You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5810)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (844)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
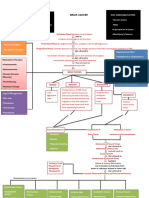
- Brain Cancer Concept MapDocument3 pagesBrain Cancer Concept MapIced Coffee100% (4)
- Bioptron Brochure ColorDocument43 pagesBioptron Brochure Colorvcurcubeului100% (1)
- Interpretation of Chest RadiographDocument7 pagesInterpretation of Chest RadiographhengkileonardNo ratings yet
- Nasser2015Document5 pagesNasser2015hengkileonardNo ratings yet
- Multimodality Cardiac Imaging of A Ventricular SepDocument4 pagesMultimodality Cardiac Imaging of A Ventricular SephengkileonardNo ratings yet
- Adriaans2019 Article PredictiveImagingForThoracicAoDocument9 pagesAdriaans2019 Article PredictiveImagingForThoracicAohengkileonardNo ratings yet
- Differential Diagnosis of Cerebellar Atrophy in Childhood An UpdateDocument13 pagesDifferential Diagnosis of Cerebellar Atrophy in Childhood An UpdatehengkileonardNo ratings yet
- 04-RCR-28-3-Algoritmos - Ingles (Para Publicacion)Document8 pages04-RCR-28-3-Algoritmos - Ingles (Para Publicacion)hengkileonardNo ratings yet
- Anatomi Otak Dan VertebrataDocument7 pagesAnatomi Otak Dan VertebratahengkileonardNo ratings yet
- Journal PediatricDocument18 pagesJournal PediatrichengkileonardNo ratings yet
- Jurnal CardioDocument10 pagesJurnal CardiohengkileonardNo ratings yet
- Endocrine Manifestations of Eating Disorders PDFDocument11 pagesEndocrine Manifestations of Eating Disorders PDFJaime GonzálezNo ratings yet
- Aesthetic, Breast 2001 PDFDocument124 pagesAesthetic, Breast 2001 PDFAhmed AttiaNo ratings yet
- What You Should Know Before You Start A Weight-Loss PlanDocument10 pagesWhat You Should Know Before You Start A Weight-Loss PlanRAKESH RANJANNo ratings yet
- Causal Argument Essay Rough DraftDocument6 pagesCausal Argument Essay Rough Draftapi-357113129No ratings yet
- Diagnosis and Management of Congenital Diaphragmatic Hernia A 2023Document14 pagesDiagnosis and Management of Congenital Diaphragmatic Hernia A 2023hosnameskarNo ratings yet
- G7-G10 Module-4Document16 pagesG7-G10 Module-4Jaddie LorzanoNo ratings yet
- Fox News: Watch TVDocument27 pagesFox News: Watch TVJoao WerleyNo ratings yet
- Bipolar Mood Tracking ChartDocument2 pagesBipolar Mood Tracking ChartMegan PenroseNo ratings yet
- RabiesDocument2 pagesRabiesninzah wanzahNo ratings yet
- A-1177-B-1 Part ADocument4 pagesA-1177-B-1 Part ADavid TrippNo ratings yet
- MODULE 6 Sir RobertDocument17 pagesMODULE 6 Sir RobertManilyn DominguezNo ratings yet
- Association of Multi-Drug Resistant Bacteria With Sanitation of Street Vendors FoodDocument14 pagesAssociation of Multi-Drug Resistant Bacteria With Sanitation of Street Vendors FoodMamta AgarwalNo ratings yet
- Sgrfull 1Document300 pagesSgrfull 1Victor SilvaNo ratings yet
- IbandronatedrugscomDocument25 pagesIbandronatedrugscomroyNo ratings yet
- Dias2009 Article PantoprazoleDocument10 pagesDias2009 Article PantoprazoleTan JayNo ratings yet
- Child Care What If Child Becomes Sick FlowchartDocument1 pageChild Care What If Child Becomes Sick FlowcharthmareidNo ratings yet
- Sri Ramachandra University SRMC & Ri Department OF Obstetrics AND Gynaecology List OF Equipments AND Instruments (AS PER Mci)Document6 pagesSri Ramachandra University SRMC & Ri Department OF Obstetrics AND Gynaecology List OF Equipments AND Instruments (AS PER Mci)ValarmathiNo ratings yet
- КRОК 2 explained pedDocument41 pagesКRОК 2 explained pedAimeeNo ratings yet
- Blood Functions: Presented by Dr. Khaled Ezam PHD PhysiologyDocument34 pagesBlood Functions: Presented by Dr. Khaled Ezam PHD PhysiologyShrouk EldakroryNo ratings yet
- Surgical MS General Anesthesiology Information PDFDocument10 pagesSurgical MS General Anesthesiology Information PDFjoNo ratings yet
- Lesson 1 IMDG CodeDocument32 pagesLesson 1 IMDG CodeBernard Mamora100% (2)
- Physiological Mechanisms Controlling Cerebral Blood Flow: George Mchedlishvili, M.DDocument9 pagesPhysiological Mechanisms Controlling Cerebral Blood Flow: George Mchedlishvili, M.DinayahNo ratings yet
- Iloilo Chinese Commercial School V FabrigarDocument2 pagesIloilo Chinese Commercial School V FabrigarJohn Erik Kapunan100% (3)
- 7 ImunisasiDocument85 pages7 ImunisasiElfa RiniNo ratings yet
- Pediatrics Physical Diagnosis Form Version 3Document15 pagesPediatrics Physical Diagnosis Form Version 3Stephen Jao Ayala UjanoNo ratings yet
- Research Paper 1 1Document3 pagesResearch Paper 1 1api-665784764No ratings yet
- Co-Inoculation of Bacillus Sp. and Pseudomonas Putida at Different Development Stages Acts As A Bioestimulant To Promote Growth, Yield Ad Nutrient Uptake of TomatoDocument13 pagesCo-Inoculation of Bacillus Sp. and Pseudomonas Putida at Different Development Stages Acts As A Bioestimulant To Promote Growth, Yield Ad Nutrient Uptake of TomatoNayo PalomequeNo ratings yet
- Biological Psychology Notes - Edexcel (IAL) Psychology A-LevelDocument14 pagesBiological Psychology Notes - Edexcel (IAL) Psychology A-LevelAyse KerimNo ratings yet