You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5796)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Urinary Tract Infections ChildrenDocument26 pagesUrinary Tract Infections ChildrenbrianzflNo ratings yet
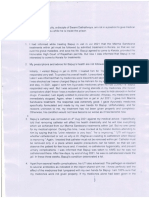
- DR Raghavan's Statement 14092021Document3 pagesDR Raghavan's Statement 14092021Ravi Rai MarwahNo ratings yet
- Hematuria: Gross Versus Microscopic HematuriaDocument2 pagesHematuria: Gross Versus Microscopic HematuriaShintia Theresia LumempouwNo ratings yet
- For Mule DetoxDocument59 pagesFor Mule Detoxkorki77No ratings yet
- (Concept Map) Urinary Tract InfectionsDocument1 page(Concept Map) Urinary Tract InfectionsRica Alyssa PepitoNo ratings yet
- Check - Unit - 554 - October - Renal - Problems V2 PDFDocument26 pagesCheck - Unit - 554 - October - Renal - Problems V2 PDFdragon660% (1)
- Project Protocol 2Document4 pagesProject Protocol 2bhargavNo ratings yet
- Topnotch IM For MoonlightersDocument274 pagesTopnotch IM For Moonlightersmefav7778520100% (2)
- Renal Health Advocacy For Nurses in La Union 1325915359Document13 pagesRenal Health Advocacy For Nurses in La Union 1325915359Rizki MatondangNo ratings yet
- Lehnes Pharmacology For Nursing Care 10th Edition Burchum Test BankDocument35 pagesLehnes Pharmacology For Nursing Care 10th Edition Burchum Test Bankmanganicidealityfy9rc1100% (19)
- Puerperal Pyrexia 2Document7 pagesPuerperal Pyrexia 2dyah ayu noer fadilaNo ratings yet
- A Colour Handbook of Urinary Stones in Small Animal MedicineDocument186 pagesA Colour Handbook of Urinary Stones in Small Animal Medicinedia_dianne100% (1)
- UTI BrochureDocument2 pagesUTI BrochureKaye de LeonNo ratings yet
- NCM109Document4 pagesNCM109Cherry Ann Cagayat MadrigalNo ratings yet
- Buletin Farmasi 1/2014Document14 pagesBuletin Farmasi 1/2014afiq83100% (1)
- Section 1 Functional Disturbances and Diseases of Kidneys: DR - Damodar SedaiDocument82 pagesSection 1 Functional Disturbances and Diseases of Kidneys: DR - Damodar SedaiShreeya SharmaNo ratings yet
- Costy Panjaitan - Materi KARS SURVEILANS NEW PDFDocument40 pagesCosty Panjaitan - Materi KARS SURVEILANS NEW PDFRr.Tutik SRi HariyatiNo ratings yet
- Aubf M5u1 (Highlighted)Document17 pagesAubf M5u1 (Highlighted)proximusNo ratings yet
- Funda Urine CollectionDocument26 pagesFunda Urine CollectionClaryse EroyNo ratings yet
- Emergency Room PortfolioDocument18 pagesEmergency Room PortfolioEricka SantosNo ratings yet
- Ultrasonographic Diagnosis of Urachal Anomalies in Cats and Dogs: Retrospective Study of 98 Cases (2009-2019)Document12 pagesUltrasonographic Diagnosis of Urachal Anomalies in Cats and Dogs: Retrospective Study of 98 Cases (2009-2019)aeliyyah jannahNo ratings yet
- Urinary Retention in AdultsDocument12 pagesUrinary Retention in AdultsVaraalakshmy GokilavananNo ratings yet
- SC Managing Illness IIDocument124 pagesSC Managing Illness IImahlowhnahmoneth17No ratings yet
- Urinary Tract Infection (UTI) in Males: Signs and SymptomsDocument33 pagesUrinary Tract Infection (UTI) in Males: Signs and Symptomssyak turNo ratings yet
- Cephalosporin Antibiotics: From 7-Aminocephalosporanic Acid - Produced by FermentationDocument23 pagesCephalosporin Antibiotics: From 7-Aminocephalosporanic Acid - Produced by FermentationVeChrist PharmacistoLshopNo ratings yet
- Treatment of Non Muscle Invasive Bladder Cancer With BCG and Emda MMCDocument7 pagesTreatment of Non Muscle Invasive Bladder Cancer With BCG and Emda MMCRyan IlhamNo ratings yet
- Urinary Tract Anti Infective AgentsDocument48 pagesUrinary Tract Anti Infective AgentsGunjan Yadav100% (1)
- Nursing Care of Women With Complications After Birth - Group#2Document10 pagesNursing Care of Women With Complications After Birth - Group#2Lyza MateoNo ratings yet
- CMS FM Form 1Document9 pagesCMS FM Form 1Ali HamzaNo ratings yet