You might also like
- Katzung QuestionsDocument29 pagesKatzung QuestionsToastie3100% (12)
- Paul Manning-Drugs and Popular CultureDocument302 pagesPaul Manning-Drugs and Popular CultureMaria Paktiti100% (1)
- Stages of Anaesthesia NotesDocument2 pagesStages of Anaesthesia NotesNomathamsanqa Khumalo100% (2)
- Sports Injuries - Prevention, Diagnosis, Treatment and Rehabilitation (PDFDrive) PDFDocument3,295 pagesSports Injuries - Prevention, Diagnosis, Treatment and Rehabilitation (PDFDrive) PDFRadu Urcan100% (2)
- Anaesthesia Equipment: Anaesthetics OSCE (Compiled by C Lee Kin) 1Document98 pagesAnaesthesia Equipment: Anaesthetics OSCE (Compiled by C Lee Kin) 1Shen BNo ratings yet
- Complications of Spinal and Epidural AnesthesiaDocument45 pagesComplications of Spinal and Epidural AnesthesiashikhaNo ratings yet
- Anaesthesia & Intensive Care: For Fcai, Frca EdaicDocument139 pagesAnaesthesia & Intensive Care: For Fcai, Frca EdaicMuhammad Farid100% (2)
- BASIC Exam Blueprint PDFDocument3 pagesBASIC Exam Blueprint PDFmichael100% (1)
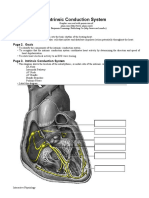
- Intrinsic Conduction System: Page 1. IntroductionDocument5 pagesIntrinsic Conduction System: Page 1. IntroductionUta Provinsiana SukmaraNo ratings yet
- Broiler Chicken FarmingDocument6 pagesBroiler Chicken FarmingYani Hardinata HairuddinNo ratings yet
- Medical-Surgical Nursing Skills ChecklistDocument2 pagesMedical-Surgical Nursing Skills ChecklistApple Maiquez GarciaNo ratings yet
- NCP (PEDIA Tonsillitis)Document2 pagesNCP (PEDIA Tonsillitis)Athena Kabigting64% (14)
- Management of High Spinal AnesthesiaDocument8 pagesManagement of High Spinal AnesthesiaYeni TriastutikNo ratings yet
- Differentiating Anesthesia Equipment: Identify and Understand Anesthesia Equipment in 1 Hour (Including the most popular manufacturers and suppliers to buy Anesthesia Equipment)From EverandDifferentiating Anesthesia Equipment: Identify and Understand Anesthesia Equipment in 1 Hour (Including the most popular manufacturers and suppliers to buy Anesthesia Equipment)No ratings yet
- Anesthesia For Bariatric SurgeryDocument47 pagesAnesthesia For Bariatric Surgerydkhiloi100% (1)
- Update 34 Obstetric Edition Sept 2019 FinalDocument100 pagesUpdate 34 Obstetric Edition Sept 2019 FinalRian ArmiNo ratings yet
- Comparison of Two Approaches ofDocument96 pagesComparison of Two Approaches ofJacob OrtizNo ratings yet
- Paediatric Anaesthesia PDFDocument33 pagesPaediatric Anaesthesia PDFMarcelitaTaliaDuwiriNo ratings yet
- Examinations Regulations 2018 Mcai FcaiDocument13 pagesExaminations Regulations 2018 Mcai FcaiTahseen TalibNo ratings yet
- Anesthetic Machine For StudentDocument76 pagesAnesthetic Machine For StudentMohmmed MousaNo ratings yet
- @anesthesia Books 2018 GuidelinesDocument16 pages@anesthesia Books 2018 GuidelinesAgil Rumboko SumitroNo ratings yet
- Race 2007 PDFDocument236 pagesRace 2007 PDFRois Hasyim100% (1)
- Textbook of Anaesthesia For Postgraduates PDFDocument1,218 pagesTextbook of Anaesthesia For Postgraduates PDFMohammad HayajnehNo ratings yet
- Update EmergenciesDocument84 pagesUpdate EmergenciesElaineNo ratings yet
- Anaesthesia For Day Case Surgery PDFDocument119 pagesAnaesthesia For Day Case Surgery PDFsabbo morsNo ratings yet
- AnaesthesiaDocument44 pagesAnaesthesiamadmaxmaxmus50% (2)
- Anaesthesia For Thyroid Surgery....Document46 pagesAnaesthesia For Thyroid Surgery....Parvathy R NairNo ratings yet
- AnaesthesiaDocument5 pagesAnaesthesiaAnonymous 4jkFIRalKNo ratings yet
- Controlled Hypotensive AnesthesiaDocument24 pagesControlled Hypotensive AnesthesiaSuresh Kumar100% (1)
- Pediatric AnesthesiaDocument70 pagesPediatric AnesthesiaEliyan KhanimovNo ratings yet
- Thsesis TopicsDocument17 pagesThsesis Topicsvvb_frndNo ratings yet
- Pediatric Anesthesiology PDFDocument309 pagesPediatric Anesthesiology PDFAviv Pasa100% (1)
- Management of Failed Block - Harsh.Document48 pagesManagement of Failed Block - Harsh.Faeiz KhanNo ratings yet
- Safe Pediatric AnesthesiaDocument24 pagesSafe Pediatric AnesthesiamdNo ratings yet
- Anesthesiology FCPS 2017Document84 pagesAnesthesiology FCPS 2017Tabish JavaidNo ratings yet
- Anestesia Pediatrica 2015Document292 pagesAnestesia Pediatrica 2015Eloy BurdaNo ratings yet
- Telegram Cloud Document 4 5893461163299045618 PDFDocument232 pagesTelegram Cloud Document 4 5893461163299045618 PDFAndreea FlorinaNo ratings yet
- Technique For Awake Fibre Optic IntubationDocument3 pagesTechnique For Awake Fibre Optic Intubationmonir61No ratings yet
- Fred Rotenberg, MD Dept. of Anesthesiology Rhode Island Hospital Grand Rounds February 27, 2008Document53 pagesFred Rotenberg, MD Dept. of Anesthesiology Rhode Island Hospital Grand Rounds February 27, 2008lmjeksoreNo ratings yet
- 17-18 Chong Kar Mun's Anaesthesia NotesDocument32 pages17-18 Chong Kar Mun's Anaesthesia NotesElaineNo ratings yet
- Regional Anesthesia - FinalDocument46 pagesRegional Anesthesia - Finalvan016_bunnyNo ratings yet
- 7..intravenous Anaesthesia 2Document23 pages7..intravenous Anaesthesia 2Mwiliza BrendaNo ratings yet
- Exm Sba July2012 PDFDocument5 pagesExm Sba July2012 PDFSuhas KapseNo ratings yet
- Paediatric Regional AnaesthesiaDocument24 pagesPaediatric Regional Anaesthesiazatvit100% (2)
- Anesthesia Pre Operative EvaluationDocument27 pagesAnesthesia Pre Operative EvaluationHassan.shehri100% (2)
- Comprehensive Board Review 2015 PDFDocument713 pagesComprehensive Board Review 2015 PDFHuma KhalidNo ratings yet
- Anaesthesia and Sedation Outside TheatresDocument15 pagesAnaesthesia and Sedation Outside Theatresمحمد زينNo ratings yet
- Final THESIS 1-116 To PrintDocument116 pagesFinal THESIS 1-116 To PrintMahesh RajwalNo ratings yet
- Obstetrics AnesthesiaDocument55 pagesObstetrics AnesthesiaJohn Paulo Catacutan100% (2)
- Essentials of Anesthesia For Medical Students FinalDocument82 pagesEssentials of Anesthesia For Medical Students FinalEs LamNo ratings yet
- 21 Obstetric Anaesthesia PDFDocument0 pages21 Obstetric Anaesthesia PDFjuniorebindaNo ratings yet
- Skeletalmusclerelaxants 151101095949 Lva1 App6891 PDFDocument69 pagesSkeletalmusclerelaxants 151101095949 Lva1 App6891 PDFvvb_frndNo ratings yet
- Neuraxial Anaesthesia: DR Ali Rahman Assistant Professor - Anaesthesiology Department (RMDC)Document27 pagesNeuraxial Anaesthesia: DR Ali Rahman Assistant Professor - Anaesthesiology Department (RMDC)fahadali2000No ratings yet
- Blood Conservation StrategiesDocument31 pagesBlood Conservation Strategiesthalida24100% (1)
- Report On The Constructed Response Question / Short Answer Question Paper - September 2019Document6 pagesReport On The Constructed Response Question / Short Answer Question Paper - September 2019cr7No ratings yet
- Anesthetic AgentsDocument7 pagesAnesthetic AgentsJan DacioNo ratings yet
- 029 Reddy PDFDocument59 pages029 Reddy PDFKonas Xi PalembangNo ratings yet
- Brachial Plexus BlockDocument13 pagesBrachial Plexus BlockAnkit Shah100% (1)
- FRCA Syllabus PDFDocument4 pagesFRCA Syllabus PDFSuhas KapseNo ratings yet
- List of Must Read Books and Journals For DNB AnaesthesiaDocument2 pagesList of Must Read Books and Journals For DNB AnaesthesiaSirisha CkvNo ratings yet
- The Hong Kong College of Anaesthesiologists Final Fellowship Examination July/September 2007 Examiners ReportDocument16 pagesThe Hong Kong College of Anaesthesiologists Final Fellowship Examination July/September 2007 Examiners ReportJane KoNo ratings yet
- 6.monitoring in AnesthesiaDocument46 pages6.monitoring in AnesthesiaIlham rianda100% (5)
- Pediatric AnesthesiaDocument194 pagesPediatric AnesthesiaSwamynadh Gandhi ReddiNo ratings yet
- Paediatric Anesthesiology - Anesthesiology ClinicsDocument309 pagesPaediatric Anesthesiology - Anesthesiology ClinicsAbdullah QaziNo ratings yet
- UiA 33 Final Replacement Web 2Document80 pagesUiA 33 Final Replacement Web 2uzairNo ratings yet
- Principles and Practice of Pharmacology for AnaesthetistsFrom EverandPrinciples and Practice of Pharmacology for AnaesthetistsRating: 5 out of 5 stars5/5 (1)
- Anatomy Review: Blood Vessel Structure & Function: Page 1. Introduction Page 2. GoalsDocument6 pagesAnatomy Review: Blood Vessel Structure & Function: Page 1. Introduction Page 2. GoalsUta Provinsiana SukmaraNo ratings yet
- Autoregulation and Capillary Dynamics: Graphics Are Used With Permission ofDocument10 pagesAutoregulation and Capillary Dynamics: Graphics Are Used With Permission ofUta Provinsiana SukmaraNo ratings yet
- English Note Level 9Document5 pagesEnglish Note Level 9Uta Provinsiana SukmaraNo ratings yet
- E Colli Work GroupDocument4 pagesE Colli Work GroupUta Provinsiana SukmaraNo ratings yet
- English Assessment Physiotherapy & History Taking Dialogue EnglishDocument4 pagesEnglish Assessment Physiotherapy & History Taking Dialogue EnglishRobby FahrezaNo ratings yet
- A Review On Needle Free Injection SystemDocument11 pagesA Review On Needle Free Injection SystemShiji DanielNo ratings yet
- GoitreDocument2 pagesGoitresuggaplumNo ratings yet
- ARTIKEL ILMIAH (061611535039 - Novi Fitria Hanifah)Document10 pagesARTIKEL ILMIAH (061611535039 - Novi Fitria Hanifah)novi fitriaNo ratings yet
- Hospital Ownership Proforma RKCHMSDocument3 pagesHospital Ownership Proforma RKCHMSVishal ShrivastavaNo ratings yet
- CCPTC Model Prevention FinalDocument71 pagesCCPTC Model Prevention Finalsoyuzmedimaging and diagnostics ltdNo ratings yet
- Prosthodontic Care For Patients With Cleft PalateDocument7 pagesProsthodontic Care For Patients With Cleft PalateValery V JaureguiNo ratings yet
- Jurnal Inter Edema 3Document7 pagesJurnal Inter Edema 3Edom LazarNo ratings yet
- GENERIC NAME: FENOFIBRATE - ORAL (fen-oh-FYE-brate) BRAND NAME (S) : Tricor, TriglideDocument3 pagesGENERIC NAME: FENOFIBRATE - ORAL (fen-oh-FYE-brate) BRAND NAME (S) : Tricor, TriglideDevesh GaurNo ratings yet
- Depression Article LancetDocument13 pagesDepression Article LancetDjamil DamryNo ratings yet
- Chapter 1 Foundation of Modern NursingDocument30 pagesChapter 1 Foundation of Modern Nursingteklay100% (2)
- Intracranial HemorrhageDocument41 pagesIntracranial Hemorrhagedoctormussieaberra100% (1)
- InsubordinationDocument9 pagesInsubordinationLouie CascaraNo ratings yet
- Prof. DR. Dr. Soeharyo Hadisaputro, SP - PD-KPTI-Dengue Infection in SepsisDocument42 pagesProf. DR. Dr. Soeharyo Hadisaputro, SP - PD-KPTI-Dengue Infection in SepsisOlivia DwimaswastiNo ratings yet
- Cannabinoids in Blood and Urine After Passive Inhalation of Cannabis SmokeDocument6 pagesCannabinoids in Blood and Urine After Passive Inhalation of Cannabis SmokeaymansousaNo ratings yet
- Identify The Strategies and Contextual Factors That Enable Optimal Engagement of Patients in The Design, Delivery, and Evaluation of Health ServicesDocument2 pagesIdentify The Strategies and Contextual Factors That Enable Optimal Engagement of Patients in The Design, Delivery, and Evaluation of Health ServiceslouryNo ratings yet
- Exceptional Life BlueprintDocument20 pagesExceptional Life BlueprintTill SchmidtNo ratings yet
- Agro NursingDocument42 pagesAgro NursingAri YuanNo ratings yet
- Ebook Lippincott Q A Review For Nclex RN 11E Revised 11Th Edition Lippincott Williams Wilkins Lippincott Online PDF All ChapterDocument69 pagesEbook Lippincott Q A Review For Nclex RN 11E Revised 11Th Edition Lippincott Williams Wilkins Lippincott Online PDF All Chaptermichelle.saunders602100% (3)
- AMOEBADocument20 pagesAMOEBAChonalyn NolascoNo ratings yet
- DentalDocument68 pagesDentalDonna MurrayNo ratings yet
- Cardiogenic ShockDocument42 pagesCardiogenic ShockpashaNo ratings yet
- SCRM Part 3 - Examples Draft2 PDFDocument14 pagesSCRM Part 3 - Examples Draft2 PDFElena StoevaNo ratings yet
- Report - Case Study 11 - Obstetric Delivery - July 2010 - Hospital Review - 2009-10 - ApdDocument66 pagesReport - Case Study 11 - Obstetric Delivery - July 2010 - Hospital Review - 2009-10 - ApdAya TahaNo ratings yet