You might also like
- فرصت اشتباه my7oshicyggyDocument4 pagesفرصت اشتباه my7oshicyggyaaes2No ratings yet
- G.711, G.721, G.726 and G.728 Codecs VoipDocument5 pagesG.711, G.721, G.726 and G.728 Codecs Voipaaes2No ratings yet
- How Credit Cards WorkDocument22 pagesHow Credit Cards Workaaes2No ratings yet
- Clinical Excellence-V2n1p50-En PDFDocument20 pagesClinical Excellence-V2n1p50-En PDFaaes2No ratings yet
- Clinical Excellence-V2n1p50-En PDFDocument20 pagesClinical Excellence-V2n1p50-En PDFaaes2No ratings yet
- Electronic Check ProcessingDocument1 pageElectronic Check Processingaaes2No ratings yet
- The Telecheckinternet Check Acceptance and Checks by Phone ServiceDocument1 pageThe Telecheckinternet Check Acceptance and Checks by Phone Serviceaaes2No ratings yet
- Supporting The SBR Style of Web Usage: Engine. There Are Other Forms of SearchDocument6 pagesSupporting The SBR Style of Web Usage: Engine. There Are Other Forms of Searchaaes2No ratings yet
- Advanced Encryption Standard (AES) : Feature OverviewDocument20 pagesAdvanced Encryption Standard (AES) : Feature Overviewaaes2No ratings yet
- Almost in Praise of MicrosoftDocument4 pagesAlmost in Praise of Microsoftaaes2No ratings yet
- Secure Hash Algorithm (SHA-1) Encryption Standard: VOCAL Technologies, Ltd. Home Page Contact Us About UsDocument1 pageSecure Hash Algorithm (SHA-1) Encryption Standard: VOCAL Technologies, Ltd. Home Page Contact Us About Usaaes2No ratings yet
- Fips 197Document51 pagesFips 197Anoop KumarNo ratings yet
- Electronic Check ProcessingDocument1 pageElectronic Check Processingaaes2No ratings yet
- Speak Freely Application Programming Interface: Draft 0.1 - 06/03/1999 by Brian C. WilesDocument7 pagesSpeak Freely Application Programming Interface: Draft 0.1 - 06/03/1999 by Brian C. Wilesaaes2No ratings yet
- NVR Camera Capacity Based On Bit RateDocument2 pagesNVR Camera Capacity Based On Bit RatemastaacaNo ratings yet
- NSumsDocument9 pagesNSumsaaes2No ratings yet
- Malware Binary Deobfuscation PDFDocument14 pagesMalware Binary Deobfuscation PDFaaes2No ratings yet
- KX-TGEA20 KX-TGHA20: Additional Digital Cordless HandsetDocument12 pagesKX-TGEA20 KX-TGHA20: Additional Digital Cordless Handsetaaes2No ratings yet
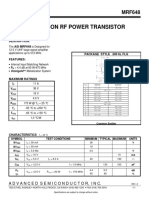
- MRF648Document1 pageMRF648aaes2No ratings yet
- Malware Binary Deobfuscation PDFDocument14 pagesMalware Binary Deobfuscation PDFaaes2No ratings yet
- Leadtek Winfast TV Pro II PDFDocument18 pagesLeadtek Winfast TV Pro II PDFAndreea Si EduardNo ratings yet
- Learn Farsi 1Document347 pagesLearn Farsi 1aaes2No ratings yet
- Understanding Genitourinary System CytologyDocument130 pagesUnderstanding Genitourinary System Cytologyaaes2No ratings yet
- IPv6 Chart 2015Document2 pagesIPv6 Chart 2015aaes2No ratings yet
- Link Planner Release Notes v4.6.3Document67 pagesLink Planner Release Notes v4.6.3aaes2No ratings yet
- SC8108-A Network Cable Tester ManualDocument20 pagesSC8108-A Network Cable Tester ManualclarkykentyNo ratings yet
- 2 SC 1971Document1 page2 SC 1971aaes2No ratings yet
- Workstation Pro 12 User GuideDocument294 pagesWorkstation Pro 12 User GuideJohn WeenNo ratings yet
- Konica Minolta ESP Matrix-45Document4 pagesKonica Minolta ESP Matrix-45suverxNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Domingo, Precious Mae TDocument56 pagesDomingo, Precious Mae Tbevzie datuNo ratings yet
- Medicinal Plants and Their Components For Wound Healing ApplicationsDocument13 pagesMedicinal Plants and Their Components For Wound Healing ApplicationsKing NguyenNo ratings yet
- Poisons of Plant OriginDocument46 pagesPoisons of Plant OriginThe AbyssinicansNo ratings yet
- Drug StudyDocument2 pagesDrug Studykev mondaNo ratings yet
- Community Health Nursing NCLEX Questions - 51 TermsDocument18 pagesCommunity Health Nursing NCLEX Questions - 51 TermsCharaNo ratings yet
- Managing Hypertension Through Diet and Lifestyle ChangesDocument1 pageManaging Hypertension Through Diet and Lifestyle ChangesChristian Daayata0% (1)
- Critique Paper01 - DabloDocument2 pagesCritique Paper01 - DabloFheevNo ratings yet
- SCORE Project Form Internal Medicine DepartmentDocument7 pagesSCORE Project Form Internal Medicine DepartmentGeorge CobuzNo ratings yet
- Geriatric Physical AssessmentDocument6 pagesGeriatric Physical AssessmentKrizzle Mae NeypesNo ratings yet
- Stemi Mimics PDFDocument112 pagesStemi Mimics PDFdeepuvbhanuNo ratings yet
- LOVEYOURCONTENTSTDPregnancyStudentWorkbook PDFDocument24 pagesLOVEYOURCONTENTSTDPregnancyStudentWorkbook PDFChlodette Eizl M. Laurente100% (1)
- Personality DisordersDocument125 pagesPersonality DisordersDevendra Singh Baryah100% (2)
- 2017 Infectious Diseases Society of America's Clinical Practice Guidelines For Healthcare-Associated Ventriculitis and MeningitisDocument32 pages2017 Infectious Diseases Society of America's Clinical Practice Guidelines For Healthcare-Associated Ventriculitis and MeningitisEugen TarnovschiNo ratings yet
- Health7 Q4 Mod4 ProgramsAndPoliciesToPreventNon-communicableDiseases 05102021Document22 pagesHealth7 Q4 Mod4 ProgramsAndPoliciesToPreventNon-communicableDiseases 05102021kiahjessieNo ratings yet
- Sub - Medical Surgical Nursing: Assignment On CVP MonitoringDocument11 pagesSub - Medical Surgical Nursing: Assignment On CVP Monitoringkamini ChoudharyNo ratings yet
- Gardasil 9 Summary of Product CharacteristicsDocument46 pagesGardasil 9 Summary of Product CharacteristicsEllaNo ratings yet
- 1 s2.0 S1074761321003654 MainDocument35 pages1 s2.0 S1074761321003654 MainIoana BiticaNo ratings yet
- Case Study On ManiaDocument30 pagesCase Study On ManiaIOM BNS75% (8)
- Group Declaration Form - NGIDocument2 pagesGroup Declaration Form - NGIrehman nikhatNo ratings yet
- High quality blood agar production with MEDIAJET and DOSE ITDocument2 pagesHigh quality blood agar production with MEDIAJET and DOSE ITBenjamin TantiansuNo ratings yet
- Communication Is Difficult': Speech, Language and Communication Needs of People With Young Onset or Rarer Forms of Non-Language Led DementiaDocument25 pagesCommunication Is Difficult': Speech, Language and Communication Needs of People With Young Onset or Rarer Forms of Non-Language Led DementiaLlamadme ImanolNo ratings yet
- Rivaroxaban ArticleDocument12 pagesRivaroxaban ArticleA. RaufNo ratings yet
- Professional English For Physical SciencesDocument134 pagesProfessional English For Physical SciencesRavindranathan ArumugamNo ratings yet
- DT 2N EU EN safetyDataSheet Sds 8799831064580 0 1Document12 pagesDT 2N EU EN safetyDataSheet Sds 8799831064580 0 1Jonatan BernalNo ratings yet
- LECTURE - 8 Biomaterial PDFDocument34 pagesLECTURE - 8 Biomaterial PDFYoza FendrianiNo ratings yet
- Pathcare Labs Antenatal Test ReportDocument8 pagesPathcare Labs Antenatal Test ReportTrilok TripathiNo ratings yet
- Philippine Pediatric Society, IncDocument41 pagesPhilippine Pediatric Society, IncMark Cristopher JoaquinNo ratings yet
- Clinical Guidelines PDFDocument19 pagesClinical Guidelines PDFEmilio AcostaNo ratings yet
- Brain - Drain The Impact of Air Pulution On Firm PerformanceDocument69 pagesBrain - Drain The Impact of Air Pulution On Firm PerformancesinhNo ratings yet
- Vol22no4 PDF VersionDocument200 pagesVol22no4 PDF VersionMia Fernandez100% (1)