You might also like
- Spinal Cord Injuries and SyndromeDocument18 pagesSpinal Cord Injuries and SyndromeKim Sunoo100% (1)
- Peripheral NeurologyDocument38 pagesPeripheral NeurologyAnna Stacy100% (1)
- Sacroiliac Joint Dysfunction and Piriformis Syndrome PDFDocument37 pagesSacroiliac Joint Dysfunction and Piriformis Syndrome PDFDevi SiswaniNo ratings yet
- Nerve of The Lower Limb Edited LagiDocument159 pagesNerve of The Lower Limb Edited Lagifathizu100% (1)
- Low Back PainDocument100 pagesLow Back Painchandrusai100% (1)
- (New Procedures in Spinal Interventional Neuroradiology) Luigi Manfrà (Eds.) - Spinal Canal Stenosis-Springer International PublisDocument98 pages(New Procedures in Spinal Interventional Neuroradiology) Luigi Manfrà (Eds.) - Spinal Canal Stenosis-Springer International PublisThuyet Nguyen PhuocNo ratings yet
- Wrist Anatomy: Bones Quiz - What Bones Comprise The Wrist? Joints Quiz - What Joints Comprise The Wrist?Document63 pagesWrist Anatomy: Bones Quiz - What Bones Comprise The Wrist? Joints Quiz - What Joints Comprise The Wrist?Mnn SaabNo ratings yet
- Orthopedics Notes for Medical StudentsFrom EverandOrthopedics Notes for Medical StudentsRating: 4.5 out of 5 stars4.5/5 (3)
- Common Injuries To The ElbowDocument88 pagesCommon Injuries To The ElbowmadhupgiNo ratings yet
- Degenerative Disorders of Lumbar SpineDocument54 pagesDegenerative Disorders of Lumbar Spineapi-19916399No ratings yet
- Orthopath Final ReviewDocument16 pagesOrthopath Final ReviewharrischoeNo ratings yet
- Cervical Spine DisorderDocument9 pagesCervical Spine DisorderANDRE MANo ratings yet
- I. Cutting and DissectingDocument10 pagesI. Cutting and DissectingApple MaeNo ratings yet
- Musculoskeletal TraumaDocument63 pagesMusculoskeletal Traumarobby pardiansyahNo ratings yet
- Fracture of Shaft FemurDocument55 pagesFracture of Shaft FemurFadliArifNo ratings yet
- Kuliah Spine TraumaDocument91 pagesKuliah Spine TraumaEvi MaisyariNo ratings yet
- Cervical SpineDocument3 pagesCervical SpineCherrie MaeNo ratings yet
- Introduction of MSK ImagingDocument63 pagesIntroduction of MSK ImagingyeabsraNo ratings yet
- Spinal InjuriesDocument65 pagesSpinal InjuriesDenuna EnjanaNo ratings yet
- 1.3 Soft Tissue InjuryDocument44 pages1.3 Soft Tissue InjurySylvinho46100% (1)
- Peripheral Neuropathies FOR CLASSIFICATIONDocument9 pagesPeripheral Neuropathies FOR CLASSIFICATIONAnnie JoNo ratings yet
- Postoperative Nursing ManagementDocument12 pagesPostoperative Nursing ManagementAhmed AliNo ratings yet
- Correction of Severe Bimaxillary ProtrusionDocument37 pagesCorrection of Severe Bimaxillary ProtrusionRobbyRamadhonieNo ratings yet
- Spinal Cord Injury AlexiDocument41 pagesSpinal Cord Injury AlexiRoberto AlexiNo ratings yet
- Bone HealingDocument5 pagesBone HealingFadliArifNo ratings yet
- UMS Orthopedic Short Cases Records 1st EditionDocument15 pagesUMS Orthopedic Short Cases Records 1st EditionHayati Nasir100% (2)
- Empanelled Network Hospital List (PAN India)Document281 pagesEmpanelled Network Hospital List (PAN India)Vairamuthu CNo ratings yet
- Management of Stoma, Cut and WoundsDocument40 pagesManagement of Stoma, Cut and WoundsLalita KumariNo ratings yet
- Entrapment Neuropathies Conversion-GateDocument76 pagesEntrapment Neuropathies Conversion-GateRam ReddyNo ratings yet
- Spine Emergencies: Spinal Cord Injury (SCI) - The BasicsDocument67 pagesSpine Emergencies: Spinal Cord Injury (SCI) - The Basicsditya_madridistasNo ratings yet
- TrunkDocument86 pagesTrunkdr_asalehNo ratings yet
- Evaluation of Low Back Pain (Ray)Document81 pagesEvaluation of Low Back Pain (Ray)Naeem AminNo ratings yet
- 7 Question OrthopaedyDocument11 pages7 Question OrthopaedyFadliArifNo ratings yet
- NN LBPDocument50 pagesNN LBPEdmonLagartoNo ratings yet
- Spinal Trauma Update Bryan BledsoeDocument80 pagesSpinal Trauma Update Bryan BledsoeMuhammad YaminNo ratings yet
- Anatomia Da ColunaDocument59 pagesAnatomia Da ColunaPaula Duarte MarquesNo ratings yet
- Huffman-Hip Pelvis Shoulder X-RaysDocument17 pagesHuffman-Hip Pelvis Shoulder X-RaysRoni PahlawanNo ratings yet
- New Biomechanics of Elbow - Wrist JointDocument33 pagesNew Biomechanics of Elbow - Wrist JointFatima AnjumNo ratings yet
- 1.12 Cervical and Low Back Pain and RadiculopDocument42 pages1.12 Cervical and Low Back Pain and RadiculopsiusiuwidyantoNo ratings yet
- Lumber InjuriesDocument15 pagesLumber InjuriesDinesh ChoudharyNo ratings yet
- Chapter Iv. Lumbago-Sciatica PDFDocument25 pagesChapter Iv. Lumbago-Sciatica PDFWilliam C ChishaNo ratings yet
- Spinal Cord Injuries: Dr. Ikhsan HidayatDocument53 pagesSpinal Cord Injuries: Dr. Ikhsan HidayatSandroNo ratings yet
- Efficacy of Faradic Electrical Stimultion IN REDUCING PAIN AND RANGE OF MOTION IN PATIENTS WITH CHRONIC LATERAL EPICONDYLITISDocument63 pagesEfficacy of Faradic Electrical Stimultion IN REDUCING PAIN AND RANGE OF MOTION IN PATIENTS WITH CHRONIC LATERAL EPICONDYLITISpriyanka muthavarapuNo ratings yet
- Canal Stenosis - ERHDocument56 pagesCanal Stenosis - ERHAries RHNo ratings yet
- Back and Nexk PainDocument7 pagesBack and Nexk PainDenise MathreNo ratings yet
- Notes SC NeurologyDocument7 pagesNotes SC Neurology202213No ratings yet
- Orthopaedic!Document15 pagesOrthopaedic!bowelprepcolonNo ratings yet
- Spinal Cord Injury and CompressionDocument10 pagesSpinal Cord Injury and CompressionAdeputhNo ratings yet
- 2.299224 - Initial Assessment Musculoskeletal TraumaDocument63 pages2.299224 - Initial Assessment Musculoskeletal TraumaMuhammad GilangNo ratings yet
- CLINICAL NEUROLOGY II Assignment 1Document8 pagesCLINICAL NEUROLOGY II Assignment 1Muskan AhujaNo ratings yet
- Lumbar Spinal Stenosis: Pathophysiology, Clinical Features, and DiagnosisDocument14 pagesLumbar Spinal Stenosis: Pathophysiology, Clinical Features, and DiagnosisAnastasia TjanNo ratings yet
- Thoracolumbarfractures 150817055817 Lva1 App6891Document75 pagesThoracolumbarfractures 150817055817 Lva1 App6891Pap PipNo ratings yet
- Trauma Medulla SpinalisDocument79 pagesTrauma Medulla SpinalisiqiqiqiqiqNo ratings yet
- 6a. Anatomi Dan Biomekanik Trauma Tulang BelakangDocument53 pages6a. Anatomi Dan Biomekanik Trauma Tulang BelakangnurwajdainiNo ratings yet
- Emergency Imaging Course 3 Spine MSK Vessels NoimagDocument96 pagesEmergency Imaging Course 3 Spine MSK Vessels NoimagAlex DanciuNo ratings yet
- Cauda-Conus SyndromesDocument28 pagesCauda-Conus Syndromessruthimeena6891No ratings yet
- PM&R in Degenearative Joint DiseaseDocument66 pagesPM&R in Degenearative Joint DiseaseLorenz SmallNo ratings yet
- The Spine and LimbsDocument7 pagesThe Spine and LimbsFrancesca vitaleNo ratings yet
- Spine RehabilationDocument157 pagesSpine RehabilationSyeda Abida Hussain SheraziNo ratings yet
- Acute Low Back PainDocument39 pagesAcute Low Back PainSathish KumarNo ratings yet
- ManoDocument26 pagesManoRoger Zambrana FloresNo ratings yet
- Peripheral Nerve Injuries c61Document69 pagesPeripheral Nerve Injuries c61Kevo YoungNo ratings yet
- 2015 - 03 - 26 NEJM SciaticaDocument9 pages2015 - 03 - 26 NEJM SciaticaShaun TylerNo ratings yet
- Lesi Medula Spinalis Khronis AaDocument49 pagesLesi Medula Spinalis Khronis AaNisha AnggiaNo ratings yet
- Peripheral NerveDocument48 pagesPeripheral Nervewhite.bear251102No ratings yet
- VIVA NOV 2018 SPINE Examiner VersionDocument13 pagesVIVA NOV 2018 SPINE Examiner VersionFadliArifNo ratings yet
- 5 Question OrthopaedyDocument5 pages5 Question OrthopaedyFadliArifNo ratings yet
- 1 Question OrthopaedyDocument15 pages1 Question OrthopaedyFadliArifNo ratings yet
- Ilioinguinal Approach To The AcetabulumDocument14 pagesIlioinguinal Approach To The AcetabulumFadliArifNo ratings yet
- Hip Medial ApproachDocument10 pagesHip Medial ApproachFadliArifNo ratings yet
- Risk Factors of Venous Thromboembolism in Indian Patients With Pelvic-Acetabular TraumaDocument8 pagesRisk Factors of Venous Thromboembolism in Indian Patients With Pelvic-Acetabular TraumaFadliArifNo ratings yet
- Journal Reading DigestivDocument35 pagesJournal Reading DigestivFadliArifNo ratings yet
- Maxillary Injection TechniquesDocument127 pagesMaxillary Injection TechniquesD YasIr MussaNo ratings yet
- Peterson's Principals of Oral and Maxyofacial Surgery Ch.0008 - Impacted TeethDocument18 pagesPeterson's Principals of Oral and Maxyofacial Surgery Ch.0008 - Impacted TeethДимитър АлександровNo ratings yet
- Fracture FemurDocument19 pagesFracture FemurWahida PutriNo ratings yet
- CV Abdelgadir Ahmed Eltayeb.Document7 pagesCV Abdelgadir Ahmed Eltayeb.AbdelgadirEltayebNo ratings yet
- EVALUATION Book Intern Medical-2023 Report 2Document1 pageEVALUATION Book Intern Medical-2023 Report 2Ahsif IsmailNo ratings yet
- Surgical Guide For Dental Implant Placement: PresentedDocument4 pagesSurgical Guide For Dental Implant Placement: PresentedAmy CuadraNo ratings yet
- Katz Et Al. - 2018 - Changes in Subcutaneous Abdominal Fat Thickness Following High-Intensity Focused Electro-MagneticDocument2 pagesKatz Et Al. - 2018 - Changes in Subcutaneous Abdominal Fat Thickness Following High-Intensity Focused Electro-MagneticNicolas FarkasNo ratings yet
- Temporomandibular Joint Ankylosis: Algorithm of TreatmentDocument5 pagesTemporomandibular Joint Ankylosis: Algorithm of TreatmentVictoria DolințăNo ratings yet
- A Case Study of Splenic Hemangiosarcoma in A Bitch and Its Surgical ManagementDocument3 pagesA Case Study of Splenic Hemangiosarcoma in A Bitch and Its Surgical ManagementWira KusumaNo ratings yet
- GORDONS 11 HEALTH FUNCTIONAL PATTERNS DraftDocument8 pagesGORDONS 11 HEALTH FUNCTIONAL PATTERNS DraftJessa C. BorjaNo ratings yet
- CBCTDocument7 pagesCBCTnaveedtariqsyedNo ratings yet
- Core Clerkship GuideDocument18 pagesCore Clerkship GuideEduardo CésarNo ratings yet
- Annex 6. List of Procedure Case Rates For Primary Care Facilities - Infirmaries/ DispensariesDocument22 pagesAnnex 6. List of Procedure Case Rates For Primary Care Facilities - Infirmaries/ DispensariesBiko LabbitNo ratings yet
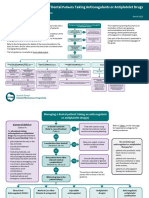
- Sdcep Anticoagulants Quick Reference Guide 2nd EditionDocument5 pagesSdcep Anticoagulants Quick Reference Guide 2nd EditionMeryem LahlouNo ratings yet
- Medial Patellar DesmotomyDocument19 pagesMedial Patellar Desmotomynitish narwalNo ratings yet
- ARTIKEL - Nur Aas AisahDocument8 pagesARTIKEL - Nur Aas Aisahaas aisahNo ratings yet
- Povidone Iodine Use in Hand Disinfectionskin Preparation and Antiseptic IrrigationDocument12 pagesPovidone Iodine Use in Hand Disinfectionskin Preparation and Antiseptic Irrigationpendekar bodohNo ratings yet
- HerniaDocument67 pagesHerniaياسر نعيم الربيعي100% (1)
- Jewett and Cash BraceDocument19 pagesJewett and Cash BraceucssNo ratings yet
- Copper Ridge Health and Rehabilitation Center 07-31-2018Document3 pagesCopper Ridge Health and Rehabilitation Center 07-31-2018NBC MontanaNo ratings yet
- Clinical Preview About Hernia: It's Types, Clinical Presentation, Diagnosis and RepairDocument10 pagesClinical Preview About Hernia: It's Types, Clinical Presentation, Diagnosis and RepairAfnan AdelNo ratings yet
- 1 s2.0 S2213576622002986 MainDocument4 pages1 s2.0 S2213576622002986 Maindr. Nur'aini HasanNo ratings yet
- Role Responsibilities of Radiographer NewDocument49 pagesRole Responsibilities of Radiographer Newjiminsarah88No ratings yet
- GMC HCL 22-23-MedibuddyDocument4 pagesGMC HCL 22-23-MedibuddyVikas Kumar PandeyNo ratings yet