You might also like
- Guidelines CIDPDocument9 pagesGuidelines CIDPTowhidulIslamNo ratings yet
- CIDP Guideline EJoN 2021Document29 pagesCIDP Guideline EJoN 2021FlowerNo ratings yet
- J Peripheral Nervous Sys - 2021 - Van Den Bergh - European Academy of Neurology Peripheral Nerve Society Guideline OnDocument27 pagesJ Peripheral Nervous Sys - 2021 - Van Den Bergh - European Academy of Neurology Peripheral Nerve Society Guideline OngkcNo ratings yet
- Euro J of Neurology - 2021 - Van Den Bergh - European Academy of Neurology Peripheral Nerve Society Guideline On DiagnosisDocument28 pagesEuro J of Neurology - 2021 - Van Den Bergh - European Academy of Neurology Peripheral Nerve Society Guideline On DiagnosisSusana RocheNo ratings yet
- NEUROLOGY2014621771Document13 pagesNEUROLOGY2014621771Alexandra SerbanNo ratings yet
- Chronic Inflammatory Demyelinating PolyradiculoneuropathyDocument5 pagesChronic Inflammatory Demyelinating PolyradiculoneuropathyDra Carolina Escalante Neurologa de AdultosNo ratings yet
- Tugas AkupunturDocument16 pagesTugas AkupunturHafid Adi NugrohoNo ratings yet
- Medsci 11 00015 v2Document34 pagesMedsci 11 00015 v2Paulina Sobarzo VegaNo ratings yet
- ADNIannualchangebiomarkers clinicaloutcomeA&D10Document8 pagesADNIannualchangebiomarkers clinicaloutcomeA&D10brunoabramoffNo ratings yet
- VejezDocument7 pagesVejezPamelaNo ratings yet
- EFNS Guideline 2010 Diagnosis and Management of ADDocument13 pagesEFNS Guideline 2010 Diagnosis and Management of ADDeni Andre AtmadinataNo ratings yet
- Diagnóstico CIDPDocument7 pagesDiagnóstico CIDPMarysol UlloaNo ratings yet
- Idsa NeurocisticercosisDocument27 pagesIdsa Neurocisticercosistucto849915No ratings yet
- Goldstein 2010Document10 pagesGoldstein 2010esckere papas fritasNo ratings yet
- Best Practice in Primary Care Pathology: Review 1Document10 pagesBest Practice in Primary Care Pathology: Review 1Sisca PrimaNo ratings yet
- UlnarNeur ReaffirmedDocument33 pagesUlnarNeur ReaffirmedEstefania ChaponNo ratings yet
- Medicine: The Effectiveness and Safety of Electroacupuncture For Nonspecific Chronic Low Back PainDocument4 pagesMedicine: The Effectiveness and Safety of Electroacupuncture For Nonspecific Chronic Low Back PainMohammad Rafi NampiraNo ratings yet
- ECAM2013 Trat FMSDocument7 pagesECAM2013 Trat FMStxankleroNo ratings yet
- 2019 EULAR SLE CriteriaDocument27 pages2019 EULAR SLE CriteriaLily ChandraNo ratings yet
- Medi 101 E29150 2 PDFDocument5 pagesMedi 101 E29150 2 PDFSam SamNo ratings yet
- Compression of The Fourth Ventricle Using A Craniosacral Osteopathic ...Document9 pagesCompression of The Fourth Ventricle Using A Craniosacral Osteopathic ...AlexNo ratings yet
- Diagnosis and Treatment For MildDocument12 pagesDiagnosis and Treatment For MildJorge SalazarNo ratings yet
- Clinical Practice Guidelines For Nursing - and HealDocument24 pagesClinical Practice Guidelines For Nursing - and HealHAMNA ZAINABNo ratings yet
- Martino, D. (2023) - Treatment Failure in Persisten Tic Disorders...Document15 pagesMartino, D. (2023) - Treatment Failure in Persisten Tic Disorders...cuautzinNo ratings yet
- Chronic Inflammatory Demyelinating PolyneuropathyDocument7 pagesChronic Inflammatory Demyelinating PolyneuropathyApriliaNo ratings yet
- Screenshot 2024-02-20 at 23.03.52Document6 pagesScreenshot 2024-02-20 at 23.03.52qory fitrahtulNo ratings yet
- Diagnostic HydrocephalDocument5 pagesDiagnostic HydrocephalTiffany NurzamanNo ratings yet
- JCPT 46 585Document14 pagesJCPT 46 585Syam ChandrasekharanNo ratings yet
- Managamnet ViralDocument14 pagesManagamnet ViralAbd Halim Gazali HNo ratings yet
- MDS Clinical Diagnostic Criteria For Parkinson's Disease: ReviewDocument9 pagesMDS Clinical Diagnostic Criteria For Parkinson's Disease: ReviewFilis MsfNo ratings yet
- 2012-European Journal of Neurology IMPRIMIR PAGINA 141Document368 pages2012-European Journal of Neurology IMPRIMIR PAGINA 141Francisco A. Villegas-LópezNo ratings yet
- The American College of Rheumatology Nomenclature and Case Definitions For Neuropsychiatric Lupus SyndromesDocument10 pagesThe American College of Rheumatology Nomenclature and Case Definitions For Neuropsychiatric Lupus SyndromesThálita Dos AnjosNo ratings yet
- Efficacy and Safety of Electroacupuncture For Post Stroke Depression: Study Protocol For A Randomized Controlled TrialDocument8 pagesEfficacy and Safety of Electroacupuncture For Post Stroke Depression: Study Protocol For A Randomized Controlled TrialwindapuspitasalimNo ratings yet
- Practice Parameters For Using Polysomnography To Evaluate Insomnia: An UpdateDocument7 pagesPractice Parameters For Using Polysomnography To Evaluate Insomnia: An UpdateSamsung UserNo ratings yet
- Steiner2010 PDFDocument14 pagesSteiner2010 PDFLilisNo ratings yet
- Trauma La NastereDocument10 pagesTrauma La NastereMarius AndreiNo ratings yet
- Tratament CushingDocument25 pagesTratament CushingAndreea VladanNo ratings yet
- A Meta-Analysis On Progressive Atrophy in Intractable Temporal Lobe EpilepsyDocument12 pagesA Meta-Analysis On Progressive Atrophy in Intractable Temporal Lobe EpilepsyBeny RiliantoNo ratings yet
- Pulsed Radiofrequency ofDocument8 pagesPulsed Radiofrequency ofDiego Pinto PatroniNo ratings yet
- Z Al-Roubaie_2020Document12 pagesZ Al-Roubaie_2020Kossay ZaouiNo ratings yet
- Acupuncture in the Treatment of Abnormal Muscle Tone in Children With Cerebral Palsy: A Meta-AnalysisDocument11 pagesAcupuncture in the Treatment of Abnormal Muscle Tone in Children With Cerebral Palsy: A Meta-AnalysisrezteevicNo ratings yet
- Translet cts1Document5 pagesTranslet cts1HasvianNo ratings yet
- Alzheimers Disease Diagnosis Using Misfolding ProDocument18 pagesAlzheimers Disease Diagnosis Using Misfolding ProRoberta Lessa RibeiroNo ratings yet
- Diagnostic Criteria For Idiopathic Pulmonary FibrosisDocument16 pagesDiagnostic Criteria For Idiopathic Pulmonary FibrosisHuyen NguyenNo ratings yet
- Considerations For Development of Therapies For Cutaneous NeurofibromaDocument11 pagesConsiderations For Development of Therapies For Cutaneous NeurofibromanadilaayukarisaNo ratings yet
- Practice Parameter: Evaluation of Distal Symmetric Polyneuropathy: Role of Laboratory, Genetic, and Autonomic Testing Nerve Biopsy and Skin Biopsy (An Evidence-Based Review)Document59 pagesPractice Parameter: Evaluation of Distal Symmetric Polyneuropathy: Role of Laboratory, Genetic, and Autonomic Testing Nerve Biopsy and Skin Biopsy (An Evidence-Based Review)M Isyhaduul IslamNo ratings yet
- Clinical Neurology and Neurosurgery: Xuemei Zhang, Siheng Lian, Yingshi Zhang, Qingchun ZhaoDocument8 pagesClinical Neurology and Neurosurgery: Xuemei Zhang, Siheng Lian, Yingshi Zhang, Qingchun ZhaoLi LianNo ratings yet
- HypertensiDocument7 pagesHypertensizazaNo ratings yet
- Systematic Literature Review of Schizophrenia Clinical Practice Guidelines On Acute and Maintenance Management With AntipsychoticsDocument10 pagesSystematic Literature Review of Schizophrenia Clinical Practice Guidelines On Acute and Maintenance Management With AntipsychoticsaqsakhanaljedeelNo ratings yet
- Bloque - 4 - DCB CriteriosDocument7 pagesBloque - 4 - DCB CriteriosMacarena RodriguezNo ratings yet
- Score Predictivo NMDA 2018Document10 pagesScore Predictivo NMDA 2018Pablo Sebastián SaezNo ratings yet
- Ijms 22 02761Document12 pagesIjms 22 02761Juberiya AjazNo ratings yet
- Epilepsy Duration and Seizure Outcome in Epilepsy Surgery: A Systematic Review and Meta-AnalysisDocument9 pagesEpilepsy Duration and Seizure Outcome in Epilepsy Surgery: A Systematic Review and Meta-Analysisbaba ababNo ratings yet
- Essai contrôlé randomisé de la maladie de ParkinsonDocument10 pagesEssai contrôlé randomisé de la maladie de Parkinsonlorit1988No ratings yet
- Researching Revised Diagnostic Criteria for Alzheimer's DiseaseDocument13 pagesResearching Revised Diagnostic Criteria for Alzheimer's DiseaseRegistro psiNo ratings yet
- Jack 2011Document6 pagesJack 2011chiquitaputriNo ratings yet
- N ClassDocument7 pagesN ClassCarlos CENo ratings yet
- Anti NMDAR Update Dalmou 2019Document13 pagesAnti NMDAR Update Dalmou 2019Nathaly LapoNo ratings yet
- West Tto 2Document10 pagesWest Tto 2Nathaly LapoNo ratings yet
- West TtoDocument3 pagesWest TtoNathaly LapoNo ratings yet
- Wjem12 1p0067 PDFDocument10 pagesWjem12 1p0067 PDFAkbal Nur KarimNo ratings yet
- Animal in The BrainDocument10 pagesAnimal in The BrainNathaly LapoNo ratings yet
- Antipsychotic Medication ReferenceDocument7 pagesAntipsychotic Medication ReferenceLiridona ImeriNo ratings yet
- Vertigo and Dizziness in ChildrenDocument11 pagesVertigo and Dizziness in ChildrenNathaly LapoNo ratings yet
- Yic AanDocument7 pagesYic AanNathaly LapoNo ratings yet
- VincrisDocument11 pagesVincrisNathaly LapoNo ratings yet
- Vander KN Aap 2019Document11 pagesVander KN Aap 2019Nathaly LapoNo ratings yet
- Benign Paroxysmal Migraine Variants of Infancy and Childhood: Transitions and Clinical FeaturesDocument7 pagesBenign Paroxysmal Migraine Variants of Infancy and Childhood: Transitions and Clinical FeaturesNathaly LapoNo ratings yet
- Management of Childhood Seizure in Pediatric Emergency Department 237 PDFDocument4 pagesManagement of Childhood Seizure in Pediatric Emergency Department 237 PDFRaul VillacresNo ratings yet
- Twilt-Benseler2015 Article TreatmentOfCNSVasculitisInChilDocument16 pagesTwilt-Benseler2015 Article TreatmentOfCNSVasculitisInChilNathaly LapoNo ratings yet
- Noninfectious Cerebral Vasculitis in Children: Indianapolis, IndianaDocument15 pagesNoninfectious Cerebral Vasculitis in Children: Indianapolis, IndianaNathaly LapoNo ratings yet
- Arterial Ischemic Stroke in Children and Young Adults: Review ArticleDocument23 pagesArterial Ischemic Stroke in Children and Young Adults: Review ArticleNathaly LapoNo ratings yet
- Clinical Guideline: Management of The First Unprovoked Epileptic Seizure in Adults and ChildrenDocument6 pagesClinical Guideline: Management of The First Unprovoked Epileptic Seizure in Adults and Childrennaili nsnNo ratings yet
- West Tto 2Document10 pagesWest Tto 2Nathaly LapoNo ratings yet
- West TtoDocument3 pagesWest TtoNathaly LapoNo ratings yet
- Wjem12 1p0067 PDFDocument10 pagesWjem12 1p0067 PDFAkbal Nur KarimNo ratings yet
- General Biology 1 - Power Point Presentation (Group 8)Document14 pagesGeneral Biology 1 - Power Point Presentation (Group 8)Archan Dom ReyesNo ratings yet
- A Toxicity Study of Methanolic Extract of Calliandra Surinamensis Seeds On Liver Functions in RodentsDocument9 pagesA Toxicity Study of Methanolic Extract of Calliandra Surinamensis Seeds On Liver Functions in RodentsMediterr J Pharm Pharm SciNo ratings yet
- Water Hammer PDFDocument30 pagesWater Hammer PDFbhavesh shuklaNo ratings yet
- Dahong PalayDocument2 pagesDahong PalayAngela MontenegroNo ratings yet
- Rocket Motor Head-end Structural AnalysisDocument83 pagesRocket Motor Head-end Structural AnalysisRudra Sai SandeepNo ratings yet
- SEN Code of Practice 2001Document148 pagesSEN Code of Practice 2001Matt GrantNo ratings yet
- Physics Investigatory Project Class 12Document12 pagesPhysics Investigatory Project Class 12shivanginirai7No ratings yet
- Administrative Case ResolutionDocument2 pagesAdministrative Case ResolutionEunice Osam RamirezNo ratings yet
- RV Failure: Pathophysiology, Diagnosis and TreatmentDocument16 pagesRV Failure: Pathophysiology, Diagnosis and TreatmentRizky Regia TriseynesyaNo ratings yet
- Early Years and Childcare Safeguarding AuditDocument4 pagesEarly Years and Childcare Safeguarding AuditEarly Years Careers100% (1)
- GRADES 1 To 12 Daily Lesson LogDocument5 pagesGRADES 1 To 12 Daily Lesson LogFlordeliza Manaois RamosNo ratings yet
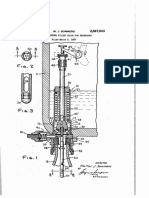
- Counter-pressure filler valve for beveragesDocument3 pagesCounter-pressure filler valve for beveragesbimalishaNo ratings yet
- Chery Amulet 1,6 Engine Service ManualDocument76 pagesChery Amulet 1,6 Engine Service ManualG x HxhNo ratings yet
- Wheat Sourdough Fermentation - Effects of Time and Acidification On Fundamental Rheological PropertiesDocument9 pagesWheat Sourdough Fermentation - Effects of Time and Acidification On Fundamental Rheological PropertiesmaurodiloretoNo ratings yet
- The Role of Technology in AgricultureDocument35 pagesThe Role of Technology in AgricultureDivyesh ThumarNo ratings yet
- Modified Pfirrmann Grading System For Lumbar Intervertebral Disc DegenerationDocument6 pagesModified Pfirrmann Grading System For Lumbar Intervertebral Disc DegenerationZack StylesNo ratings yet
- Candidates applied for Medical Officer post on contract basisDocument11 pagesCandidates applied for Medical Officer post on contract basiszephyrNo ratings yet
- Manoshe Street Takeaway MenuDocument9 pagesManoshe Street Takeaway MenuimaddakrNo ratings yet
- Shandong Lingong Wheel Loader LG956l Operation & Maintenance Manual Final 10.3.23Document130 pagesShandong Lingong Wheel Loader LG956l Operation & Maintenance Manual Final 10.3.23mliugong94% (16)
- Inside Out or Outside In. Meeting With Couples. Hugh JenkinsDocument24 pagesInside Out or Outside In. Meeting With Couples. Hugh JenkinsRita1976No ratings yet
- Operator Manual For Respons920 With ISE - v2016.02Document358 pagesOperator Manual For Respons920 With ISE - v2016.02Juan Pablo CondoriNo ratings yet
- Micro Bio Disease ListDocument168 pagesMicro Bio Disease Listspiff spacemanNo ratings yet
- Starbucks BSC Project Analyzes Store PerformanceDocument8 pagesStarbucks BSC Project Analyzes Store Performanceandrea100% (1)
- Mitsubishi Galant 4g63 Engine Repair ManualDocument29 pagesMitsubishi Galant 4g63 Engine Repair ManualMoaed Kanbar100% (1)
- CSC 101-CSC 111 - Introduction To Computer Science - Lecture 1Document23 pagesCSC 101-CSC 111 - Introduction To Computer Science - Lecture 1CODE100% (1)
- How To Judge A Dasha in JyotishDocument2 pagesHow To Judge A Dasha in JyotishRavan SharmaNo ratings yet
- Fuente As-IDocument4 pagesFuente As-IadalaviNo ratings yet
- Spares Parts Cannibalisation ProcedureDocument3 pagesSpares Parts Cannibalisation ProcedureThang Nguyen Hung100% (1)
- Public Health EngineeringDocument10 pagesPublic Health EngineeringOmkar DeshpandeNo ratings yet
- Make Every Day Count: George Eliot's inspirational poemDocument3 pagesMake Every Day Count: George Eliot's inspirational poemRUTUJA KALENo ratings yet