM, VanderWeele J, Bayles J, et al. Severe
43 NICE. Diabetes in pregnancy: management from preconception to hypoglycemia-induced fatal cardiac arrhythmias are augmented by
the postnatal period. NICE guideline [NG3]. London: National diabetes and attenuated by recurrent hypoglycemia. Diabetes 2017;
Institute for Health and Care Excellence, 2015. 66: 3091–97.
44 Edge JA, Ford-Adams ME, Dunger DB. Causes of death in children 67 Tattersall RB, Gill GV. Unexplained deaths of type 1 diabetic
with insulin dependent diabetes 1990–96. Arch Dis Child 1999; patients. Diabet Med 1991; 8: 49–58.
81: 318–23. 68 Secrest AM, Becker DJ, Kelsey SF, Laporte RE, Orchard TJ.
45 O’Grady MJ, Delaney J, Jones TW, Davis EA. Standardised mortality Characterizing sudden death and dead-in-bed syndrome in type 1
is increased three-fold in a population-based sample of diabetes: analysis from two childhood-onset type 1 diabetes
children and adolescents with type 1 diabetes. Pediatr Diabetes 2013; registries. Diabet Med 2011; 28: 293–300.
14: 13–17. 69 Tanenberg RJ, Newton CA, Drake AJ. Confirmation of hypoglycemia
46 Desouza CV, Bolli GB, Fonseca V. Hypoglycemia, diabetes, in the “dead-in-bed” syndrome, as captured by a retrospective
and cardiovascular events. Diabetes Care 2010; 33: 1389–94. continuous glucose monitoring system. Endocr Pract 2010; 16: 244–48.
47 Dahlquist G, Källén B. Mortality in childhood-onset type 1 diabetes: 70 Marques JLB, George E, Peacey SR, et al. Altered ventricular
a population-based study. Diabetes Care 2005; 28: 2384–87. repolarization during hypoglycaemia in patients with diabetes.
48 Fisher BM, Gillen G, Hepburn DA, Dargie HJ, Frier BM. Diabet Med 1997; 14: 648–54.
Cardiac responses to acute insulin-induced hypoglycemia in 71 Landstedt-Hallin L, Englund A, Adamson U, Lins PE. Increased QT
humans. Am J Physiol 1990; 258: H1775–79. dispersion during hypoglycaemia in patients with type 2 diabetes
49 Sommerfield AJ, Wilkinson IB, Webb DJ, Frier BM. Vessel wall mellitus. J Intern Med 1999; 246: 299–307.
stiffness in type 1 diabetes and the central hemodynamic effects of 72 Tu E, Bagnall RD, Duflou J, Lynch M, Twigg SM, Semsarian C.
acute hypoglycemia. Am J Physiol Endocrinol Metab 2007; Post-mortem pathologic and genetic studies in “dead in bed
293: E1274–79. syndrome” cases in type 1 diabetes mellitus. Hum Pathol 2010;
50 Petersen KG, Schlüter KJ, Kerp L. Regulation of serum potassium 41: 392–400.
during insulin-induced hypoglycemia. Diabetes 1982; 31: 615–17. 73 Novodvorsky P, Bernjak A, Chow E, et al. Diurnal differences in
51 Frier BM, Schernthaner G, Heller SR. Hypoglycemia and risk of cardiac arrhythmias during spontaneous hypoglycemia in
cardiovascular risks. Diabetes Care 2011; 34 (suppl 2): S132–37. young people with type 1 diabetes. Diabetes Care 2017; 40: 655–62.
www.thelancet.com/diabetes-endocrinology Published online March 26, 2019 http://dx.doi.org/10.1016/S2213-8587(18)30315-2 11
Review
74 Reno CM, Daphna-Iken D, Chen YS, VanderWeele J, Jethi K, 91 Pickup JC, Sutton AJ. Severe hypoglycaemia and glycaemic control
Fisher SJ. Severe hypoglycemia-induced lethal cardiac arrhythmias in type 1 diabetes: meta-analysis of multiple daily insulin injections
are mediated by sympathoadrenal activation. Diabetes 2013; compared with continuous subcutaneous insulin infusion.
62: 3570–81. Diabet Med 2008; 25: 765–74.
75 Chow E, Bernjak A, Williams S, et al. Risk of cardiac arrhythmias 92 Beck RW, Riddlesworth TD, Ruedy K, et al. Continuous glucose
during hypoglycemia in patients with type 2 diabetes monitoring versus usual care in patients with type 2 diabetes
and cardiovascular risk. Diabetes 2014; 63: 1738–47. receiving multiple daily insulin injections: a randomized trial.
76 Chow E, Bernjak A, Walkinshaw E, et al. Cardiac autonomic Ann Intern Med 2017; 167: 365–74.
regulation and repolarization during acute experimental 93 Bergenstal RM, Klonoff DC, Garg SK, et al. Threshold-based
hypoglycemia in type 2 diabetes. Diabetes 2017; 66: 1322–33. insulin-pump interruption for reduction of hypoglycemia.
77 Fisher BM, Gillen G, Dargie HJ, Inglis GC, Frier BM. The effects N Engl J Med 2013; 369: 224–32.
of insulin-induced hypoglycaemia on cardiovascular function in 94 Bergenstal RM, Garg S, Weinzimer SA, et al. Safety of a hybrid
normal man: studies using radionuclide ventriculography. closed-loop insulin delivery system in patients with type 1 diabetes.
Diabetologia 1987; 30: 841–45. JAMA 2016; 316: 1407–08.
78 Rao AD, Bonyhay I, Dankwa J, et al. Baroreflex sensitivity 95 Rickels MR, Peleckis AJ, Markmann E, et al. Long-term
impairment during hypoglycemia: implications for cardiovascular improvement in glucose control and counterregulation by islet
control. Diabetes 2016; 65: 209–15. transplantation for type 1 diabetes. J Clin Endocrinol Metab 2016;
79 Hendrieckx C, Halliday JA, Bowden JP, et al. Severe hypoglycaemia 101: 4421–30.
and its association with psychological well-being in Australian 96 American Diabetes Association. American Diabetes Association 6:
adults with type 1 diabetes attending specialist tertiary clinics. glycemic targets: standards of medical care in diabetes—2019.
Diabetes Res Clin Pract 2014; 103: 430–36. Diabetes Care 2019; 42 (suppl 1): S61–70.
80 Evans M, Khunti K, Mamdani M, et al. Health-related quality of life 97 Lowe G, Woodward M, Hillis G, et al. Circulating inflammatory
associated with daytime and nocturnal hypoglycaemic events: markers and the risk of vascular complications and mortality in
a time trade-off survey in five countries. Health Qual Life Outcomes people with type 2 diabetes and cardiovascular disease or risk
2013; 11: 90. factors: the ADVANCE study. Diabetes 2014; 63: 1115–23.
81 Anderbro T, Gonder-Frederick L, Bolinder J, et al. Fear of 98 Keating ST, van Diepen JA, Riksen NP, El-Osta A. Epigenetics in
hypoglycemia: relationship to hypoglycemic risk and psychological diabetic nephropathy, immunity and metabolism. Diabetologia 2018;
factors. Acta Diabetol 2015; 52: 581–89. 61: 6–20.
82 Gonder-Frederick L, Nyer M, Shepard JA, Vajda K, Clarke W. 99 Rooijackers HM, Wiegers EC, Tack CJ, van der Graaf M,
Assessing fear of hypoglycemia in children with type 1 diabetes de Galan BE. Brain glucose metabolism during hypoglycemia in
and their parents. Diabetes Manag (Lond) 2011; 1: 627–39. type 1 diabetes: insights from functional and metabolic
83 Driscoll KA, Raymond J, Naranjo D, Patton SR. Fear of neuroimaging studies. Cell Mol Life Sci 2016; 73: 705–22.
hypoglycemia in children and adolescents and their parents 100 Joy NG, Tate DB, Younk LM, Davis SN. Effects of acute and
with type 1 diabetes. Curr Diab Rep 2016; 16: 77. antecedent hypoglycemia on endothelial function and markers of
84 Gonder-Frederick LA, Vajda KA, Schmidt KM, et al. Examining atherothrombotic balance in healthy humans. Diabetes 2015;
the behaviour subscale of the Hypoglycaemia Fear Survey: 64: 2571–80.
an international study. Diabet Med 2013; 30: 603–09. 101 Reno CM, Tanoli T, Bree A, et al. Antecedent glycemic control
85 Barnard K, Thomas S, Royle P, Noyes K, Waugh N. Fear of reduces severe hypoglycemia-induced neuronal damage in diabetic
hypoglycaemia in parents of young children with type 1 diabetes: rats. Am J Physiol Endocrinol Metab 2013; 304: E1331–37.
a systematic review. BMC Pediatr 2010; 10: 50. 102 Puente EC, Silverstein J, Bree AJ, et al. Recurrent moderate
86 International Hypoglycaemia Study Group. Understanding hypoglycemia ameliorates brain damage and cognitive dysfunction
hypoglycaemia. https://ihsgonline.com/resources (accessed Feb 21, induced by severe hypoglycemia. Diabetes 2010; 59: 1055–62.
2019). 103 Milani-Nejad N, Janssen PM. Small and large animal models in
87 Yeoh E, Choudhary P, Nwokolo M, Ayis S, Amiel SA. Interventions cardiac contraction research: advantages and disadvantages.
that restore awareness of hypoglycemia in adults with type 1 Pharmacol Ther 2014; 141: 235–49.
diabetes: a systematic review and meta-analysis. Diabetes Care 2015; 104 Campbell M, Heller SR, Jacques RM. Response to Comment on
38: 1592–609. Novodvorsky et al. Diurnal differences in risk of cardiac
88 Lane W, Bailey TS, Gerety G, et al. Effect of insulin degludec vs arrhythmias during spontaneous hypoglycemia in young people
insulin glargine U100 on hypoglycemia in patients with type 1 with type 1 diabetes. Diabetes Care 2017; 40: 655–662.
diabetes: the SWITCH 1 randomized clinical trial. JAMA 2017; 105 Currie CJ, Peters JR, Tynan A, et al. Survival as a function of HbA1c
318: 33–44. in people with type 2 diabetes: a retrospective cohort study. Lancet
89 Wysham C, Bhargava A, Chaykin L, et al. Effect of insulin degludec 2010; 375: 481–89.
vs insulin glargine U100 on hypoglycemia in patients with type 2
diabetes: the SWITCH 2 randomized clinical trial. JAMA 2017; © 2019 Elsevier Ltd. All rights reserved.
318: 45–56.
90 Marso SP, McGuire DK, Zinman B, et al. Efficacy and safety of
degludec versus glargine in type 2 diabetes. N Engl J Med 2017;
377: 723–32.
12 www.thelancet.com/diabetes-endocrinology Published online March 26, 2019 http://dx.doi.org/10.1016/S2213-8587(18)30315-2
You might also like
- Artigo Citado Dizendo Que Hiperglicemia Posprandial Sendo Um Preditor Melhor Qe Hemoglobina GlicadaDocument7 pagesArtigo Citado Dizendo Que Hiperglicemia Posprandial Sendo Um Preditor Melhor Qe Hemoglobina GlicadabonelockNo ratings yet
- Diabetes, Glucose Level, and Risk of Sudden Cardiac DeathDocument6 pagesDiabetes, Glucose Level, and Risk of Sudden Cardiac DeathDino DanielNo ratings yet
- Asssociation of Glycaemia With Macrovascular and Microvascular ComplicationsDocument8 pagesAsssociation of Glycaemia With Macrovascular and Microvascular ComplicationsMartha CoradoNo ratings yet
- Ijms 24 09357 v2Document14 pagesIjms 24 09357 v2MSNo ratings yet
- Perspectives in Diabetes: Postprandial Hyperglycemia and Diabetes ComplicationsDocument7 pagesPerspectives in Diabetes: Postprandial Hyperglycemia and Diabetes ComplicationsHania Asmarani RahmanitaNo ratings yet
- Diabetes 5Document16 pagesDiabetes 5patricia osei-owusuNo ratings yet
- Hypoglycemia, Diabetes, and Cardiovascular Events: C V. D, G B. B, V FDocument6 pagesHypoglycemia, Diabetes, and Cardiovascular Events: C V. D, G B. B, V FHervi LaksariNo ratings yet
- PP Lancet 1998 Ukpds33Document17 pagesPP Lancet 1998 Ukpds33HelloNo ratings yet
- ADO in BRCDocument10 pagesADO in BRCVlahtNo ratings yet
- Oxidative Stress and Diabetic Vascular ComplicationsDocument11 pagesOxidative Stress and Diabetic Vascular ComplicationsMatias PrietoNo ratings yet
- Diabetes and Cvs DiseaseDocument8 pagesDiabetes and Cvs DiseaseZaraNo ratings yet
- Pathogenesisof Cardiovasculardiseasein Diabetes: Andrea V. Haas,, Marie E. McdonnellDocument13 pagesPathogenesisof Cardiovasculardiseasein Diabetes: Andrea V. Haas,, Marie E. McdonnellPaulina DiazNo ratings yet
- UKPDS Study Shows Benefits of Lowering Blood Glucose and Blood Pressure in Type 2 DiabetesDocument5 pagesUKPDS Study Shows Benefits of Lowering Blood Glucose and Blood Pressure in Type 2 DiabetesAgustin MendezNo ratings yet
- Hypoglycemia in Diabetes: P E. C, S N. D, H SDocument11 pagesHypoglycemia in Diabetes: P E. C, S N. D, H SFabio FabbriNo ratings yet
- Hypoglycemia - The Neglected ComplicationDocument23 pagesHypoglycemia - The Neglected Complication4g5xwdvh9sNo ratings yet
- Exposure To Hypoglycemia and Risk of StrokeDocument15 pagesExposure To Hypoglycemia and Risk of StrokeNurvia AndrianiNo ratings yet
- 20200800.0-00029 Preoperative GlucosaDocument9 pages20200800.0-00029 Preoperative GlucosaLuis OrdóñezNo ratings yet
- Haffner Am J Med 2003Document6 pagesHaffner Am J Med 2003slavenNo ratings yet
- Can Hypoglicemic EpisodesDocument6 pagesCan Hypoglicemic EpisodesRizki NovNo ratings yet
- Nihms 1840957Document35 pagesNihms 1840957Melda AngleNo ratings yet
- Cerebral Ischemic Damage in Diabetes: An Inflammatory PerspectiveDocument22 pagesCerebral Ischemic Damage in Diabetes: An Inflammatory PerspectiveAnonymous QPakSNNo ratings yet
- Journal ReadingDocument7 pagesJournal Readingdr AnnisaNo ratings yet
- Dysglycemiaandglucose Controlduringsepsis: Mark P. Plummer,, Adam M. DeaneDocument11 pagesDysglycemiaandglucose Controlduringsepsis: Mark P. Plummer,, Adam M. DeanePaul GuijarroNo ratings yet
- Control GlicemicoDocument20 pagesControl GlicemicomiguelalmenarezNo ratings yet
- Hypoglycemia - 2014 Morales N DoronDocument8 pagesHypoglycemia - 2014 Morales N DoronDian Eka RamadhaniNo ratings yet
- Prevalence of Diabetes and Its Effects On Stroke Outcomes: A Meta-Analysis and Literature ReviewDocument13 pagesPrevalence of Diabetes and Its Effects On Stroke Outcomes: A Meta-Analysis and Literature ReviewarinyNo ratings yet
- 2016 - Potential Drug Combinations To Reduce Cardiovascular Disease Burden in DiabetesDocument13 pages2016 - Potential Drug Combinations To Reduce Cardiovascular Disease Burden in DiabetesWENDY JOHANA HENRIQUEZ SEGURA ESTUDIANTE ACTIVONo ratings yet
- 1 s2.0 S000291491730807X MainDocument11 pages1 s2.0 S000291491730807X MainEndru AngelNo ratings yet
- Jurnal Hipoglikemia 1Document11 pagesJurnal Hipoglikemia 1dimas gilang prakosoNo ratings yet
- The Pathological Effects of Hyperglycaemia On The Cardiovascular (CV) System and BrainDocument5 pagesThe Pathological Effects of Hyperglycaemia On The Cardiovascular (CV) System and BrainRyzka Izza MayFanyNo ratings yet
- CroatMedJ 56 0181Document13 pagesCroatMedJ 56 0181Aditya ArthaNo ratings yet
- Up-Date On Diabetic NephropathyDocument17 pagesUp-Date On Diabetic NephropathykvyNo ratings yet
- ADA Scientific 2000Document6 pagesADA Scientific 2000Rahmah Gadis Wartania PutriNo ratings yet
- ADVANCE: Action in Diabetes and Vascular Disease: Original ArticleDocument6 pagesADVANCE: Action in Diabetes and Vascular Disease: Original ArticleMade LascanoNo ratings yet
- Eid2019 Article NewInsightsIntoTheMechanismsOf PDFDocument11 pagesEid2019 Article NewInsightsIntoTheMechanismsOf PDFStella UrdinolaNo ratings yet
- ADA - UKPD StudyDocument5 pagesADA - UKPD StudyMagdalena MercyanaNo ratings yet
- HHS Public Access: Diabetes and Stroke: Epidemiology, Pathophysiology, Pharmaceuticals and OutcomesDocument13 pagesHHS Public Access: Diabetes and Stroke: Epidemiology, Pathophysiology, Pharmaceuticals and OutcomesayuNo ratings yet
- 77 FullDocument6 pages77 FullRizkaNNatsirNo ratings yet
- Diabetes Mellitus: Anaesthetic Management : ReviewarticleDocument4 pagesDiabetes Mellitus: Anaesthetic Management : Reviewarticledrdion mangku alamNo ratings yet
- Elisa Dal Canto 2019Document8 pagesElisa Dal Canto 2019Nikola Dragicka DragicevicNo ratings yet
- Original Article: Hyperglycemia Stimulates Coagulation, Whereas Hyperinsulinemia Impairs Fibrinolysis in Healthy HumansDocument6 pagesOriginal Article: Hyperglycemia Stimulates Coagulation, Whereas Hyperinsulinemia Impairs Fibrinolysis in Healthy Humansfamie_zzNo ratings yet
- Hypoglycemia: Table 1Document8 pagesHypoglycemia: Table 1erik1585No ratings yet
- Hypoglycemia in DiabetesDocument12 pagesHypoglycemia in Diabetesnaili mumtazatiNo ratings yet
- Evaluation of Urinary 8-Hydroxydeoxy-Guanosine As A Novel Biomarker of Macrovascular Complications in Type 2 DiabetesDocument6 pagesEvaluation of Urinary 8-Hydroxydeoxy-Guanosine As A Novel Biomarker of Macrovascular Complications in Type 2 DiabetesTomNo ratings yet
- Fatores Risco Cetoacidose em Pacientes Tipo 1Document9 pagesFatores Risco Cetoacidose em Pacientes Tipo 1miguelfilipegralhaalmeidaNo ratings yet
- 1 s2.0 S1877593409000575 Main PDFDocument5 pages1 s2.0 S1877593409000575 Main PDFTiya HilmawanNo ratings yet
- The UK Prospective Diabetes Study (UKPDS) : Clinical and Therapeutic Implications For Type 2 DiabetesDocument6 pagesThe UK Prospective Diabetes Study (UKPDS) : Clinical and Therapeutic Implications For Type 2 DiabetesLaila KurniaNo ratings yet
- Coutinho 1999Document8 pagesCoutinho 1999DR VENKATARAMANA MurthyNo ratings yet
- Hypoglycemia in Patients With Insulin Treated Diabetes: Review ArticleDocument9 pagesHypoglycemia in Patients With Insulin Treated Diabetes: Review ArticleEmanuel BaltigNo ratings yet
- The Role of Glycemic Variability in Cardiovascular DisordersDocument15 pagesThe Role of Glycemic Variability in Cardiovascular DisordersNinaRicaR.RamosNo ratings yet
- UKPDSDocument39 pagesUKPDSIsaac TellezNo ratings yet
- Diabetes Obesity Metabolism - 2019 - Ghouse - Effect of Diabetes Duration On The Relationship Between Glycaemic Control andDocument12 pagesDiabetes Obesity Metabolism - 2019 - Ghouse - Effect of Diabetes Duration On The Relationship Between Glycaemic Control androbert mbwamboNo ratings yet
- Heart Failure and Diabetes Endo Metab Clinics North Am 17Document19 pagesHeart Failure and Diabetes Endo Metab Clinics North Am 17Paulina DiazNo ratings yet
- Hyperglycemic CrisisDocument9 pagesHyperglycemic CrisisRoberto López MataNo ratings yet
- Hyperglycaemic EmergenciesDocument11 pagesHyperglycaemic EmergenciesdramaysinghNo ratings yet
- Best Practice & Research Clinical Endocrinology & MetabolismDocument12 pagesBest Practice & Research Clinical Endocrinology & MetabolismMarnia SulfianaNo ratings yet
- Polypharmacy in The Aging Patient A Review of Glycemic Control in Older Adults With Type 2 DiabetesDocument12 pagesPolypharmacy in The Aging Patient A Review of Glycemic Control in Older Adults With Type 2 Diabetesapi-311409998No ratings yet
- Emerging Role of Dipeptidyl Peptidase-IV (DPP-4) Inhibitor Vildagliptin in The Management of Type 2 DiabetesDocument9 pagesEmerging Role of Dipeptidyl Peptidase-IV (DPP-4) Inhibitor Vildagliptin in The Management of Type 2 DiabetesIndrasuari Anak Agung AyuNo ratings yet
- Effects of Type 2 Diabetes Upon Cardiovascular Diseases: Nimesha Gunathilaka, Bhagya ManjareeDocument8 pagesEffects of Type 2 Diabetes Upon Cardiovascular Diseases: Nimesha Gunathilaka, Bhagya ManjareeMarchelino ChristianNo ratings yet
- Differences in Left Ventricular and Left Atrial FuDocument10 pagesDifferences in Left Ventricular and Left Atrial FueugeniaNo ratings yet
- Detailed Lesson Plan in General MathematicsDocument6 pagesDetailed Lesson Plan in General MathematicsAira Jane Irarum78% (18)
- Brochure - 2018 - Hitfact Mkii 2Document2 pagesBrochure - 2018 - Hitfact Mkii 2diaa ahmedNo ratings yet
- FIKE RD Combo With Relief ValvesDocument11 pagesFIKE RD Combo With Relief ValvesAnkit GandhiNo ratings yet
- Collaboration Processes: Looking Inside the Black BoxDocument13 pagesCollaboration Processes: Looking Inside the Black Boxเข้าใจว่า น่าจะชื่อตุ้นNo ratings yet
- 11 Physics Test Paper Ch3 1Document4 pages11 Physics Test Paper Ch3 1Devendar SharmaNo ratings yet
- Gem EscortingDocument7 pagesGem Escortingsuman sutharNo ratings yet
- SR. NO. Capacity/Descirption of Machine Client: A.C. Generator StatorsDocument5 pagesSR. NO. Capacity/Descirption of Machine Client: A.C. Generator Statorsmtj4uNo ratings yet
- QRP Yu1lm SDR-RX TXDocument299 pagesQRP Yu1lm SDR-RX TXD BNo ratings yet
- z1875 Caton (BMJ) Electric Currents of The BrainDocument23 pagesz1875 Caton (BMJ) Electric Currents of The BrainUnholy VladNo ratings yet
- Girbau STI-54 STI-77 Parts ManualDocument74 pagesGirbau STI-54 STI-77 Parts Manualrpm14sheratonbsasNo ratings yet
- 2a CTRL DecDocument75 pages2a CTRL Decramanathan balamoorthyNo ratings yet
- Communications in Algebra: On The U-Invariant of P-Adic Function FieldsDocument9 pagesCommunications in Algebra: On The U-Invariant of P-Adic Function FieldsKarim ZahidiNo ratings yet
- Shock Classification and PathophysiologyDocument40 pagesShock Classification and PathophysiologyErick Anca100% (2)
- Essay - DnaDocument2 pagesEssay - Dnaapi-243852896No ratings yet
- RCS England Trainees Guide To A Quality Improvement Project 2021Document17 pagesRCS England Trainees Guide To A Quality Improvement Project 2021Wee K WeiNo ratings yet
- Image Forgery DetectionDocument17 pagesImage Forgery DetectionanlemacoNo ratings yet
- S2 Papers FinalizedDocument149 pagesS2 Papers FinalizedRaffles HolmesNo ratings yet
- When Ceramic Sociology Meets Material SCDocument10 pagesWhen Ceramic Sociology Meets Material SCJosé Renato TeixeiraNo ratings yet
- Yanmar Mechnical PumpDocument16 pagesYanmar Mechnical Pump송성훈100% (9)
- Shivag Itim Al ADocument27 pagesShivag Itim Al AKellie RamosNo ratings yet
- Memorial Garden Policies and Guidelines St. Mark's Episcopal Church, Raleigh, North CarolinaDocument7 pagesMemorial Garden Policies and Guidelines St. Mark's Episcopal Church, Raleigh, North Carolinaestela maria dulaganNo ratings yet
- Computations on a waiters bill pad and conversations in the mistDocument3 pagesComputations on a waiters bill pad and conversations in the mistRavishu NagarwalNo ratings yet
- My Version of Meatlaof Project DraftDocument3 pagesMy Version of Meatlaof Project DraftCloue Faye I. BasalloNo ratings yet
- Sample Article Used by MeDocument14 pagesSample Article Used by MeMagnum OpusNo ratings yet
- Eutelsat 12 West A Satellite FootprintDocument2 pagesEutelsat 12 West A Satellite FootprintSkybrokersNo ratings yet
- Popular CultureDocument25 pagesPopular CultureVibhuti KachhapNo ratings yet
- MFJ-854 RF MeterDocument5 pagesMFJ-854 RF MeterHappyJoeNo ratings yet
- Philips HF C-Arm BrochureDocument2 pagesPhilips HF C-Arm Brochuregarysov50% (2)
- Hellstorm NotesDocument57 pagesHellstorm NotesDeni ZenNo ratings yet